 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Malaria Surveillance -- United States, 1993Lawrence M. Barat, M.D., M.P.H. Jane R. Zucker, M.D., M.Sc. Ann M. Barber Monica E. Parise, M.D. Lynn A. Paxton, M.D., M.P.H. Jacqueline M. Roberts, M.S. Carlos C. Campbell, M.D., M.P.H. Division of Parasitic Diseases National Center for Infectious Diseases Abstract Problem/Condition: Malaria is caused by infection with one of four species of Plasmodium (P. falciparum, P. vivax, P. ovale, and P. malariae), which are transmitted by the bite of an infective female Anopheles sp. mosquito. Most malaria cases in the United States occur among persons who have traveled to areas (i.e., other countries) in which disease transmission is ongoing. However, cases are transmitted occasionally through exposure to infected blood products, by congenital transmission, or by local mosquito-borne transmission. Malaria surveillance is conducted to identify episodes of local transmission and to guide prevention recommendations. Reporting Period Covered: Cases with onset of illness during 1993. Description of System: Malaria cases confirmed by blood smear are reported to local and/or state health departments by health-care providers and/or laboratories. Case investigations are conducted by local and/or state health departments, and the reports are transmitted to CDC. Results: CDC received reports of 1,275 cases of malaria in persons in the United States and its territories who had onset of symptoms during 1993; this number represented a 40% increase over the 910 malaria cases reported for 1992. P. vivax, P. falciparum, P. ovale, and P. malariae were identified in 52%, 36%, 4%, and 3% of cases, respectively. The species was not determined in the remaining 5% of cases. The 278 malaria cases in U.S. military personnel represented the largest number of such cases since 1972; 234 of these cases were diagnosed in persons returning from deployment in Somalia during Operation Restore Hope. In New York City, the number of reported cases increased from one in 1992 to 130 in 1993. The number of malaria cases acquired in Africa by U.S. civilians increased by 45% from 1992; of these, 34% had been acquired in Nigeria. The 45% increase primarily reflected cases reported by New York City. Of U.S. civilians who acquired malaria during travel, 75% had not used a chemoprophylactic regimen recommended by CDC for the area in which they had traveled. Eleven cases of malaria had been acquired in the United States: of these cases, five were congenital; three were induced; and three were cryptic, including two cases that were probably locally acquired mosquito-borne infections. Eight deaths were associated with malarial infection. Interpretation: The increase in the reported number of malaria cases was attributed to a) the number of infections acquired during military deployment in Somalia and b) complete reporting for the first time of cases from New York City. Actions Taken: Investigations were conducted to collect detailed information concerning the eight fatal cases and the 11 cases acquired in the United States. Malaria prevention guidelines were updated and disseminated to health-care providers. Persons who have a fever or influenza-like illness after returning from a malarious area should seek medical care, regardless of whether they took antimalarial chemoprophylaxis during their stay. The medical evaluation should include a blood smear examination for malaria. Malaria can be fatal if not diagnosed and treated rapidly. Recommendations concerning prevention and treatment of malaria can be obtained from CDC. INTRODUCTION Malaria is caused by infection with one of four species of Plasmodium (P. vivax, P. falciparum, P. ovale, and P. malariae). Infection is transmitted by the bite of an infective female Anopheles sp. mosquito. Forty percent of the world's population live in areas where malaria is transmitted (e.g., parts of Africa, Asia, Central America, Hispaniola, North America, Oceania, and South America). In the past, malaria was endemic throughout much of the continental United States. During the late 1940s, a combination of improving socioeconomic conditions, water management, vector-control efforts, and case management was successful at interrupting malaria transmission in the United States (1). Since then, malaria case surveillance has been maintained to detect locally acquired cases that could indicate reintroduction of mosquito-borne transmission. Through 1993, almost all cases of malaria diagnosed in the United States were imported from regions of the world where malaria transmission was known to occur. Each year, a few congenital infections and infections resulting from exposure to infected blood and blood products have been acquired in the United States. In addition, outbreaks of malaria that were probably acquired through local mosquito-borne transmission were identified during 1989-1992 (i.e., California, outbreaks