 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
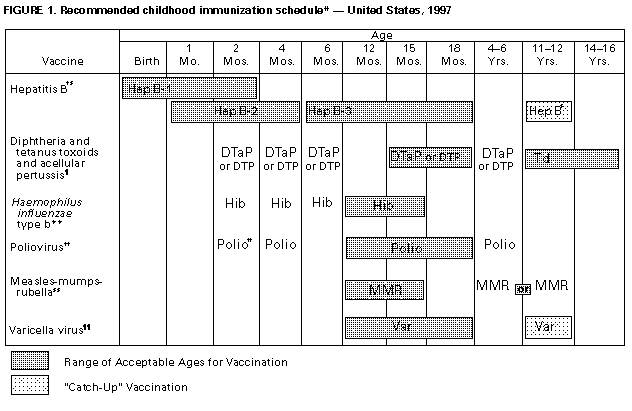
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Notice to Readers Recommended Childhood Immunization Schedule -- United States, 1997Since publication of the recommended childhood immunization schedule in July 1996 (1), the Advisory Committee on Immunization Practices (ACIP), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP) have made important changes in recommendations for preventing pertussis and poliomyelitis (Figure_1A) (Figure_1B). Following the licensure of two acellular pertussis vaccines for infants, the advisory groups now recommend use of acellular pertussis vaccine (Tripedia{Registered}
Since 1992, two DTaP vaccines, ACEL-IMUNE{Registered} and Tripedia{Registered}, have been licensed for use as the fourth and fifth doses of diphtheria and tetanus toxoids and pertussis vaccine (DTP) in children aged 15 months-6 years. In 1995, data became available about the clinical protection conferred by acellular pertussis vaccines when administered to young infants. Multiple controlled trials conducted in Europe demonstrated that, when administered to infants beginning at age 2 months, the protective efficacy of acellular pertussis vaccines was similar to the expected range for most whole-cell vaccines (70%-90%) and these vaccines were associated with fewer local reactions, fevers, and other systemic adverse events than whole-cell pertussis vaccines (2-5). In 1996, the Food and Drug Administration (FDA) licensed two DTaP vaccines, Tripedia{Registered} (July 31) for the initial four doses and ACEL-IMUNE{Registered} (December 30) for all five doses of the DTP vaccination series. As with whole-cell DTP, the first three doses of DTaP are recommended at ages 2, 4, and 6 months. The fourth dose is recommended at age 15-18 months and the fifth dose at age 4-6 years. The fourth dose of DTaP can be administered as early as 12 months of age if at least 6 months have elapsed since receipt of the third dose and if the provider considers the child to be unlikely to return at age 15-18 months to receive this dose. DTaP is preferred for all doses of the pertussis vaccination series, but whole-cell pertussis vaccines remain acceptable alternatives. Both Tripedia{Registered} and ACEL-IMUNE{Registered} continue to be recommended for administration of doses four and five to children who have received three doses of whole-cell DTP vaccine and are preferred for these doses. Change in Polio Vaccination Recommendations: Sequential Polio Vaccination Schedule The elimination of wild-virus-associated polio in the Western Hemisphere (6) and the reduced threat of poliovirus importation into the United States because of rapid progress in global polio-eradication efforts have resulted in the most important change in polio vaccination policy since the introduction of OPV in 1961. Since 1980, an average of eight to nine cases of VAPP have been reported annually in the United States, and VAPP has been the only indigenous paralytic polio in this country since 1979. Although the risk for acquiring VAPP is low (about one case per 2.4 million doses distributed or one case per 750,000 children receiving their first dose of OPV), the relative benefits of OPV have diminished, and the risk for VAPP attributable to OPV is now considered less acceptable. Therefore, ACIP, AAP, and AAFP now recommend a greater reliance on IPV, with a transition policy that will increase use of IPV and decrease use of OPV during the next 3-5 years. ACIP, AAP, and AAFP recommend three options for polio vaccination: sequential administration of IPV and OPV, all IPV, or all OPV. For overall public health benefit, ACIP recommends a sequential schedule of two doses of IPV followed by two doses of OPV for routine childhood vaccination; however, all three polio vaccination options meet acceptable standards of care. Parents should be informed of the benefits and risks associated with each schedule and should choose among them. Implementation of these recommendations should reduce the risk for VAPP and facilitate a transition to exclusive use of IPV following further progress toward global polio eradication. The recommended schedule for sequential IPV/OPV vaccination consists of two doses of IPV administered at ages 2 and 4 months, followed by two doses of OPV, administered at age 12-18 months and at age 4-6 years. If an all IPV schedule is used, the timing of doses is the same as for the sequential schedule (i.e., 2 months, 4 months, 12-18 months, and 4-6 years of age). If an all OPV schedule is used, the first two doses are recommended at ages 2 and 4 months, the third dose at age 6-18 months, and the fourth dose at age 4-6 years. Licensure of New Combination Vaccines Two new combination vaccines have recently been licensed. On September 27, 1996, FDA licensed one Hib conjugate vaccine (Act-HIB{Registered} ****) reconstituted with Tripedia{Registered} for the fourth dose of the DTP and Hib vaccination series. This vaccine is not licensed for the primary three-dose series; children receiving the primary series should either be vaccinated simultaneously with DTaP and Hib vaccines or with combined whole-cell DTP-Hib vaccine. ***** A combination Hib and hepatitis B vaccine (ComVax{Registered} ******) was licensed on October 2, 1996. The vaccine is routinely recommended at ages 2, 4, and 12-15 months and constitutes a complete series of Hib and hepatitis B vaccines. As with other licensed combination products, these vaccines may be used whenever administration of all vaccine components is indicated. Use of combination vaccines may reduce the number of injections required at a single visit. Detailed recommendations about the use of vaccines are available from the manufacturers' package inserts, the 1994 Red Book (7), or the vaccine-specific ACIP statements. References
+-------------------------------------------------------------------
---+
|
|
|
|
| Erratum: Vol. 46, No. 2
|
| =======================
|
| SOURCE: MMWR 46(10);227 DATE: Mar 14, 1997
|
|
|
| In the Notice to Readers "Recommended Childhood
Immunization |
| Schedule -- United States, 1997," in the double asterisk
footnote |
| on page 39, the manufacturer of the HbOC component of Tetramune
|
| was incorrect. Instead of Praxis Biologics, the manufacturer
|
| should have been listed as Lederle Laboratories, Inc., Division
|
| of American Cyanamid (Pearl River, New York).
|
|
|
+-------------------------------------------------------------------
---+ Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}