 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Sarcoidosis Among U.S. Navy Enlisted Men, 1965-1993Sarcoidosis is a multisystem granulomatous disease of unknown etiology with highest incidence among young and middle-aged adults. In the United States, the risk for sarcoidosis is substantially higher among blacks than among other races (1,2); however, the reasons for this association are unknown. In response to the occurrence of a case of sarcoidosis in a U.S. Navy (USN) enlisted man, CDC's National Institute for Occupational Safety and Health (NIOSH) analyzed USN data on cases of sarcoidosis diagnosed among active-duty enlisted personnel during 1965-1993. This report summarizes the findings of this analysis, which indicate that the incidence of sarcoidosis declined among USN enlisted men during 1965-1993, particularly among blacks, and that the risk for sarcoidosis was statistically associated with the assignment of USN enlisted men to aircraft carriers. In 1974, a 21-year-old black enlisted man had sarcoidosis diagnosed based on a chest radiograph indicating bilateral hilar adenopathy without parenchymal disease; noncaseating granulomata were present on lymph node biopsy. He had a history of shortness of breath, cough, and chest and joint pain, which he related to his work of grinding antiskid materials from aircraft carrier decks during the preceding 2 years. He received a medical discharge for sarcoidosis in 1975. In 1987, physicians at the U.S. Department of Veterans Affairs diagnosed pneumoconiosis in this patient after mineral-dust deposits were identified in a lung biopsy; the mineral-dust deposits were attributed to the same work exposures aboard the aircraft carrier. In October 1992, the patient asked the USN to request NIOSH to investigate whether his sarcoidosis diagnosis and other cases diagnosed in persons with whom he had served in the USN may have been associated with environmental exposures during their USN service. Because of the possibility of an association between risk for sarcoidosis-like illnesses and environmental exposures during service in the USN and because the underlying cause(s) of sarcoidosis is unknown, in December 1992 the USN requested that NIOSH evaluate the potential relation between sarcoidosis and the USN work environment. NIOSH obtained records from the U.S. Naval Health Research Center (NHRC) for all incident cases of sarcoidosis (defined as diagnosis of "sarcoidosis" by a USN health-care provider) identified among white and black enlisted men while on active duty at any time from 1965 through 1993 * (n=1121). Incidence rates were calculated using age-specific total denominator data for white and black enlisted men on active duty from 1971 through 1993 (denominator data were unavailable for the years before 1971). Numbers for other races were too small for meaningful analysis (no more than three incident cases of sarcoidosis were diagnosed among persons in any other racial category); women were excluded because none had been assigned to aircraft carriers -- an exposure of particular a priori interest -- during 1965-1993. During 1971-1993, the average annual age-specific incidence rate for sarcoidosis declined substantially among USN enlisted black men aged 21-30 years, from 73.3 per 100,000 to 13.2 per 100,000 (Figure_1). Rates for enlisted black men aged 31-40 years declined from 46.5 to 27.8, primarily during 1991-1993. During 1971-1993, rates for USN enlisted white men remained relatively stable. To provide a basis for comparison with cases, a random sample of 10,000 controls was obtained from the NHRC records of enlisted personnel on active duty at any time during 1965-1993; of these, 9040 fulfilled the selection criteria of being men and either white or black. During this period (1965-1993), blacks accounted disproportionately for cases (47.8% of cases versus 11.4% of controls); in addition, USN men with sarcoidosis had served in the USN approximately twice as long as controls (mean tenure was 10.7 years {standard error (SE)=plus or minus 0.2 years} versus 5.5 years {SE=plus or minus 0.1 year}, respectively) and had entered USN service an average of 5 years earlier (1971 {SE=plus or minus 0.3} versus 1976 {SE=plus or minus 0.1}, respectively). Of the enlisted men in whom sarcoidosis had been diagnosed, 27% were discharged within 1 year of diagnosis. Because specific codes for ship type and land assignment were generally not available until 1971, comparisons involving these