in 1988, 1989, and 1990; Florida, 1990; and New Jersey, 1991) (2-4). State and/or local health departments and CDC thoroughly investigate all malaria cases acquired in the United States, and CDC conducts an analysis of all imported malaria cases to detect trends in acquisition. This information has been used to guide recommendations for preventing malaria among persons who travel abroad. For example, an increase in P. falciparum malaria among travelers returning from Africa, an area with increasing incidence of chloroquine-resistance, prompted CDC in 1990 to change the recommended chemoprophylaxis from chloroquine to mefloquine (5). This report summarizes malaria cases reported to CDC for 1993. METHODS Sources of Data Malaria surveillance is a passive system; cases of blood-slide-confirmed malaria are identified by health-care providers, infection-control practitioners, and/or laboratories. A slide-confirmed case is reported to local and/or state health departments, and a standard form that contains clinical, laboratory, and epidemiologic information is completed. This information is transmitted to the state health department and then to CDC. CDC staff review all report forms at the time of receipt and request additional information if necessary (e.g., if no recent travel is reported or chemoprophylaxis failure is suspected). CDC directly obtains reports of other cases from health-care providers who request assistance with the diagnosis and treatment of malaria. In addition, records of CDC's National Malaria Reference Laboratory are reviewed, and case report forms are completed for all patients who have smear-positive infection that have not already been reported. All cases that have been acquired in the United States are fully investigated, including all induced and congenital cases and possible introduced or cryptic cases. Information derived from uniform case report forms concerning all slide-confirmed cases is entered into a computer data base and analyzed annually. Definition of Terms The following definitions are used in this report:
This report also uses terminology derived from the recommendations of the World Health Organization (WHO) (6). Definitions of the following terms are included for reference.
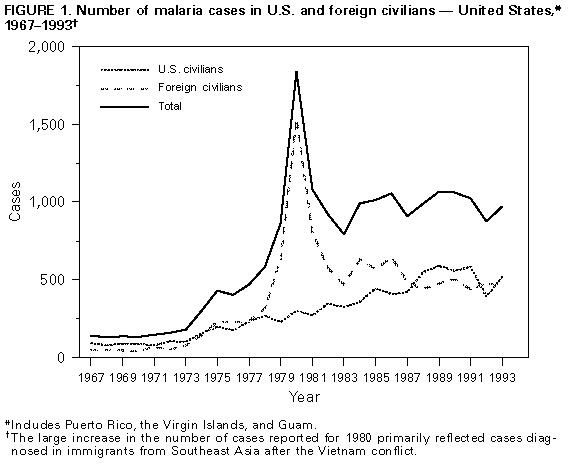
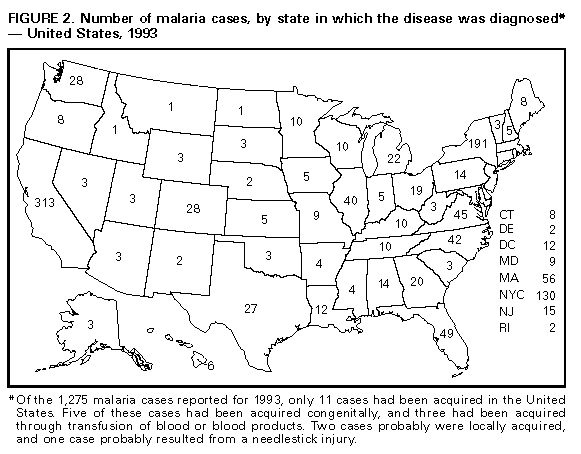
Microscopic Diagnosis of Malaria The early diagnosis of malaria requires that physicians consider malaria in the differential diagnosis of every patient who has an unexplained fever; the evaluation of such patients should include taking a comprehensive travel history. If malaria is suspected, a Giemsa-stained smear of the patient's peripheral blood should be examined for parasites. Thick and thin blood smears must be prepared properly because the accuracy of diagnosis depends on the quality of the blood film and the experience of the laboratory personnel. (See Appendix for proper procedures necessary for accurately diagnosing malaria.) RESULTS General Surveillance CDC received reports of 1,275 malaria cases that had onset of symptoms during 1993 among persons in the United States and its territories. This represented a 40% increase over the 910 cases of malaria reported for 1992 and was the highest total number of cases reported to CDC since 1980 (7). In 1993, 11 of the 1,275 cases had been acquired in the United States. Since 1973, malaria in civilians has accounted for most cases reported to CDC (Table_1). During 1993, 519 (41%) reported cases of malaria were diagnosed in U.S. civilians, representing a 31% increase from the 394 cases reported for 1992 (Figure_1). The 453 (36%) malaria cases in foreign civilians constitutes a 6% decrease from the 481 cases reported for 1992. For each year from 1975 through 1992, malaria cases in U.S. military personnel accounted for no more than 5% of reported cases. In 1993, however, malaria in U.S. military personnel accounted for 278 (22%) reported cases, representing an almost tenfold increase over the 29 cases reported for 1992. Plasmodium Species The Plasmodium species was identified in 1,216 (95%) of the 1,275 cases reported for 1993. P. vivax was identified from blood smears in 663 (52%) cases, representing a 43% increase from the 463 cases for 1992 (Table_2). The 457 (36%) P. falciparum cases identified during 1993 represented a 54% increase from the 296 cases reported for 1992. P. malariae and P. ovale were identified in 53 (4%) and 41 (3%) of cases, respectively. Two mixed infections were reported. The species was undetermined in 59 (5%) cases. Area of Acquisition and of Diagnosis The number of malaria infections acquired in Africa during 1993 (745 {58%} cases) was more than twice the number of cases acquired there during 1992 (337 {37%} cases) (Table_3). Of cases reported for 1993, 259 (20%) cases had been acquired in Asia, representing a 22% decrease from the 330 (36%) cases for 1992. In the United States, cases are reported by the state in which