 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Eradication of Poliomyelitis, 1997In 1988, the World Health Assembly adopted the goal of eradicating poliomyelitis by 2000 (1). Substantial progress toward this goal has been reported from many areas of the world (2). Since 1988, all but four countries with endemic polio have conducted National Immunization Days * (NIDs), and most countries have established sensitive surveillance systems for acute flaccid paralysis (AFP). This report updates progress toward global polio eradication in 1997 based on data available from the World Health Organization (WHO) as of May 18, 1998. PROGRESS IN IMPLEMENTING STRATEGIES Routine vaccination Global coverage with three doses of oral poliovirus vaccine (OPV3) among infants was 73% in 1988 and was 81% during 1996-1997 (Figure_1). OPV3 coverage remains lowest in the African Region (AFR) (54% in 1996); however, OPV3 coverage was greater than 50% for the first time in 1996. Supplementary vaccination During 1997, approximately 450 million children aged less than 5 years in 80 countries were vaccinated during NIDs. As of May 1998, NIDs have been conducted in every country with endemic polio, including all countries in Asia, Europe, and Africa (except the Democratic Republic of Congo {DR Congo}, Liberia, Sierra Leone, and Somalia). NIDs are planned during 1998 in DR Congo, Sierra Leone, Somalia, and possibly Liberia. Initiatives to coordinate NIDs across national and regional borders continued in 1997. For the third consecutive year, in April and May 1997, "Operation MECACAR" synchronized NIDs in 19 countries of the European Region (EUR) and Eastern Mediterranean Region (EMR) (including the Russian Federation) and achieved OPV3 coverage of greater than 90% (60 million children). During December 1997, eight countries in the South East Asian Region (SEAR) coordinated NIDs to vaccinate 190 million children during a 1-week period. Reported OPV3 coverage was greater than 85% in Afghanistan and greater than 90% in Bangladesh, India, and Pakistan. NIDs in India reached 134 million children in 1 day during December 1997. Mopping-up vaccination Targeted supplementary house-to-house vaccination activities ("mopping-up campaigns") were conducted in high-risk areas (areas identified as potential or known foci of continued poliovirus transmission based on surveillance for AFP). During May-June 1997, mopping-up vaccination targeted approximately 1.1 million children aged less than 5 years living in the Mekong River area of Cambodia and Vietnam and in parts of Laos. AFP surveillance AFP surveillance ** requires detection, investigation, and reporting of AFP cases among children aged less than 15 years. AFP surveillance is monitored by two main performance indicators: 1) the sensitivity of AFP reporting (target: nonpolio AFP rate of more than one case per 100,000 children aged less than 15 years); and 2) the completeness of specimen collection (i.e., two adequate stool specimens from greater than 80% of persons with AFP). From 1996 to 1997, the global rate of nonpolio AFP increased from 0.6 to 0.8 (Table_1), and rates of more than one were reported in EUR and the Western Pacific Region (WPR). AFP reporting improved in EMR and SEAR (Figure_2, Table_1). In 1997, the proportion of AFP cases with adequate specimens was 65% worldwide, with substantial regional variations (Table_1). In 1997, AFP surveillance was established in several countries (e.g., Afghanistan and many sub-Saharan African countries), and case-based AFP reporting was introduced in India. AFP surveillance has not been initiated in 10 African countries (Burundi, Congo, Equatorial Guinea, Eritrea, Gabon, Gambia, Liberia, Mauritius, Rwanda, and Sierra Leone). Laboratory network The Global Polio Laboratory Network comprises 67 national, 14 regional, and six specialized laboratories (3). In 1997, WHO initiated a process to formally accredit each laboratory. In April 1998, a total of 46 of 67 national laboratories were reviewed; of these, 28 (61%) were accredited, 11 (24%) received provisional accreditation, and seven (15%) failed. IMPACT OF STRATEGIES ON POLIO INCIDENCE As of 1998, a total of 