 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
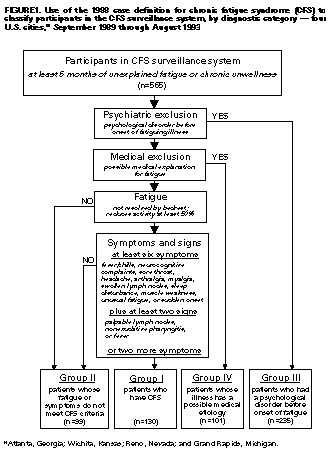
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Chronic Fatigue Syndrome -- Four U.S. Cities, September 1989 Through August 1993Michele Reyes, Ph.D.,1 Howard E. Gary, Jr., Ph.D.,(1) James G. Dobbins, Ph.D.,1 Bonnie Randall, M.C.P.,(2) Lea Steele, Ph.D.,1 Keiji Fukuda, M.D., M.P.H.,(1) Gary P. Holmes, M.D.,1,3 David G. Connell, Ph.D.,(2) Alison C. Mawle, Ph.D.,1 D. Scott Schmid, Ph.D.,(1) John A. Stewart, M.D.,1 Lawrence B. Schonberger, M.D., M.P.H.,(1) Walter J. Gunn, Ph.D.,1,4 William C. Reeves, M.D., M.S.P.H.(1) (1) Division of Viral and Rickettsial Diseases National Center for Infectious Diseases (2) Abt Associates Inc., Cambridge, Massachusetts (3) Texas A & M University Health Science Center, Scott and White Clinic, Temple, Texas (4) Arlington Associates Inc., Lilburn, Georgia Abstract Problem/Condition: Although chronic fatigue syndrome (CFS) has been recognized as a cause of morbidity in the United States, the etiology of CFS is unknown. In addition, information is incomplete concerning the clinical spectrum and prevalence of CFS in the United States. Reporting Period Covered: This report summarizes CFS surveillance data collected in four U.S. cities from September 1989 through August 1993. Description of System: A physician-based surveillance system for CFS was established in four U.S. metropolitan areas: Atlanta, Georgia; Wichita, Kansas; Grand Rapids, Michigan; and Reno, Nevada. The objectives of this surveillance system were to collect descriptive epidemiologic information from patients who had unexplained chronic fatigue, estimate the prevalence and incidence of CFS in defined populations, and describe the clinical course of CFS. Patients aged greater than or equal to 18 years who had had unexplained, debilitating fatigue or chronic unwellness for at least 6 months were referred by their physicians to a designated health professional(s) in their area. Those patients who participated in the surveillance system a) were interviewed by the health professional(s); b) completed a self-administered questionnaire that included their demographic information, medical history, and responses to the Beck Depression Inventory, the Diagnostic Interview Schedule, and the Sickness Impact Profile; c) submitted blood and urine samples for laboratory testing; and d) agreed to a review of their medical records. On the basis of this information, patients were assigned to one of four groups: those whose illnesses met the criteria of the 1988 CFS case definition (Group I); those whose fatigue or symptoms did not meet the criteria for CFS (Group II); those who had had an identifiable psychological disorder before onset of fatigue (Group III); and those who had evidence of other medical conditions that could have caused fatigue (Group IV). Patients assigned to Group III were further evaluated to determine the group to which they would have been assigned had psychological illness not been present. The epidemiologic characteristics of the illness and the frequency of symptoms among patients were evaluated, and the prevalence and incidence of CFS were estimated for each of the areas. Results: Of the 648 patients referred to the CFS surveillance system, 565 (87%) agreed to participate. Of these, 130 (23%) were assigned to Group I; 99 (18%), Group II; 235 (42%), Group III; and 101 (18%), Group IV. Of the 130 CFS patients, 125 (96%) were white and 111 (85%) were women. The mean age of CFS patients at the onset of illness was 30 years, and the mean duration of illness at the time of the interview was 6.7 years. Most (96%) CFS patients had completed high school, and 38% had graduated from college. The median annual household income for CFS patients was $40,000. In the four cities, the age-, sex-, and race-adjusted prevalences of CFS for the 4-year surveillance period ranged from 4.0 to 8.7 per 100,000 population. The age-adjusted 4-year prevalences of CFS among white women ranged from 8.8 to 19.5 per 100,000 population. Interpretation: The results of this surveillance system were similar to those in previously published reports of CFS. Additional studies should be directed toward determining whether the data collected in this surveillance system were subject to selection bias (e.g., education and income levels might have influenced usage of the health-care system, and the populations of these four surveillance sites might not be representative of the U.S. population). Actions Taken: In February 1997, CDC began a large-scale, cross-sectional study at one surveillance site (Wichita) to describe more completely the magnitude and epidemiology of unexplained chronic fatigue and CFS. INTRODUCTION