they are diagnosed (Figure_2). The number of cases reported from New York State (excluding New York City) increased from 77 in 1992 to 191 in 1993; this increase primarily reflected the 107 cases diagnosed in military personnel returning from Somalia. The number of cases in North Carolina decreased from 85 in 1992 to 42 in 1993; this decrease primarily reflected a decrease in the number of cases in Montagnard refugees arriving in the state. In addition, New York City began submitting case reports to CDC in 1993. One hundred thirty cases were reported from New York City for 1993, compared with one case for 1992. Interval Between Arrival and Onset of Illness Of those persons who became ill with malaria after arriving in the United States, the interval between the dates of arrival and the onset of illness was known for 847 persons. The species was not identified for 37 of the 847 cases, and one case was a mixed infection. Of the remaining 809 cases caused by a single infecting Plasmodium species, symptoms developed within 30 days after the person's arrival in the United States in 278 (88%) of 316 P. falciparum infections and in 84 (20%) of 431 P. vivax infections (Table_4). Nineteen (2%) of these 809 infected persons became ill greater than 1 year after arrival in the United States. Another 58 persons reportedly became ill from 1 to 163 days before arrival in the United States. Thirty-six (62%) of these 58 persons became ill within a week before arrival in the United States. Imported Malaria Cases Imported Malaria in Military Personnel For 1993, 278 reported cases of imported malaria occurred in U.S. military personnel. Of these cases, 161 (58%) occurred in personnel of the U.S. Army; 100 (36%), the U.S. Marine Corps; and nine (3%), the U.S. Air Force. Eight (3%) cases occurred in military personnel for whom the service branch was not identified. Of the total 278 cases, 234 (84%) were acquired in Somalia during Operation Restore Hope (8). P. vivax was the infecting species in 215 (92%) of these 234 cases, all of which were considered relapse infections; P. falciparum was the infecting species in 10 (4%) cases. Of the remaining 44 (16%) cases reported in U.S. military personnel, 20 had been acquired in Honduras. Imported Malaria In Civilians Of the 961 imported malaria cases in civilians, 508 (53%) were diagnosed in U.S. residents and 453 (47%) were in residents of other countries (Table_5). Of the 508 imported malaria cases in U.S. civilians, 276 (54%) occurred in persons who had traveled in Africa, representing a 45% increase over the 190 cases acquired in this region during 1992. Ninety-five (34%) of the 276 U.S. civilians who acquired malaria in Africa reported having traveled in Nigeria, and 100 (36%) had traveled in other parts of West Africa. Of the 453 cases of imported malaria in foreign civilians during 1993, 213 (47%) had been acquired in Africa; in comparison, 142 cases had been acquired in Africa during 1992. The 157 (35%) cases of imported malaria acquired during 1993 in Asia by foreign civilians represented a 33% decrease from the 233 cases acquired in Asia during 1992. Use of Antimalarial Chemoprophylaxis Information concerning use of chemoprophylaxis was available for 482 (95%) of the 508 U.S. civilians who had imported malaria. Of these 482 persons, 229 (48%) had not taken chemoprophylaxis, 116 (24%) had not taken a drug recommended by CDC for the area visited, and 28 (6%) did not specify the type of chemoprophylaxis taken (9). The remaining 109 (23%) persons reported having taken a medication recommended by CDC for the area visited; however, 23 (21%) of these persons had not taken the recommended dosage, and information was incomplete for 18 (17%). Fifty-seven (52%) of these 109 cases were clinically consistent with relapses of P. vivax or P. ovale infection. The remaining 11 cases occurred in persons who reported having been compliant with a regimen of mefloquine. Of these 11 cases, five were diagnosed as P. falciparum infection, three cases of which had been acquired in West Africa. Serum levels of mefloquine were measured on four of the five persons infected with P. falciparum, and none had mefloquine levels adequate to provide protection from blood-stage infection (10). Illnesses in the remaining six persons who had been compliant with a regimen of mefloquine were diagnosed as P. malariae infection 1-2 months after completion of chemoprophylaxis. The purpose of travel to foreign countries with known malaria transmission was reported for 303 (60%) of the 508 U.S. civilians who had imported malaria (Table_6). Of these 303 persons, 63 (21%) had traveled to visit friends and relatives, 61 (20%) had been tourists, and 56 (18%) had been conducting missionary work. Malaria Acquired in the United States Congenital Malaria The following five cases of congenital malaria were reported for 1993. Case 1. On January 6, 1993, a 3-week-old girl was admitted to a hospital in California