 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Improper Use of Child Safety Seats -- Kentucky, 1996Since enactment of the Kentucky child restraint law in 1982, the number of motor-vehicle-occupant deaths among children aged 0-4 years has decreased 37% (1). A substantial proportion of this decline is attributed to the increased use of child safety seats (CSSs); in 1995, use of CSSs in Kentucky was 72% (2). In 1996 in the United States, although approximately 85% of infants and 60% of children aged 0-4 years were restrained, approximately 80% of CSSs were used improperly (3). The effectiveness of CSSs in preventing death and injury is reduced when they are used incorrectly (4,5). To estimate the rate for improper use of CSSs, the Kentucky Injury Prevention and Research Center analyzed data from observations and inspections of vehicles entering the main community shopping center parking lot during 1 day in each of two rural counties. This report summarizes the results of this study, which indicate that most children in CSSs were restrained improperly. In both counties, an inspection area was set up within the parking lot, and two observers were placed at the entrance; other entrances were closed by traffic safety cones. Observers completed a survey form for each vehicle containing an occupant appearing to be aged less than or equal to 4 years, and every other vehicle with an occupant appearing to be aged less than or equal to 4 years was asked to participate in the interview/inspection process. When a driver agreed to participate, a consent form was signed and one researcher interviewed the driver and a second inspected the CSS. Interviews consisted of 16 questions related to the driver, the CSS, and the reason for the trip. Inspections addressed the type of CSS, position(s) of child(ren) in the vehicle, type of vehicle, and whether the CSS was used properly. A total of 232 motor vehicles with an occupant aged less than or equal to 4 years were observed at the two sites. Of the 116 vehicles that were eligible for interview/inspection, 77 (66%) drivers agreed to participate. There were 87 child occupants in the 77 vehicles; 62 (81%) of the drivers were female, and 54 (70%) of the drivers were mothers of the children. Of the 87 children, 69 (79%) were restrained, and 17 (20%) were restrained properly; 14 (16%) of the children were unrestrained. The restraint status of the remaining four children was undetermined because they were unrestrained at the time of inspection; although the adult occupants reported the children had been restrained before the inspection and interview, these four were not included in the analysis. A total of 73 instances of improper use were observed among the 52 improperly restrained children. A substantially greater percentage of these errors occurred with the use of convertible CSSs (e.g., a seat that can be used for both infants and toddlers; backward facing for infants aged less than 12 months and weighing less than 20 lbs, and forward facing for children aged greater than or equal to 12 months and weighing 20-40 lbs). Within this category, 22 (42%) errors involved the harness, and 19 (37%) involved misuse of the harness retainer (chest) clip (Figure_1). Of the 42 drivers who had improperly restrained children as occupants, 28 (67%) reported having learned how to use the device by reading the accompanying instructions. Nine (21%) reported having learned through the process of trial and error, and five (12%) reported having learned through demonstration. The 83 children with known restraint status were distributed into three age categories: aged less than or equal to 12 months (n=19), aged 13-24 months (n=29), and aged greater than 24 months (n=36). For three (4%) children, ages were not recorded on the interview form. Children aged less than or equal to 12 months had the lowest percentage (15%) of improper use (referent group). Compared with children aged less than or equal to 12 months, those aged 13-24 months were four times more likely to be restrained improperly (odds ratio=4.0, p=0.06). Among children aged 13-24 months, 90% were restrained improperly, followed by children aged greater than 24 months (69%) and children aged less than or equal to 12 months (68%). Reported by: C Spurlock, PhD, P Kidd, PhD, J Mays, MPH, R McCool, MS, J Buckner, R Clatos, J Rochussen, Kentucky Injury Prevention and Research Center, Lexington; RC Leach, MD, Kentucky Dept for Public Health. Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control, CDC. Editorial NoteEditorial Note: The findings in this report indicate that although most children were restrained in a CSS, three fourths were restrained improperly. Previous studies have documented similar proportions of improper restraint (5,6). Concern about the proper use of CSSs was prompted by the relation between CSS use and air bag-related injuries to children (7). Children aged 13-24 months who used convertible CSSs were most likely to be restrained improperly. Infant CSSs may be easier to use correctly than are convertible CSSs. In addition, more instruction may be available for infant seats than for convertible CSSs. A previous study documented a 46% decrease in misuse of CSSs when personal instruction was given (8). Because children aged 13-24 months are no longer passive infants and may protest vigorously about being restrained, the risk for CSS errors or the lack of restraint may be increased. As a result, caregivers must be firm in their resolve to have children restrained properly. Because the developmental characteristics of children cannot be changed, prevention efforts must focus on changing the behavior of caregivers. The findings in this report are subject to at least two limitations. First, only 66% of eligible drivers participated in the survey; therefore, the findings may not be representative of all child restraint use. Second, eligibility was determined by the physical appearance of the child. As a result, some children may have been missed who appeared to be aged greater than 4 years. At least five strategies exist for increasing the proper use of CSSs. First, encouraging proper use of CSSs should combine health education and law enforcement (9). For example, law enforcement officers could issue citations for improper use, but fines could be waived if the caregiver attended an educational class on proper use and then demonstrated the capability of using the device properly. Second, at the 12-month well-child examination, health-care providers could assess the child for weight and ability to make the transition from an infant CSS to a convertible CSS, or to use the convertible seat in the position for an older child. The caregiver could bring the CSS and vehicle most frequently used to the examination site, and the health-care provider could explain and demonstrate proper use. Third, targeted educational strategies are needed for groups at highest risk. This will require better documentation of the characteristics of the misuse and resulting injuries to child passengers. Fourth, local health departments and others could offer training in the proper use of CSSs at areas frequented by toddlers and their caregivers (e.g., fast-food restaurants, day care centers, and church-affiliated child-care programs). Finally, improved engineering could make CSSs easier to use. In addition, efforts to improve automobiles so that rear seats are equipped with universal attachments for CSSs should continue (10 ). All 50 states have legislation that mandates restraint use for children aged less than 4 years. The adoption of this legislation has been associated with declines in motor-vehicle- related deaths among children in this age group. To continue this decline, prevention efforts now must focus on the proper use of these CSSs to maximize their life-saving potential. References
Figure_1 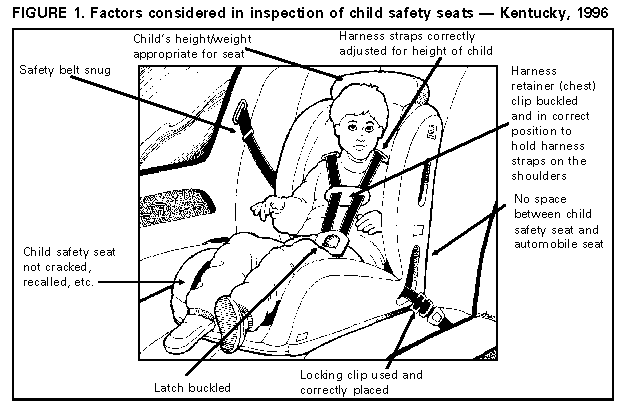 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}