Although chronic fatigue syndrome (CFS) has been recognized as a cause of morbidity in the United States, the etiology of the syndrome is unknown, and only symptomatic treatments are available. No biologic markers of CFS have been identified, and no diagnostic tests have been developed; the illness is diagnosed primarily on the basis of symptoms and signs reported by the patient and exclusion of other possible causes of prolonged, debilitating fatigue. Information is incomplete concerning the characteristics of patients who have unexplained fatigue, their symptoms, and the prevalence of chronic fatigue. Fatigue is a common complaint, and chronic fatigue is a well-known symptom of many physical and psychological illnesses (1,2). CFS patients constitute a subgroup of persons who have chronic fatigue. Outbreaks of similar illnesses were described before the early 1980s (3), when interest in endemic CFS was heightened (4). Several early reports suggested an association between the symptoms and Epstein-Barr virus (EBV), and the illness was referred to as "chronic EBV syndrome" (4-6). Subsequent studies indicated that CFS patients were no more likely than non-CFS patients to have evidence of infection with EBV (7). In 1988, a CFS case definition was published for the purpose of improving comparability across research studies (8). According to this definition, other clinical conditions that might have caused the fatigue must have been excluded. At least six of the following 11 symptoms must have begun at or after the onset of illness and must have persisted or recurred for at least 6 months: mild fever (37.5-38.6 C {99.5-101.5 F}) (as measured by the patient) and/or chills; sore throat; painful lymph nodes; muscular discomfort or myalgia; prolonged (greater than or equal to 24 hours) generalized fatigue after exercise that would have been easily tolerated before the illness; generalized headaches different from those the patient had before the onset of illness; migratory arthralgia without joint swelling or redness; neuropsychologic complaints (e.g., photophobia, transient visual scotomata, forgetfulness, excessive irritability, confusion, difficulty thinking, inability to concentrate, and depression); sleep disturbance; sudden onset of symptoms *; and unexplained generalized muscle weakness. Furthermore, unless eight or more of these symptoms have been present, at least two of the following three physical signs must have been documented by a physician on at least two occasions and at least 1 month apart: low-grade fever (37.6-38.6 C {99.6-101.5 F}), nonexudative pharyngitis, and palpable or tender lymph nodes. Only two peer-reviewed studies have made population-based estimates of the prevalence of a chronic fatiguing illness. The first study, which was conducted in Australia, relied on solicitation of medical-practitioner referrals to identify persons who had had at least 6 months of unexplained prolonged fatigue accompanied by neuropsychiatric dysfunction (9). Using this definition, the researchers estimated the prevalence as 37 cases per 100,000 population. The second study, which was conducted in the United States, was based on data from a nationwide population-based mental health survey of 13,000 persons (10). This latter study used information obtained by administering the Diagnostic Interview Schedule (DIS) (11) to approximate the CFS case definition. Only one case of CFS was identified, for an estimated prevalence of 7.4 cases per 100,000 population. From September 1989 through August 1993, CDC conducted physician-based surveillance for unexplained chronic fatigue in Atlanta, Georgia; Wichita, Kansas; Grand Rapids, Michigan; and Reno, Nevada. The primary objectives of this system were to a) collect descriptive epidemiologic information from patients who had unexplained chronic fatigue, b) estimate the prevalence and incidence of CFS in defined populations, and c) describe the clinical course of CFS. This report addresses the first two objectives. METHODS Surveillance Sites Each of the four surveillance sites comprised a central city and its surrounding counties (12). Wichita and Grand Rapids were chosen because they are cities with stable populations whose overall demographic characteristics approximated those of the total U.S. population. Reno was selected because of its close proximity to Incline Village, the site of a 1986 cluster of CFS cases (4). Atlanta was chosen because of the proximity to CDC for special laboratory studies. Surveillance System Procedures At each surveillance site, physicians whose clientele were likely to include patients who have CFS (i.e., family practitioners, internists, infectious disease specialists, and rheumatologists) were identified