because of fever. An examination of the infant's peripheral blood smear demonstrated the presence of P. vivax parasites. She was successfully treated with chloroquine. The infant also received primaquine, although congenital infection does not result in liver stage infection and, therefore, does not require such treatment for radical cure. The infant's mother, a resident of Tijuana, Mexico, had traveled in Guatemala from December 1991 through January 1992. She had treated herself with an unknown medication for malaria while in Guatemala. On December 21, 1992, while visiting in California, she was admitted to a hospital, where she was diagnosed as having P. vivax malaria and treatment with chloroquine was initiated. The infant was born on December 22. After the delivery, the mother was treated with primaquine. Case 2. In June 1993, an 18-day-old boy was admitted to a hospital in California because of fever, anemia, and thrombocytopenia. An examination of the infant's blood smears demonstrated the presence of P. vivax. The symptoms and parasitemia resolved after treatment with chloroquine. The infant's mother had arrived recently from Guatemala, where she had been treated for malaria during the first and seventh months of this pregnancy but had not received chemoprophylaxis for prevention of relapses during the remainder of the pregnancy. Blood smears obtained from the mother after diagnosis of the infant's infection reportedly demonstrated a dual infection with P. vivax and P. malariae; however, the slides were not provided to CDC for confirmation. The mother was treated with chloroquine, but her medical records did not indicate whether she also was treated with primaquine. Case 3. On July 12, 1993, a 7-week-old girl was admitted to a hospital in Florida because of fever, irritability, splenomegaly, anemia, and thrombocytopenia. P. falciparum infection was diagnosed after examination of the infant's blood smear, and she was treated with quinine and pyrimethamine-sulfadoxine. Medical information concerning the infant's mother, who had resided recently in Sierra Leone, was not available. Case 4. During September 1993, a 3-week-old girl was admitted to a hospital in California because of fever. Parasites consistent with P. vivax were present on examination of thick and thin blood smears. The infant was treated with chloroquine and subsequently had resolution of fever and clearance of parasitemia. Symptoms of malaria did not develop in the infant's twin. The infants' mother had traveled from India 11 months before the delivery, and she reported having had febrile episodes during the pregnancy. Indirect immunofluorescent antibody (IFA) assays were performed on serum samples obtained from the mother and both twins. IgG and IgM titers to P. vivax for the parasitemic infant were 1:4,096 and 1:1,024, respectively. Both the mother and the asymptomatic twin had high titers of serum IgG (1:1,024) but low titers of IgM (1:16 in the mother and less than 1:16 in the asymptomatic twin) to P. vivax. The mother was treated with chloroquine and primaquine, and the asymptomatic twin was not treated. Case 5. During November 1993, a 7-week-old girl was admitted to a hospital in Texas because of fever. An examination of her blood smear demonstrated the presence of parasites consistent with P. vivax. The child was treated with chloroquine, and the symptoms and parasitemia resolved. The child had been delivered by cesarean section because of abruptio placentae. The mother had emigrated from India in January 1993 and had been treated for an unspecified type of malaria at 4 months' gestation; she reported no recurrent fevers during her pregnancy. The mother's blood smears were negative for parasites. Treatment information on the mother was unavailable. Cryptic Malaria The following three cases of cryptic malaria were reported for 1993. Cases 1 and 2. The first case occurred in a 27-year-old man who was admitted on both July 20 and August 5, 1993, to a hospital in New York City; both hospitalizations were for fever of unknown origin. On August 17, an examination of smears of a bone marrow aspirate demonstrated the presence of parasites consistent with P. falciparum. The second case occurred in a 22-year-old woman who was admitted to another hospital in New York City on July 21, 1993, because of fever of unknown origin. On August 4, her illness was diagnosed as malaria after an examination of her peripheral blood smear demonstrated the presence of P. falciparum parasites. The man had emigrated from Poland in May 1993 but reported never having traveled to a country with known malaria transmission. The woman had never traveled outside the United States. Neither person had ever received a blood transfusion, used injection drugs, or sustained a needlestick injury. These two persons resided within 2 miles of each other. The New York City Department of Health and CDC (11) investigated both cases and determined