 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
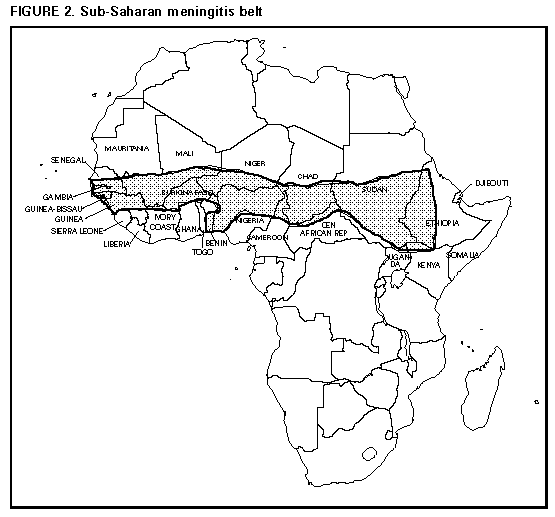
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Control and Prevention of Meningococcal Disease: Recommendations of the Advisory Committee on Immunization Practices (ACIP)Summary These recommendations update information regarding the polysaccharide vaccine licensed in the United States for use against disease caused by Neisseria meningitidis serogroups A, C, Y, and W-135, as well as antimicrobial agents for chemoprophylaxis against meningococcal disease (superseding MMWR 1985;34:255-9). This report provides additional information regarding meningococcal vaccines and the addition of ciprofloxacin and ceftriaxone as acceptable alternatives to rifampin for chemoprophylaxis in selected populations. INTRODUCTION Neisseria meningitidis causes both endemic and epidemic disease, principally meningitis and meningococcemia (1). As a result of the control of Haemophilus influenzae type b infections, N. meningitidis has become the leading cause of bacterial meningitis in children and young adults in the United States, with an estimated 2,600 cases each year (2). The case-fatality rate is 13% for meningitic disease (defined as the isolation of N. meningitidis from cerebrospinal fluid) and 11.5% for persons who have N. meningitidis isolated from blood (2), despite therapy with antimicrobial agents (e.g., penicillin) to which U.S. strains remain clinically sensitive (3). The incidence of meningococcal disease peaks in late winter to early spring. Attack rates are highest among children 3-12 months of age and then steadily decline among older age groups (Figure_1). Based on multistate surveillance conducted during 1989-1991, serogroup B organisms accounted for 46% of all cases and serogroup C for 45%; serogroups W-135 and Y and strains that could not be serotyped accounted for most of the remaining cases (2). Recent data indicate that the proportion of cases caused by serogroup Y strains is increasing (4). Serogroup A, which rarely causes disease in the United States, is the most common cause of epidemics in Africa and Asia. In the United States, localized community outbreaks of serogroup C disease and a statewide serogroup B epidemic have recently been reported (5,6). Persons who have certain medical conditions are at increased risk for developing meningococcal infection. Meningococcal disease is particularly common among persons who have component deficiencies in the terminal common complement pathway (C3, C5-C9); many of these persons experience multiple episodes of infection (6). Asplenic persons also may be at increased risk for acquiring meningococcal disease with particularly severe infections (8). Persons who have other diseases associated with immunosuppression (e.g., human immunodeficiency virus {HIV} and Streptococcus pneumoniae) may be at higher risk for acquiring meningococcal disease and for disease caused by some other encapsulated bacteria. Evidence suggests that HIV-infected persons are not at substantially increased risk for epidemic serogroup A meningococcal disease (9); however, such patients may be at increased risk for sporadic meningococcal disease or disease caused by other meningococcal serogroups (10). Previously, military recruits had high rates of meningococcal disease, particularly serogroup C disease; however, since the initiation of routine vaccination of recruits with the bivalent A/C meningococcal vaccine in 1971, the high rates of meningococcal disease caused by those serogroups have decreased substantially and cases occur infrequently (11). Military recruits now routinely receive the quadrivalent A,C,Y, W-135 meningococcal vaccine. MENINGOCOCCAL POLYSACCHARIDE VACCINE The quadrivalent A,C,Y,W-135 vaccine (Menomune -A,C,Y,W-135, manufactured by Connaught Laboratories, Inc.) is the formulation currently available in the United States. The recommended dose of vaccine is a single 0.5-mL subcutaneous injection. Each vaccine dose consists of 50 ug each of the purified bacterial capsular polysaccharides. Menomune is available in single-dose, 10-dose, and 50-dose vials. Vaccine Efficacy The immunogenicity and clinical efficacy of the serogroups A and C meningococcal vaccines have been well established. The serogroup A polysaccharide induces antibody in some children as young as 3 months of age, although a response comparable with that among adults is not achieved until 4 or 5 years of age; the serogroup C component is poorly immunogenic in recipients who are less than 18-24 months of age (12,13). The serogroups A and C vaccines have demonstrated estimated clinical efficacies of 85%-100% in older children and adults and are useful in controlling epidemics (9,14-17). Serogroups Y and W-135 polysaccharides are safe and immunogenic in adults and in children greater than 2 years of age (18-21); although clinical protection has not been documented, vaccination with these polysaccharides induces bactericidal antibody. The antibody responses to each of the four polysaccharides in the quadrivalent vaccine are serogroup-specific and independent. Duration of Efficacy Measurable levels of antibodies against the group A and C polysaccharides decrease markedly during the first 3 years following a single dose of vaccine (13,22-25). This decrease in antibody occurs more rapidly in infants and young children than in adults. Similarly, although vaccine-induced clinical protection probably persists in schoolchildren and adults for at least 3 years, the efficacy of the group A vaccine in young children may decrease markedly with the passage of time: in a 3-year study, efficacy declined from greater than 90% to less than 10% among children who were