by using telephone and medical directories. Of the eligible physicians, 879 were asked to participate in the study; 409 (47%) of these physicians agreed to participate. The site-specific participation rates were 55% in both Wichita and Reno, 45% in Grand Rapids, and 37% in Atlanta (12). The participating physicians were contacted annually to confirm their continued participation and were sent periodic newsletters to inform them of the status of the surveillance system. Two surveillance nurses were designated in each of the four cities. Patients who possibly had CFS were referred by the participating physicians to the surveillance nurses based in that city. Physicians were asked to refer patients aged greater than or equal to 18 years who had had at least 6 months of unexplained debilitating fatigue or chronic unwellness. Debilitating fatigue was defined as the patient's subjective report of reduced activity level and greater effort required to perform the same routine activities as were performed before onset of fatigue. Chronic unwellness was defined as a patient's report of two or more of the following symptoms occurring at least monthly: fever, sore throat, unusual muscle weakness, unusual fatigue after exercise, tender lymph nodes, myalgia, and arthralgia. Those patients who participated in the surveillance system
During the personal interview, the surveillance nurse(s) obtained informed consent from each participant; reviewed the self-administered questionnaire with the patient; and obtained information concerning the onset, frequency, and severity of all symptoms reported by the patient, including symptoms not included in the CFS case definition, self-reported energy levels, and ability to perform everyday activities. Cognitive function was measured by tests of memory, attention, and concentration. The DIS (11) was administered to identify those patients who had psychological illnesses. Only the DIS sections concerning somatization, panic disorder, generalized anxiety disorder, and depression were used. For each patient, a battery of standard blood and urine tests was performed, including a complete blood count, urinalysis, and renal analyses and measurements of erythrocyte sedimentation rate, thyroid function, and liver function. The surveillance nurses reviewed for each patient the medical records maintained by the referring physician and summarized the information regarding the symptoms suggestive of CFS, the laboratory test results, other illnesses and health problems, and hospitalizations. Classification of Participating Patients A physician review committee (PRC), composed of clinicians and researchers, was established for the purpose of classifying the participating patients into one of four groups (Figure_1). The assignment of each patient into one of these groups was decided by at least three members of the PRC and was based on an independent review of the summarized information for each patient. The PRC reviewers unanimously agreed on the initial classification of 82% of all cases reviewed. When the initial classification was not unanimous, PRC members conferred and reached a consensus. CDC then compiled and analyzed the data for each group of patients. The 1988 case definition of CFS (8) was used as the basis for classification of patients. Patients whose illnesses met the criteria of the CFS case definition (i.e., the CFS patients) were assigned to Group I. Patients whose fatigue or symptoms did not meet the criteria for CFS were assigned to Group II. Patients who had evidence of a psychological disorder that was diagnosable before the onset of fatigue and that could have explained the fatiguing illness were assigned to Group III. Patients in this group were further evaluated to determine the group to which they would have been assigned had psychological illness not been present (i.e., Groups III-I, III-II, or III-IV). Patients who had evidence of a medical condition that could have caused fatigue were assigned to Group IV. RESULTS Patients During the 4-year surveillance period from September 1989 through August 1993, participating physicians referred 648 patients who had had unexplained debilitating fatigue or chronic unwellness for at least 6 months. Of these, 565 (87%) patients agreed to participate in the surveillance system, and 83 (13%) declined. The largest percentage of participants was from Atlanta (46%), followed by Wichita (22%), Reno (18%), and Grand Rapids (14%) (Table_1). Characteristics and Classification of Participants Of the 565 patients, 130 (23%) were assigned to Group I; 99 (18%), Group II; 235 (42%), Group III; and 101 (18%), Group IV (Table_1). The distribution of patients by group was similar for all four surveillance sites. The