4116 polio cases with onset during 1997 were reported worldwide. Data for 1997 are not complete, mainly because of incomplete and delayed reporting from Africa. Although the 1997 total exceeds the number of cases confirmed in 1996 (4074), a direct comparison is difficult because AFP reporting has improved substantially in 1997. Compared with 1988, when the global eradication goal was established, the number of reported cases declined by 89%. In AFR, the impact of supplementary vaccination and the change in incidence from 1996 to 1997 is difficult to measure because 1997 surveillance data are incomplete (Table_1). However, two large poliovirus reservoirs remain, one each in DR Congo and Nigeria. In EMR, the number of reported polio cases increased from 532 in 1996 to 1023 in 1997, primarily because of improved surveillance and outbreaks in Pakistan. In Egypt, the number of reported cases decreased from 100 in 1996 to 14 in 1997, despite improvements in surveillance for AFP. In EUR, the number of reported polio cases decreased from 193 in 1996 to seven in 1997. Except for one clinically confirmed case in Tajikistan, all cases in 1997 were confirmed by poliovirus isolation and were confined to southeastern Turkey. In SEAR, the number of reported polio cases increased from 1203 in 1996 to 2858 in 1997, primarily reflecting improved surveillance in India and a large outbreak of 751 cases in Uttar Pradesh. AFP reporting improved in most other countries in SEAR, with increases in the number of clinically confirmed cases from 1996 to 1997 in Bangladesh (97 to 191), India (1005 to 2074), Indonesia (77 to 507), Myanmar (eight to 55), and Thailand (one to 19). In 1997, wild polioviruses were isolated from four countries in SEAR (Bangladesh, India, Nepal, and Thailand). In WPR, nine virologically confirmed cases were reported from the Mekong Delta area of Cambodia and Vietnam. The last case reported from WPR occurred in March 1997 near Phnom Penh in Cambodia. Reported by: Global Program for Vaccines and Immunization, World Health Organization, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Vaccine-Preventable Disease Eradication Div, National Immunization Program, CDC. Editorial NoteEditorial Note: Since 1988, substantial progress in polio eradication has been reported from all six WHO regions (2). In 1997, several factors contributed to this progress, including 1) widespread use of NIDs and mopping-up campaigns, 2) accreditation by WHO of 28 national polio laboratories, 3) establishment of sensitive surveillance systems in virtually all countries with endemic polio, and 4) expansion of the "Kick Polio out of Africa" campaign (4). In AFR, limited laboratory capacity is a barrier to improved AFP surveillance. Only 13 laboratories in the African laboratory network serve 31 countries, which requires frequent specimen transport between neighboring countries. Poliovirus transmission occurs primarily in southern Asia and sub-Saharan Africa, and transmission is intense in countries with large populations (e.g., Bangladesh, India, and Pakistan in Asia and DR Congo, Ethiopia, and Nigeria in Africa). Except for DR Congo, all countries have initiated NIDs and have reduced poliovirus transmission. However, poliovirus type 2, usually the first serotype to be eliminated once NIDs have started, was isolated in Afghanistan, Benin, India, and Pakistan in 1997, suggesting that large population subgroups remain unvaccinated. Although type 2 virus was detected in only one African country in 1997, virologic surveillance in AFR remains insufficient to document the presence or absence of this virus serotype in most of sub-Saharan Africa. Recent civil wars in Afghanistan, Congo Republic, DR Congo, Sudan, and Tajikistan hinder NIDs and AFP surveillance. Four countries with endemic polio (DR Congo, Liberia, Sierra Leone, and Somalia) have not conducted NIDs and are affected by ongoing conflicts. Interrupting poliovirus transmission in these countries, in which recognized governments are often absent and the provision of international assistance may be difficult, remains a major concern. The costs of polio eradication are shared by countries with