that the two patients probably acquired malaria in New York City through mosquito-borne transmission. In addition, a 17-year-old woman who lived within 2 miles of the first two patients was diagnosed on August 4 as having P. falciparum malaria. This case was investigated as a possible case of local mosquito-borne infection; however, the infection was classified as imported malaria because the woman had traveled to Thailand during July 1991. Case 3. On March 29, 1993, fever developed in a 34-year-old woman 2 weeks after she sustained a needlestick injury in the medical office where she was employed. The woman did not seek medical care until April 5, when an examination of her blood smears demonstrated the presence of P. falciparum parasites (8% of her red blood cells were infected). She was treated initially with 1.25 g of mefloquine, 600 mg of quinine, and 900 mg of clindamycin, followed by 250 mg of mefloquine daily for the next 3 days. On April 8, she complained of right upper quadrant pain of unclear etiology, and treatment for malaria was resumed with oral quinine sulfate. She died the next day. The needlestick injury involved a syringe that had been used to obtain blood from a patient who had arrived recently from Africa; blood smears obtained from this patient were reportedly negative for parasites but were unavailable for review by CDC. The woman had traveled several months before to Tijuana and Acapulco, Mexico, which are not considered to be areas with known malaria transmission. She also had traveled in Africa 5 years earlier. Because malarial symptoms developed in the woman within 2 weeks after she sustained the needlestick injury and because she had not traveled recently to an area in which malaria is endemic, the infection could have resulted from the injury; however, a definitive conclusion regarding the source of infection could not determined. Induced Malaria Case 1. In January 1993, illness in a 78-year-old man who had large cell lymphoma was diagnosed at a Connecticut hospital as P. vivax infection. He had never traveled outside the United States, but he had received multiple transfusions of blood and blood products from 63 different donors. On the basis of the results of a survey questionnaire mailed to 59 of these donors, the 29 donors who had ever traveled to an area in which malaria is endemic were tested serologically. One platelet donor had a serum IFA assay titer of 1:256 to P. falciparum, 1:64 to P. vivax, 1:64 to P. ovale, and less than 1:16 to P. malariae on blood obtained on August 31, 1993. An examination of this donor's blood smears demonstrated the presence of P. falciparum parasites. This donor had been born in India, and the last time he had visited there before the platelet donation was in 1987. He again visited India from May through July 1993 (i.e., between the time of the donation and the investigation of this case). Repeat serologic testing on October 14 demonstrated an IFA assay titer of 1:64 for P. falciparum and 1:16,384 for P. vivax, the latter of which was consistent with recent P. vivax infection. An examination of blood smears at that time did not demonstrate the presence of parasites. The donor was treated for both P. vivax and P. falciparum infection. Whether this donor was the source of the recipient's infection is uncertain, because the donor might have acquired malaria during his most recent trip to India. Case 2. On December 21, 1992, a 62-year-old man who had multiple myeloma was admitted to a hospital in New York City because of fever. He was treated initially for presumptive bacterial sepsis, but he continued to have febrile episodes. On January 7, 1993, a bone marrow aspirate was performed, and malaria parasites were identified on microscopic examination. Subsequent examination of his peripheral blood smear confirmed the diagnosis of P. falciparum infection, with a 12% level of parasitemia. He was treated with intravenous quinidine and tetracycline with subsequent resolution of fever and parasitemia. The patient had been born in Russia and had moved to the United States 10 years before the diagnosis of malaria. Two years before the diagnosis, he had vacationed in Cancun, Mexico, although this is not an area with known malaria transmission. He had received two units of packed red blood cells on November 22, 1992, and one unit of packed red blood cells 7 days later. All three of the blood donors were subsequently tested for malaria antibodies; a serum sample from one of these donors had a positive reaction, with an IFA assay titer of greater than 1:16,384 for P. falciparum malaria. The implicated donor was a man who had been born in Nigeria and who had been to both Nigeria and Haiti during September 1992; however, he had not reported this information to the blood bank at the time of the donation. An examination of blood smears obtained from the donor demonstrated parasites consistent with P. falciparum. He was treated with quinine