less than 4 years of age at the time of vaccination, whereas among children who were greater than or equal to 4 years of age when vaccinated, efficacy was 67% 3 years later (26). RECOMMENDATIONS FOR USE OF MENINGOCOCCAL VACCINE Routine vaccination of civilians with the quadrivalent meningococcal polysaccharide vaccine is not recommended because of its relative ineffectiveness in children less than 2 years of age (among whom risk for endemic disease is highest) and its relatively short duration of protection. However, the polysaccharide meningococcal vaccine is useful for controlling serogroup C meningococcal outbreaks (27). Indications for Use In general, use of polysaccharide meningococcal vaccine should be restricted to persons greater than or equal to 2 years of age; however, children as young as 3 months of age may be vaccinated to elicit short-term protection against serogroup A meningococcal disease (two doses administered 3 months apart should be considered for children 3-18 months of age) (28). Routine vaccination with the quadrivalent vaccine is recommended for certain high-risk groups, including persons who have terminal complement component deficiencies and those who have anatomic or functional asplenia. Persons whose spleens have been removed because of trauma or nonlymphoid tumors and persons who have inherited complement deficiencies have acceptable antibody responses to meningococcal vaccine; however, the clinical efficacy of vaccination has not been documented for these persons, and they may not be protected by vaccination (7,29). Research, industrial, and clinical laboratory personnel who routinely are exposed to N. meningitidis in solutions that may be aerosolized should be considered for vaccination. Vaccination with the quadrivalent vaccine may benefit travelers to and U.S. citizens residing in countries in which N. meningitidis is hyperendemic or epidemic, particularly if contact with the local populace will be prolonged. Single-dose vials of the quadrivalent vaccine are now available and may be more convenient than multidose vials for use in international health clinics for travelers (30). Epidemics of meningococcal disease are recurrent in that part of sub-Saharan Africa known as the "meningitis belt," which extends from Senegal in the west to Ethiopia in the east (Figure_2) (31). Epidemics in the meningitis belt usually occur during the dry season (i.e., from December to June); thus, vaccination is recommended for travelers visiting this region during that time. Epidemics occasionally are identified in other parts of the world and recently have occurred in Saudi Arabia (during a Haj pilgrimage), Kenya, Tanzania, Burundi, and Mongolia. Information concerning geographic areas for which vaccination is recommended can be obtained from international health clinics for travelers, state health departments, and CDC (telephone: {404} 332-4559). Primary Vaccination For both adults and children, vaccine is administered subcutaneously as a single 0.5-mL dose. The vaccine can be administered at the same time as other vaccines but at a different anatomic site (i.e., deltoid muscle or buttocks). Protective levels of antibody are usually achieved within 7-10 days after vaccination. Revaccination Revaccination may be indicated for persons at high risk for infection (e.g., persons remaining in areas in which disease is epidemic), particularly for children who were first vaccinated when they were less than 4 years of age; such children should be considered for revaccination after 2-3 years if they remain at high risk. Although the need for revaccination of older children and adults has not been determined, antibody levels decline rapidly over 2-3 years, and if indications still exist for immunization, revaccination may be considered within 3-5 years. PRECAUTIONS AND CONTRAINDICATIONS Reactions to Vaccination Adverse reactions to meningococcal vaccine are mild and consist principally of pain and redness at the injection site, for 1-2 days. Estimates of incidence of mild-to-moderate local reactions have varied, ranging from infrequent to greater than 40% among vaccine recipients (32,33). Pain at the site of injection is the most commonly reported adverse reaction, and a transient fever might develop in less than or equal to 2% of young children. Vaccination During Pregnancy Studies of vaccination during pregnancy have not documented adverse effects among either pregnant women or newborns (34,35). In addition, these studies have documented high antibody levels in maternal and umbilical cord blood following vaccination during pregnancy. Antibody levels in the infants decreased during the first few months after birth; subsequent response to meningococcal vaccination was not affected (35). These observations have been confirmed in more recent studies of other polysaccharide vaccines administered during pregnancy (36). Based on data from studies involving use of meningococcal vaccines and other polysaccharide vaccines administered during pregnancy, altering meningococcal vaccination recommendations during pregnancy is unnecessary. PROSPECTS FOR NEW MENINGOCOCCAL VACCINES To enhance the immunogenicity and protective efficacy of A and C polysaccharides in infants and young children, methods similar to those used for H. influenzae type b conjugate vaccines have been applied to produce conjugate serogroups A and C vaccines (37,38). Capsular polysaccharides are being covalently linked to carrier proteins to convert the T-cell-independent polysaccharide to a T-cell-dependent antigen. The efficacy of these vaccines has not been evaluated. Because the serogroup B capsular polysaccharide is poorly immunogenic in humans, vaccine development for