variables were restricted to the 426 persons classified as cases and 4377 persons classified as controls who entered the USN after that date. Although 70% of case-patients and 66% of controls had ever served on ships, 26% of case-patients and 17% of controls had ever served specifically on aircraft carriers. Additional analyses were conducted to examine the possible association of sarcoidosis with ship service and to control for potential confounders and investigate possible effect modification. For each case, a risk set was created that comprised all persons who had been born during the same 5-year period and who had survived without sarcoidosis beyond the age at which the corresponding case-patient had sarcoidosis diagnosed. Within each risk set, work history in the USN was truncated for persons in the control group when they reached the age at which their corresponding case-patient had sarcoidosis diagnosed. Cox regression with age as the time variable was conducted to examine associations between a USN diagnosis of sarcoidosis and the following variables: race, entry period of USN enlistment, type of ship assignment, and region of country where enlisted. ** Region of enlistment was investigated because previous studies identified it as a predictor of sarcoidosis (1). The analysis indicated a statistically significant increased risk for blacks compared with whites (Table_1) and higher risks in earlier periods of entry, confirming patterns observed in the age-specific incidence rates (Figure_1). No association was identified between increased risk for sarcoidosis and ever having served on a ship; however, a statistically significant association was identified between increased risk for sarcoidosis and ever having served on USN aircraft carriers (risk ratio {RR}=1.5; 95% confidence interval {CI}=1.2-1.9). The RR for aircraft carrier service was higher for blacks (RR=1.7; 95% CI=1.3-2.3) than whites (RR=1.2; 95% CI=0.8-1.7), although the difference between these two RRs was not statistically significant. There was no indication that the risk for sarcoidosis was clustered around any specific aircraft carrier or period of entry. After adjusting for race, aircraft carrier exposure, and year of enlistment, an association was identified between increased risk for sarcoidosis and enlistment from the South Atlantic region (RR=2.1; 95% CI=1.6-2.7) and from the South Central region (RR=1.4; 95% CI=1.1-1.9) compared with the "Other" region. However, the effect of aircraft carrier assignment was neither confounded nor modified by region of enlistment. Reported by: Div of Respiratory Disease Studies, and Div of Surveillance, Hazard Evaluation, and Field Studies, National Institute for Occupational Safety and Health, CDC. Editorial NoteEditorial Note: Sarcoidosis is a multisystem granulomatous disease that typically presents with bilateral hilar lymphadenopathy, diffuse/nodular pulmonary infiltrates, and skin/ocular granulomata. The histology is characterized by noncaseating epithelioid-cell granulomas. Because there are no pathognomonic features, this definition is nonspecific, and sarcoidosis is a diagnosis of exclusion. Although the etiology of sarcoidosis is unknown, the epidemiology of the disease suggests that environmental or infectious agents could be contributory factors (3). For example, manifestations of sarcoidosis are more common during the winter and early spring. Health-care workers are disproportionately affected (4,5), and clusters of cases have been reported both in specific geographic regions (1) and among other occupational groups (e.g., firefighters) (6). Illnesses classified as sarcoidosis may represent a variety of discrete conditions with similar clinical presentations but varying etiologies, and other specific etiologies might be identified for what is currently reported as sarcoidosis. For example, a recent case report suggests an association between exposure to photocopier toner dust and sarcoidosis-like pulmonary disease (7). During the 1940s, several cases of "sarcoidosis" diagnosed among young women in the fluorescent light industry in Salem, Massachusetts, resulted in the recognition of beryllium exposure as a cause of "Salem sarcoid." Chronic beryllium disease is now considered a distinct diagnosis requiring specific immunologic testing (8). The higher risk for sarcoidosis among blacks (1,2) remains unexplained, and possible areas of further investigation include genetic predisposition and disproportionate