sulfate and pyrimethamine-sulfadoxine. Case 3. In December 1993, a 60-year-old woman who had received a liver transplant the previous month was diagnosed as having P. vivax infection. She was treated successfully with chloroquine and primaquine. She had been born in the United States and had never traveled to an area in which malaria is endemic. She had received 110 units of blood and blood products during her hospitalization for the liver transplantation. Serum was obtained from the liver donor and all donors from whom she had received red blood cells and platelets. Only one platelet donor had detectable antibodies for Plasmodium. The implicated donor was a woman who had emigrated from Ghana in 1990; she had not traveled out of the United States since her arrival. She was asymptomatic at the time of donation. IFA assay titers of her serum were 1:1,024 for P. ovale, 1:1,024 for P. malariae, 1:4,096 for P. falciparum, and 1:256 for P. vivax, a pattern consistent with that of a person from a geographic area in which the incidence of malaria transmission is high. An examination of blood smears obtained from this donor demonstrated rare ring forms consistent with Plasmodium infection, but a definitive species identification was not possible. Another person had received red blood cells from this donor. An IFA assay of this recipient's serum only identified antibodies to P. ovale (titer 1:64), and an examination of this recipient's blood smear did not demonstrate the presence of parasites. This recipient was treated with chloroquine, and the donor was treated with chloroquine and primaquine. A DNA amplification using polymerase chain reaction of blood samples obtained from the donor and the first recipient (i.e., the person with the initially diagnosed infection) identified the infecting species as P. ovale, thus highlighting the limitations of using parasite morphology for species identification -- particularly when differentiating P. vivax and P. ovale. Deaths Attributed to Malaria The following eight deaths were attributed to malaria during 1993. Case 1. A 32-year-old woman in her 35th week of pregnancy came to the United States from Liberia on March 13, 1993. She had had an illness that was diagnosed as malaria in June 1992, for which she was treated with chloroquine and pyrimethamine. Her pregnancy was complicated by preeclampsia. Two days after arrival in the United States, she became ill with myalgia and fever (103 F). She was hospitalized on March 20. An examination of her blood smear demonstrated the presence of parasites consistent with P. falciparum, and treatment with oral quinine sulfate was initiated. On March 21, adult respiratory distress syndrome and hypoglycemia developed in the woman. Two days later, pyrimethamine-sulfadoxine was included in her treatment regimen. Because her respiratory status was deteriorating rapidly, a cesarean section was performed on March 23. The woman's respiratory status continued to worsen, and she died on March 30. The woman's infant girl weighed 2.5 kg and was apparently healthy. Although an examination of placental sections demonstrated the presence of P. falciparum parasites, no parasites were demonstrated on blood smears obtained from the infant on March 24. Case 2. On April 17, 1993, a 51-year-old woman returned from traveling in South Africa and Zimbabwe. She had taken chloroquine for antimalarial chemoprophylaxis while traveling. Fever developed in the woman on April 24, and an examination of the woman's blood smear on April 26 demonstrated the presence of P. falciparum parasites. She was treated with a single dose of 1.5 g of mefloquine on April 27. She continued to have febrile episodes; on April 30, she complained of intense left ear pain and was leukopenic (white blood cell count of 2000/mm3). Doxycycline and norfloxacin were added to her treatment regimen for additional coverage against P. falciparum and bacterial pathogens. The patient had a cardiac arrest and died on April 31. Case 3. A 24-year-old male U.S. resident was working as a volunteer in the jungles of Guyana. He had not been taking antimalarial chemoprophylaxis. On March 29, 1993, he was hospitalized in Guyana because of fever. Detailed information concerning this hospitalization was unavailable. He was airlifted to a hospital in Miami on April 5, at which time he had altered mental status. He died within an hour after his arrival. A postmortem examination indicated cerebral malaria caused by P. falciparum infection. Case 4. On November 11, 1993, a 51-year-old woman returned from a 2-week visit to Nigeria, where she had taken hydroxychloroquine as antimalarial chemoprophylaxis. Fever developed in the woman on November 17, and she was hospitalized the next day. A blood smear obtained from the woman was examined and reported to be negative for parasites. On November 21, she became lethargic and had lactic acidosis. She was transferred to another hospital on November 22, at