serogroup B meningococci has focused on the outer membrane proteins as potential immunogens. The immunogenicity and protective efficacy of several outer membrane protein vaccines against several serogroup B meningococci have been evaluated recently. Evaluation of those vaccines documented estimated efficacies ranging from 57% to 83% in older children and adults (39-41). However, a subsequent study of one of these vaccines did not document efficacy in children less than 4 years of age, the group often at highest risk for disease (42). None of the currently available serogroup B meningococcal vaccines are licensed for use in the United States. ANTIMICROBIAL CHEMOPROPHYLAXIS Antimicrobial chemoprophylaxis of close contacts of sporadic cases of meningococcal disease is the primary means for prevention of meningococcal disease in the United States (Table_1). Close contacts include a) household members, b) day care center contacts, and c) anyone directly exposed to the patient's oral secretions (e.g., through kissing, mouth-to-mouth resuscitation, endotracheal intubation, or endotracheal tube management). The attack rate for household contacts exposed to patients who have sporadic meningococcal disease has been estimated to be four cases per 1,000 persons exposed, which is 500-800 times greater than for the total population (43). Because the rate of secondary disease for close contacts is highest during the first few days after onset of disease in the primary patient, antimicrobial chemoprophylaxis should be administered as soon as possible (ideally within 24 hours after the case is identified). Conversely, chemoprophylaxis administered greater than 14 days after onset of illness in the index case-patient is probably of limited or no value. Oropharyngeal or nasopharyngeal cultures are not helpful in determining the need for chemoprophylaxis and may unnecessarily delay institution of this preventive measure. Rifampin is administered twice daily for 2 days (600 mg every 12 hours for adults, 10 mg/kg of body weight every 12 hours for children greater than or equal to 1 month of age, and 5 mg/kg every 12 hours for infants less than 1 month of age). Rifampin is effective in eradicating nasopharyngeal carriage of N. meningitidis (44). Rifampin is not recommended for pregnant women, because the drug is teratogenic in laboratory animals. Rifampin changes the color of urine to reddish-orange and is excreted in tears and other body fluids; it may cause permanent discoloration of soft contact lenses. Because the reliability of oral contraceptives may be affected by rifampin therapy, consideration should be given to using alternate contraceptive measures while rifampin is being administered. In addition to rifampin, other antimicrobial agents are effective in reducing nasopharyngeal carriage of N. meningitidis. Ciprofloxacin in various dosage regimens is greater than 90% effective in eradicating nasopharyngeal carriage (45,46). A single 500-mg oral dose of ciprofloxacin is a reasonable alternative to the multidose rifampin regimen. Ciprofloxacin levels in nasal secretions far exceed the MIC90 for N. meningitidis following oral dosing (47). Ciprofloxacin is not generally recommended for persons less than 18 years of age or for pregnant and lactating women because the drug causes cartilage damage in immature laboratory animals. However, a recent international consensus report has concluded that ciprofloxacin can be used for chemoprophylaxis of children when no acceptable alternative therapy is available (48). When ceftriaxone was administered in a single parenteral dose (an intramuscular dose of 125 mg for children and 250 mg for adults), it was 97%-100% effective in eradicating pharyngeal carriage of N. meningitidis (49,50). Thus, ceftriaxone (diluted in 1% lidocaine to reduce local pain after injection) is also a reasonable alternative for chemoprophylaxis. Systemic antimicrobial therapy of meningococcal disease with agents other than ceftriaxone or other third-generation cephalosporins may not reliably eradicate nasopharyngeal carriage of N. meningitidis. If other agents have been used for treatment, the index patient should receive chemoprophylactic antibiotics for eradication of nasopharyngeal carriage before being discharged from the hospital (51). CONCLUSIONS N. meningitidis is the leading cause of bacterial meningitis in older children and young adults in the United States. The quadrivalent A, C, Y, and W-135 meningococcal vaccine available in the United States is recommended for control of serogroup C meningococcal disease outbreaks and for use among certain high-risk groups, including a) persons who have terminal complement deficiencies, b) persons who have anatomic or functional asplenia, and c) laboratory personnel who routinely are exposed to N. meningitidis in solutions that may be aerosolized. Vaccination also may benefit travelers to countries in which disease is hyperendemic or epidemic. Conjugate serogroup A and C meningococcal vaccines are being developed by using methods similar to those used for H. influenzae type b conjugate vaccines, and the efficacies of several experimental serogroup B meningococcal vaccines have been documented in older children and young adults. Antimicrobial chemoprophylaxis of close contacts of patients who have sporadic cases of meningococcal disease is the primary means for prevention of meningococcal disease in the United States. Rifampin has been the drug of choice for chemoprophylaxis; however, data from recent studies document that single doses of ciprofloxacin or ceftriaxone are reasonable alternatives to the multidose rifampin regimen for chemoprophylaxis. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}