demographic characteristics of patients did not differ significantly by group (Table_2). Most Group I patients were white (96%) and female (85%) and had a median of 14 years of education and a median annual household income of $40,000. The mean age at onset of fatigue for Group I patients was 30 years (range: 15-56 years), and the mean age at the time of the interview was 37 years, resulting in a mean illness duration of 6.7 years. Symptoms and Signs Each symptom and sign listed in the CFS case definition was evaluated to determine the frequency with which it was reported by patients. Each symptom was reported by at least 73% of the 130 Group I patients. However, only 48 (37%) Group I patients reported that the onset of their symptoms occurred suddenly (i.e., in less than 24 hours) (Table_3), and only seven (5%) Group I patients were classified as such on the basis of this criterion in combination with other symptoms and signs. In addition, less than or equal to 32% of Group I patients had documented physical criteria that met the CFS case definition. Symptoms and signs were reported least frequently by Group II patients, although this directly reflected the definition for assignment to this group. Persons who had psychological or medical conditions that possibly explained the fatigue (Groups III and IV, respectively) reported having had more symptoms and signs of CFS than patients in Group II, but fewer symptoms and signs than patients in Group I. Patients assigned to Groups III-I, III-II, and III-IV reported frequencies of symptoms remarkably similar to those of patients in Groups I, II, and IV, respectively. Symptoms not included in the CFS case definition that were reported by patients included shortness of breath, cough, wheezing, nausea, vomiting, constipation, diarrhea, stomach ache, bloating, ringing in the ears, numbness, poor balance, anger, anxiousness, nightmares, night sweats, chest pain, heart palpitations, itchiness, and skin rashes. No one symptom or group of symptoms was reported by greater than 50% of respondents. Group I patients most often reported symptoms not included in the case definition, followed by patients in Groups III and IV; patients in Group II reported such symptoms least often. Prevalence On the basis of 1990 U.S. census data for the counties encompassing each study site, the crude 4-year period prevalence of CFS among persons aged greater than or equal to 18 years ranged from 3.8 cases per 100,000 population in Atlanta to 9.6 per 100,000 in Wichita, with an overall crude rate of 5.2 per 100,000 (Table_4). The differences in prevalence between the surveillance sites remained after directly adjusting for age, sex, and race. Because most patients who had CFS were white (98%) and female (85%), the site-specific period prevalences were calculated for this group. For white women, the crude prevalence rates ranged from 8.6 cases per 100,000 population in Atlanta to 17.7 per 100,000 in Wichita, with an overall crude rate of 10.8 per 100,000 (Table_4). The overall crude prevalence rate for white men was 2.1 per 100,000. Estimates of site-specific prevalence rates for persons of other racial/ethnic groups were not calculated because of the small number of cases. The estimated prevalence of unexplained chronic fatigue was based on the 393 patients who did not have evidence of a medical condition that could have caused fatigue (i.e., patients in Groups I and II and patients in Group III who did not have a medical exclusion). The crude period prevalence of chronic fatigue ranged from 12.9 per 100,000 population in Atlanta to 34.3 per 100,000 in Wichita, with an overall rate of 18.4 per 100,000 (Table_5). As with the CFS prevalence differences among sites, the differences in prevalence of chronic fatigue remained after adjustment, using 1990 U.S. census data, for sex, race, and age. For white women, the crude prevalence rate of unexplained chronic fatigue ranged from 28.6 cases per 100,000 population in Atlanta to 60.0 per 100,000 in Wichita, with an overall prevalence of 37.3 per 100,000. The overall crude prevalence rate of chronic fatigue for white men was 7.0 cases per 100,000. The rank orders of prevalence of CFS and unexplained chronic fatigue for the four surveillance sites were the same using both crude and the adjusted rates. Incidence An incident case was defined as a case of CFS in a patient (i.e., illness in a patient assigned to Group I) who had onset of symptoms during the 4-year surveillance period. Only 19 incident cases were identified: 10 in Atlanta, four in Wichita, four in Grand Rapids, and one in Reno. The overall annual incidence rates, as well as the site-specific annual incidence rates, were less than one case per 100,000 