endemic polio and the international community. Individual countries provided 80% of the total cost for polio eradication in AMR, and China and Indonesia contributed even higher national shares. However, in developing countries, most of the cost to implement polio eradication strategies will require external funding. An estimated $1 billion, primarily for operational costs of NIDs, vaccine, and surveillance, will be needed for polio eradication from 1998 to 2005; two thirds of these funds are needed during 1998-2000. An international coalition of partners supporting the eradication effort in countries with endemic polio include Rotary International, CDC, United States Agency for International Development (USAID), United Nations Children's Fund (UNICEF), WHO, and the governments of Japan, Great Britain, Denmark, Germany, and others. Progress toward global polio eradication has led to the certification of polio elimination in AMR (5), the probable interruption of poliovirus transmission in WPR (6), the restriction of poliovirus transmission to one country in EUR (7), and the strengthening of national vaccination programs worldwide. However, global eradication requires the cessation of poliovirus transmission everywhere. Fewer than 1000 days remain to reach the 2000 target (8). Success will depend on securing the additional resources to conduct and maintain eradication strategies in the remaining countries with endemic polio and sustained political commitment. References
* Mass campaigns over a short period (days to weeks) in which two doses of oral poliovirus vaccine are administered to all children in the target group, regardless of prior vaccination history, with an interval of 4-6 weeks between doses. ** A confirmed case of polio is defined as AFP and at least one of the following: 1) laboratory confirmed wild poliovirus infection, 2) residual paralysis at 60 days, 3) death, or 4) no follow-up investigation at 60 days. Figure_1 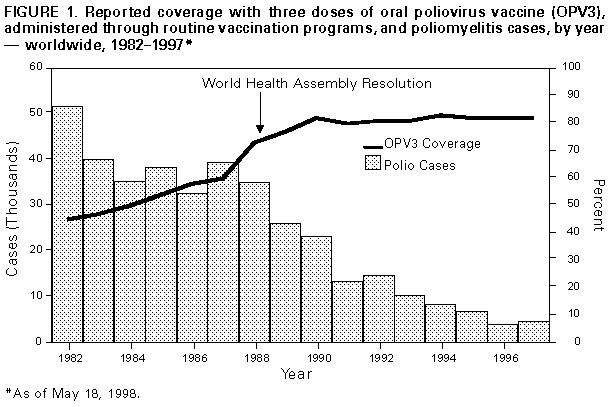 Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Confirmed poliomyelitis cases, acute flaccid paralysis (AFP) surveillance performance indicators, and poliovirus
strain detected, by World Health Organization region *, 1996 and 1997
=======================================================================================================================================================================
Polio cases
% AFP cases ----------------------------------------------------------
No. reported Nonpolio with adequate 1996 1997
AFP cases AFP rate + specimens & -------------------------- -------------------------- Wild polivirus
------------------ ---------------- ---------------- Wild virus- Wild virus- strain detected
Region 1996 1997 1996 1997 1996 1997 Confirmed associated Confirmed associated in 1997
---------------------------------------------------------------------------------------------------------------------------------------------------------------------
AFR 2,377 478 0.15 0.16 -- 24% 1949 ( 0) 219 ( 34) P1/P2/P3
AMR 1,963 1,856 1.20 0.95 76% 74% 0 0 --
EMR 1,775 2,846 0.72 0.97 63% 63% 532 (268) 1023 (261) P1/P2/P3
EUR 1,039 1,596 0.69 1.12 68% 69% 193 ( 86) 7 ( 6) P1
SEAR 1,408 4,581 0.04 0.26 11% 39% 1203 ( 17) 2858 (273) P1/P2/P3
WPR 5,295 5,961 1.17 1.35 79% 84% 197 ( 21) 9 ( 9) P1
Total 13,857 17,318 0.58 0.84 -- 65% 4074 (392) 4116 (583)
---------------------------------------------------------------------------------------------------------------------------------------------------------------------
* The regions are African (AFR), American (AMR), Eastern Mediterranean (EMR), European (EUR), South East Asian (SEAR), and Western
Pacific (WPR).
+ Number of cases of AFP per 100,000 children aged <15 years.
& Two stool specimens that are collected within 14 days of onset of paralysis from a person with AFP and that arrive in the laboratory in
good condition.
=======================================================================================================================================================================
Return to top. Figure_2 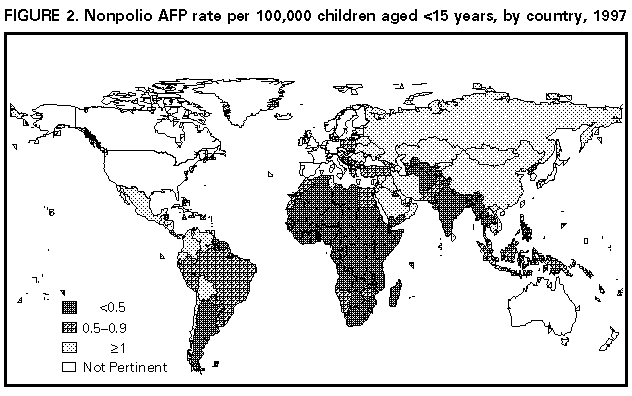 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}