which time she had altered mental status consistent with cerebral malaria. An examination of her blood smear demonstrated the presence of P. falciparum parasites (4% of her red blood cells were infected). Treatment with intravenous quinidine and oral pyrimethamine-sulfadoxine was initiated at the time of admission. During her hospitalization, she was diagnosed with adult respiratory distress syndrome and required mechanical ventilation. She subsequently acquired nosocomial bacterial pneumonia. She died as a result of respiratory failure on December 15. Case 5. In June 1993, a 63-year-old female native of India traveled to the United States. She had had multiple episodes of malaria that had been treated in India. On August 8, she was admitted to a hospital in Missouri because of fever (100.5 F), nausea, vomiting, and diarrhea. An examination of her blood smears reportedly demonstrated a mixed Plasmodium infection, and she was treated with oral quinine sulfate and doxycycline. The symptoms of her illness improved markedly, and she was discharged 2 days after admission. On August 14, after she had completed a 3-day course of quinine and was on her fourth day of treatment with doxycycline, she was admitted to another hospital because of shortness of breath that required mechanical ventilation. A radiograph of her chest was consistent with pulmonary edema, and an echocardiogram demonstrated diffuse cardiac dysfunction consistent with myocarditis or ischemia. Her cardiac enzymes were normal, excluding the diagnosis of acute myocardial infarction. The patient died as a result of congestive heart failure. Subsequent reexamination by CDC of the initial blood smears from the first hospitalization demonstrated the presence of only P. vivax parasites (1.3% of her red blood cells were infected). The underlying cause of myocardial disease was not determined. Case 6. On January 10, 1993, a 67-year-old woman was admitted to a hospital in Florida because of febrile episodes. An examination of her blood smears demonstrated the presence of P. falciparum parasites. She was treated with quinine sulfate. During her hospitalization, she was diagnosed with adult respiratory distress syndrome and cardiac arrhythmia, the latter of which caused her death on January 20. The arrhythmia may have resulted from either P. falciparum-associated myocardial dysfunction or an adverse reaction to quinine. Case 7. On January 1, 1993, fever developed in a 30-year-old man 1 day after he returned from a trip to Nigeria. He had not taken antimalarial chemoprophylaxis while traveling. He was hospitalized on January 20 because of headache, nausea, and vomiting. His illness was diagnosed initially as viral meningitis, but a subsequent examination of his blood smears identified P. falciparum parasitemia. Treatment with quinine and pyrimethamine-sulfadoxine was initiated. He also was diagnosed as having bacterial pneumonia, which was treated with a cephalosporin antibiotic, and mild renal insufficiency. His temperature decreased with treatment. On January 24, the patient signed out of the hospital against medical advice without completing his prescribed course of quinine. On February 1, he was admitted to another hospital because of respiratory distress. An examination of his blood smears again demonstrated the presence of P. falciparum parasites, and findings on his chest radiograph were consistent with adult respiratory distress syndrome. He was treated with intravenous quinidine, pyrimethamine-sulfadoxine, and clindamycin. His respiratory status did not improve, and he died on February 6. Case 8. See Cryptic Case #3. DISCUSSION The 1,275 cases of malaria reported to CDC for 1993 represented a 40% increase from the 910 cases reported for 1992 (7). This increase was attributed primarily to two events. First, the number of cases in military personnel increased almost tenfold, reflecting the 234 cases of malaria acquired in Somalia during Operation Restore Hope (which occurred from December 1992 through May 1993) (8). This increase represented the largest number of malaria cases in military personnel in 1 year since the peak in cases associated with the return of troops from Vietnam. Second, during 1993, the New York City Department of Health began routinely sending all malaria case report forms to CDC, reporting 130 cases for that year. In comparison with 1992, the number of P. falciparum infections reported for 1993 in U.S. civilians returning from Africa increased by 45%; this overall increase primarily reflected the increased number of cases acquired in Nigeria and other parts of West Africa. Almost all these cases occurred in persons who had not taken a chemoprophylactic regimen recommended by CDC. Failure to take the appropriate antimalarial chemoprophylaxis and noncompliance with dosing regimens contributed to most of the imported malaria cases in U.S. civilians during 1993. Only 25% of U.S. civilians diagnosed with malaria