 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hypothermia-Related Deaths -- Vermont, October 1994-February 1996Hypothermia is a lowering of the core body temperature to less than or equal to 95 F (less than or equal to 35 C) (1). From 1979 through 1992, a total of 10,550 persons in the United States died from hypothermia, an average of 754 deaths per year (range: 557-1021 deaths) (2). From October 1994 through February 1996, a total of 10 hypothermia-related deaths were reported by the chief medical examiner in Vermont. The average age of the 10 decedents was 62 years (range: 18-88 years); eight were men. Seven decedents were reported to have had histories of mental illness, and alcohol abuse was mentioned on the police or pathology report for two decedents. This report summarizes the investigation of three of these deaths and describes risk factors commonly associated with hypothermia. Case 1. In March 1995, an 18-year-old woman was found dead, lightly clothed, and covered in snow in the woods behind her house. During the preceding 24 hours, the minimum temperature had been 34 F (1 C), and 0.04 inches of precipitation had fallen. The woman had a prolonged history of drug abuse. At autopsy, a blood test revealed the presence of benzodiazepines (diazepam, nordazepam, temazepam, and oxazepam) and diphenhydramine. Drug overdose was listed as the primary cause of death with hypothermia as a contributing cause. Case 2. In November 1995, a 74-year-old man was found without a coat lying in a field 250 feet from his residence; he was unresponsive and had no palpable pulse. The outside temperature had been 11 F (-12 C) the previous night. He lived alone and, during the previous 2 weeks, had been reported to be increasingly confused with incidences of wandering and entering wrong apartments. He was last seen at 6:30 p.m. the evening before he was discovered. On admission to the hospital, his core body temperature was 68 F (20 C), and he died despite resuscitative efforts. He had a medical history of dementia, atherosclerotic cardiovascular disease, and diabetes. Cold exposure was listed as the primary cause of death, dementia as a secondary cause, and atherosclerotic cardiovascular disease and diabetes as contributory medical conditions. Case 3. In January 1996, a 46-year-old woman was found frozen in a snow bank; a bottle of liquor was nearby. She had a history of depressive disorder and alcohol abuse. Two days before she was found, she reportedly had been drinking heavily when she left one house to walk to another. At autopsy, her blood alcohol concentration (BAC) was 0.33 g/dL. Hypothermia was listed as the primary cause of death, with ethanol intoxication as a contributing factor. Reported by: L Siciliano, PL Morrow, MD, Office of the Chief Medical Examiner; J Carney, MD, Vermont Dept of Health. Div of Environmental Hazards and Health Effects, National Center for Environmental Health, CDC. Editorial NoteEditorial Note: From 1979 through 1992, approximately half of all hypothermia deaths in the United States occurred among persons aged greater than or equal to 65 years (Figure_1). The annual death rate for hypothermia in this age group was 1.3 per 100,000 persons compared with the annual, age-adjusted death rate for hypothermia of 0.3 per 100,000 (3). Elderly persons particularly are at risk for hypothermia because of medical and socioeconomic factors such as underlying diseases, social isolation, and physiologic changes (e.g., lack of appropriate vasoconstriction in response to cold environments, decreased basal metabolic rate, and impaired shivering mechanism). The risk for hypothermia-related death also was greater in men than in women (age-adjusted death rates, 2.0 versus 0.7 per 100,000 among persons aged greater than or equal to 65 years, respectively); reasons for this difference have not been defined. Ethanol abuse, which is strongly associated with hypothermia, results in vasodilation and interferes with peripheral vasoconstriction, an important physiologic mechanism of defense against the cold. Neuroleptic drugs also predispose a person to hypothermia by inducing vasodilation and suppressing the shivering response. The hypothermic effects of these types of drugs are amplified by lower ambient temperatures. Other risk factors for hypothermia include hypothyroidism, mental illness, dehydration and starvation, homelessness and poverty, immobilizing illness, and sustained contact with materials that promote conductive heat loss (e.g., water, solvents, and metals) (1). Hypothermia-related morbidity and mortality can be prevented by early recognition and prompt medical care. Early indications of hypothermia include shivering, numbness, fatigue, poor coordination, slurred speech, impaired mentation, blueness or puffiness of the skin, and irrationality. The use of insulated clothing that does not retain moisture and appropriate head gear can assist in preventing cold-related illness because 30% of heat loss comes from the head. Immersion in water and wet clothing during cold weather should be avoided. In addition, persons who are outdoors in cold conditions should increase fluid and calorie intake, abstain from consuming alcoholic beverages, and avoid overexertion and sweating. References
Figure_1 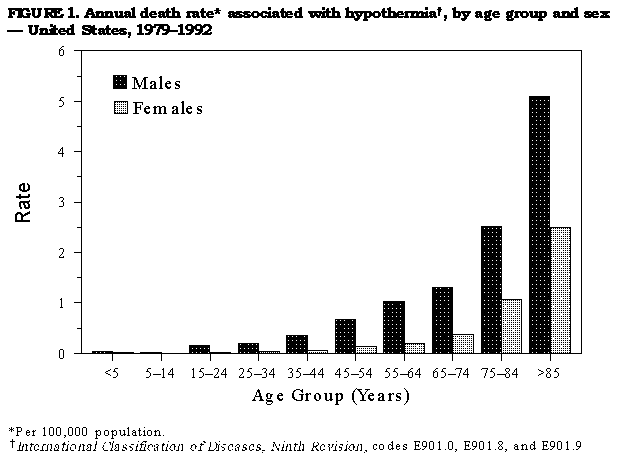 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}