exposure to environmental risk factors. The limited data in this report indicate substantially higher sarcoidosis incidence rates for blacks than for whites enlisted in the USN and a clear decline in rates for blacks over time. The USN average annual sarcoidosis incidence rates per 100,000 for 1990-1993 (16.0 for black males and 2.5 for white males) were lower than average annual incidence rates for both black males (29.8) and white males (9.6) in a recently studied (1990-1994) population in Detroit, Michigan (2). However, reliable population-based rates over longer periods or for the United States are not available. Reasons for the temporal changes in USN rates are unknown and could reflect unrecognized trends in the total U.S. population. The association of sarcoidosis with earlier entry period into the USN and the decline in incidence rates for blacks over time may indicate that exposures to etiologic factors (possibly including work-related exposures) were higher in the past and differentially affected blacks. The association of sarcoidosis with assignment to aircraft carriers also suggests an occupational factor, although ship assignment is only a crude surrogate for any specific exposures that might be causally related to the disease. However, secular changes in population characteristics, diagnostic and medical screening procedures, and case definition and diagnostic criteria may have affected the findings in this report and contributed to the observed decline in incidence of sarcoidosis. Such factors are particularly important for a disease such as sarcoidosis, which may be asymptomatic and remain undetected for long periods (9,10). In recent years, the USN has reduced the frequency of routine chest radiographs for enlisted personnel, which could explain some of the decline in sarcoidosis incidence rates over time but should not differentially affect rates for blacks and whites. The excess risk on aircraft carriers also may reflect increased detection rates from more frequent use of routine chest radiographs on aircraft carriers, which have large, well-equipped medical facilities. The findings in this report have been shared with the USN and the Department of Veterans Affairs; both are considering further action. References
* The most recent year for which USN data were complete at the time the NIOSH analysis was started. ** The states of enlistment were divided into four regions: Northeast, South Central, South Atlantic, and Other, with the included states as indicated. Northeast -- Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont. South Central -- Alabama, Arkansas, Kentucky, Louisiana, Mississippi, Oklahoma, Tennessee, and Texas. South Atlantic -- Delaware, District of Columbia, Florida, Georgia, Maryland, North Carolina, South Carolina, Virginia, and West Virginia. Other -- Alaska, Arizona, California, Colorado, Hawaii, Idaho, Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Montana, Nebraska, Nevada, New Mexico, North Dakota, Ohio, Oregon, South Dakota, Utah, Washington, Wisconsin, Wyoming, other U.S. possessions, and non-U.S. possessions. Figure_1 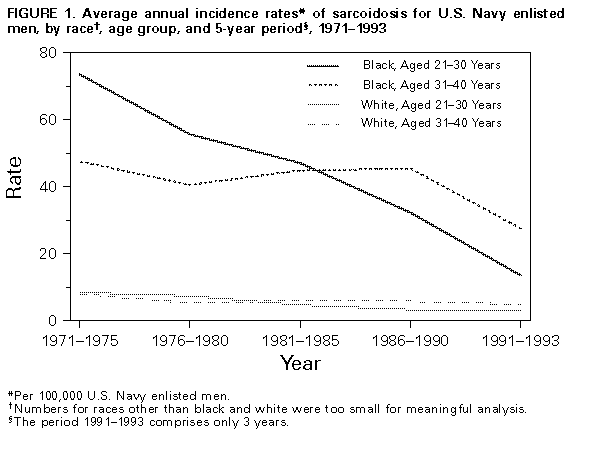 Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size. TABLE 1. Regression analysis for diagnosis of sarcoidosis among U.S. Navy enlisted men who entered the service during 1971-1993 ========================================================================================================== Model variables Estimated coefficient Standard error p value Risk ratio (95% CI *) ---------------------------------------------------------------------------------------------------------- Race + 2.10 (+/-0.10) 0.0001 8.19 (6.7-10.0) Aircraft carrier 0.38 (+/-0.12) 0.00015 1.47 (1.2- 1.9) Entry period 1 & 0.54 (+/-0.37) 0.1417 1.72 (0.8- 3.5) Entry period 2 0.45 (+/-0.35) 0.1983 1.57 (0.8- 3.1) Entry period 3 0.48 (+/-0.31) 0.1271 1.61 (0.9- 3.0) ---------------------------------------------------------------------------------------------------------- * Confidence interval. + The races in this analysis are black and white. Numbers for other racial/ethnic groups were too small for meaningful analysis. & Design variables that compare three time periods of entry to 1987-1993, based on 5-year intervals. Entry period 1=1972-1976; entry period 2=1977-1981; entry period 3=1982-1986. ========================================================================================================== Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}