had taken an appropriate chemoprophylactic medication recommended by CDC for their area of travel. The drug recommended by CDC for travelers to areas with known transmission of chloroquine-resistant P. falciparum is mefloquine (9). Excluding cases of relapse infection and cases for which information was incomplete, symptomatic parasitemia developed in only 11 patients who had correctly taken mefloquine for chemoprophylaxis. Serum mefloquine levels were found to be below a protective level for all four of the five patients with P. falciparum infection who were tested. This may indicate noncompliance or differences in metabolism of mefloquine in these persons (10). The remaining six patients had P. malariae parasitemia greater than 2 months after completion of their chemoprophylactic regimen. Health-care providers should contact CDC if chemoprophylaxis failure is suspected, thus enabling measurement of serum levels of the chemoprophylactic agent. The development of malarial infection in the setting of protective levels of mefloquine might indicate the emergence of mefloquine-resistant strains of the parasite. Reported cases of chloroquine-resistant P. falciparum infections in travelers returning from Africa prompted CDC to revise the recommended antimalarial chemoprophylaxis for travelers to that region (5). The signs and symptoms of malarial illness are variable, but most patients experience fever. Other symptoms include headache, back pain, chills, increased sweating, myalgia, nausea, vomiting, diarrhea, and cough. The diagnosis of malaria should be considered for any person who has these symptoms and who has traveled to an area in which malaria is transmitted. Malaria also should be considered in the differential diagnosis of persons who have a fever of unknown origin, regardless of their travel history. Asymptomatic parasitemia can occur among long-term residents of areas in which malaria is endemic. Untreated P. falciparum infection can progress to coma, renal failure, pulmonary edema, and death. During 1993, eight (0.7%) persons who had malaria died. Previously described factors that may have contributed to these deaths included failure to take the recommended antimalarial chemoprophylaxis during travel, delay in seeking medical care, delay in diagnosis and initiation of therapy, and use of suboptimal treatment regimens (12). None of the patients who died during 1993 had taken the appropriate chemoprophylaxis. Failure to identify and aggressively treat major complications also may have contributed to some of these deaths. Treatment for malaria should be initiated immediately after the diagnosis has been confirmed by a positive blood smear. Treatment should be determined on the basis of the infecting Plasmodium species, the parasite density, and the patient's clinical status (10). Although non-falciparum malaria rarely causes severe illness, persons diagnosed as having P. falciparum infection are at risk for developing severe life-threatening complications. The use of intravenous quinidine gluconate and exchange transfusion might be necessary to manage patients who have high levels of parasitemia or severe complications (13). Two malaria cases that occurred in New York City were probably locally acquired from infected Anopheles sp. mosquitoes; these cases represented the seventh outbreak of locally acquired infection in the continental United States during 1989-1993 (11). Local outbreaks were identified twice in San Diego County in 1989 and once in 1990, once in rural Florida in 1990, and twice in suburban New Jersey in 1991 (2-4). The outbreak in 1993 differs from other recent outbreaks in that a) it occurred in an urban setting and b) the infecting organism was P. falciparum. Health-care providers should consider malaria in the differential diagnosis of any patient who has an unexplained fever, regardless of the patient's travel history, and they should conduct a blood smear examination if indicated. To enable prompt investigation of malaria cases in patients who have not traveled to an area in which malaria is endemic, health-care providers should immediately notify their state or local health department and CDC of such cases. Health-care providers are encouraged to consult appropriate sources for malaria treatment recommendations or call CDC's National Center for Infectious Diseases, Division of Parasitic Diseases at (770) 488-7760 (10). Detailed recommendations for preventing malaria are available 24 hours a day from the CDC Malaria Hotline, which can be accessed by telephone ({404} 332-4555), facsimile ({404} 332-4565), or CDC's World-Wide Web server (http://www.cdc.gov/). CDC annually publishes updated recommendations in the Health Information for International Travel (9), which is available through the Superintendent of Documents, U.S. Government Printing Office, Washington, DC 20402-9235; telephone (202) 512-1800. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}