persons. The rates of CFS for the four surveillance sites were not significantly different, and the rates remained stable during the 4-year surveillance period. DISCUSSION This surveillance system demonstrated the feasibility of conducting surveillance for an illness characterized primarily on the basis of self-reported symptoms. This system identified the existing CFS cases in those patients who were referred to the system at the four surveillance sites. The annual number of CFS incident cases did not increase during the surveillance period. The mean age of the CFS patients at the time of symptom onset, 30 years, was similar to that reported previously (9,12). The 6.7-year average duration of fatiguing illness before participation in this surveillance system was consistent with the reported long-term nature of CFS (15). Less than 8% of the CFS patients reported an eventual absence of all symptoms during the surveillance period. If recovery from CFS is reflected by the absence of symptoms, then the 4-year period prevalence estimates should provide an estimate of point prevalence for August 31, 1993 (i.e., the last day of the surveillance period). The results of several previously published studies indicated that CFS occurs primarily among white females (12,15,16), and the high percentage of CFS patients who were white women in the CDC surveillance system for CFS was consistent with these reports. Previous reports also indicated that persons who have CFS are more likely to be well-educated and are potentially high-income earners (12,15,16). Of the CFS patients identified by the surveillance system, 96% had graduated from high school, and 38% of this group had graduated from college. Although 48% of CFS patients were unemployed at the time of interview, the median annual household income of these patients was $40,000. However, the higher prevalence of CFS among some groups in this study (e.g., white women) could reflect selection biases. For example, the education and income levels of the patients participating in the surveillance system could have influenced their pattern of using the health-care system (i.e., persons with lower incomes who had a fatiguing illness might not have sought medical care for the illness and would not have been referred to the surveillance system). The number and pattern of symptoms reported by patients in Groups I, III, and IV were similar, suggesting that the criteria of the CFS case definition do not enable clinicians to reliably distinguish which patients have a history of a psychological disorder. The National Institutes of Health (17) and CDC (18) have recommended that future studies of fatiguing illness continue to include patients both with and without a history of a psychological disorder so that information regarding these groups can be analyzed separately. The physical signs listed in the CFS case definition were not useful for classifying CFS cases. Only seven (5%) of the CFS cases were classified as such based on the presence of physical signs. Furthermore, no specific symptom or group of symptoms enabled CFS to be distinguished from illness in patients assigned to the other groups. Illnesses in Group I patients might represent one end of a CFS spectrum (i.e., the most severe degree of illness), whereas illnesses in Group II patients might represent the other end (i.e., the least severe). By definition, the Group II patients reported fewer CFS symptoms, but this group also reported substantially fewer symptoms not included in the CFS case definition. The crude estimates of the 4-year period prevalence of CFS ranged from 3.8 to 9.6 cases per 100,000 population. These estimates could not be compared with the prevalence of 7.4 per 100,000 reported previously (10) because this latter estimate a) was based on an approximation to the CDC CFS case definition and b) represented a lifetime prevalence. Because of the long duration of CFS, the period prevalence estimates derived from the CDC surveillance system can be more appropriately compared with the point prevalence estimates derived from the study conducted in Australia (9). Although the overall period prevalence estimate of CFS in the four U.S. cities (i.e., 5.2 cases per 100,000 population) was lower than the point prevalence estimate reported for the study in Australia (37.1 per 100,000), the CFS case definition used in the CDC surveillance system was more restrictive. The CDC classification for unexplained chronic fatigue more closely approximated the CFS case definition used in the study conducted in Australia (19), and the site-specific period prevalence estimates of unexplained chronic fatigue in the four U.S. cities (i.e., 11.3-27.8 cases per 100,000 population) were comparable to the point prevalence estimate of CFS derived from the study conducted in Australia (9). Reno was chosen as a surveillance site because of its close proximity to Incline Village (i.e., the site of the first CDC investigation of a cluster of CFS cases) and because of concern regarding the incidence of CFS in this geographic area (4). The prevalence of CFS in Reno, however, was similar to the prevalence in the other surveillance sites, and the incidence of CFS in this area was the lowest among the sites. This CFS surveillance system demonstrated the feasibility of collecting information concerning the demographic characteristics of participants and estimating a 4-year period prevalence for both CFS and unexplained prolonged fatigue. However, the possible underascertainment of CFS cases in this study may have biased these estimates downward; all the estimated rates should, therefore, be considered minimum estimates of the true prevalence of CFS and unexplained chronic fatigue in the four U.S. cities. At least six factors could have been associated with underreporting of CFS cases. First, some physicians who treat patients who have CFS might not have been asked to participate in the surveillance system. However, current telephone and medical directories were used to identify such physicians, and all these physicians were contacted and asked to participate in the surveillance system. In addition, physicians who were identified during the surveillance period were asked to participate, and contact was maintained with participating physicians during the surveillance period to encourage continued participation. Second, approximately 50% of all physicians who were asked to participate chose not to do so; however, most of these physicians reported that they either a) did not provide service to patients who have CFS or b) did not accept CFS as an established diagnosis. Third, follow-up surveys of the 489 participating physicians indicated that, of the 241 physicians who provided service to patients who should have been referred to the surveillance system, 22 (9%) physicians did not refer such patients. Fourth, participating physicians might have referred only those patients whose illness was probably CFS, rather than all patients whose illness met the screening criteria (i.e., greater than 67% of patients reported that their illness had been diagnosed as CFS by the physician before the referral). Fifth, 13% of the patients who had been referred to the surveillance system chose not to participate. Finally, many patients who had a fatiguing illness might not have sought medical care; however, a CDC survey conducted in 1994 indicated that 82% of persons who had unexplained chronic fatigue sought medical care for the illness (CDC, unpublished data). All these factors could have contributed to an underestimation of the prevalence of CFS and unexplained chronic fatigue in the four surveillance sites. However, these prevalence estimates, even if understated, are similar to previously reported estimates (9). The sites chosen for this surveillance system were not selected randomly; therefore, the findings cannot be directly generalized to the overall U.S. population. The range of prevalence estimates for the four sites might reflect actual differences between the sites or differences in case ascertainment. An additional limitation of this surveillance system was the potential for inaccurate recall of information by patients, whose average illness duration at the time of interview was greater than 6 years. However, many patients kept extensive records of their fatiguing illness and were able to provide detailed information regarding the onset of symptoms. Future studies of CFS should include patients who have more recent onset of illness to minimize the potential for recall bias. Despite the limitations, this surveillance system will assist in investigations of CFS and its impact on patients who have the illness. In February 1997, CDC began a large-scale, cross-sectional study at one surveillance site (Wichita) to describe more completely the magnitude and epidemiology of CFS. The population-based approach will enable investigators to actively and more completely identify patients who have CFS and unexplained chronic fatigue. Information concerning these patients can then be compared with information for persons in the same population who do not have chronic fatigue. Acknowledgments The authors thank the additional members of the physician review committee: Susan Abbey, M.D., Louisa E. Chapman, M.D., Nelson M. Gantz, M.D., James F. Jones, M.D., Nancy Klimas, M.D., Anthony L. Komaroff, M.D., Susan Levine, M.D., and Sarah Minden, M.D. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}