 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. International Notes Emerging Polio-Free Zone -- Southern Africa, 1990-1994A key component of the global strategy to eradicate poliomyelitis by the year 2000 is surveillance for all cases of acute flaccid paralysis (AFP), ensuring the detection of cases of paralytic polio. During the 1990s, most of the countries of southern Africa Table_1 have reported high (i.e., 70%-90%) levels of vaccination coverage among children aged less than 1 year with three doses of oral poliovirus vaccine (OPV3). In addition, with the exception of Namibia, all of these countries have reported very low or zero incidence of polio (Table_1, Figure_1). To determine whether the low number of reported polio cases reflects the true incidence or underreporting, during 1992 and 1993 assessments of polio incidence and the quality of surveillance of suspected polio were conducted by teams consisting of national health officials, World Health Organization (WHO) staff and consultants, and representatives from Rotary International, using a standard protocol (1). This report summarizes the findings of assessments in Botswana, Lesotho, Malawi, South Africa, Swaziland, and Zimbabwe. Of the six countries, only Malawi maintains surveillance for AFP as recommended by WHO (2). Since 1991, all health facilities in Malawi likely to provide care for cases of AFP have reported such cases as suspected polio in the routine monthly reporting system. The local health authority immediately initiates an investigation that includes collection of stool specimens for virologic analysis. In addition, a private group specializing in rehabilitation (Malawi Against Polio) conducts approximately 700 lameness clinics serving more than 10,000 patients annually; these clinics also provide active surveillance for convalescent cases of polio. Since 1992, 13 AFP cases have been reported to the Malawi Ministry of Health; no polioviruses have been isolated from these reported cases, and no cases clinically compatible with polio (i.e., met the WHO case definition for polio) have been identified. In Botswana, Lesotho, and Zimbabwe, AFP surveillance has not yet been fully implemented, and surveillance is based on reporting of physician-diagnosed polio. Since 1990, each country has reported 0-2 cases annually. In 1992, the incidence of AFP was evaluated in Zimbabwe and included a review of hospital records for 1990-1992 of children aged less than 15 years at each of the seven provincial and three central hospitals likely to provide care to persons with cases of AFP. Of the 21 identified cases of AFP, 11 were in children aged less than 5 years. Three cases compatible with polio occurred during 1990-1991 but were not reported. The average annual AFP incidence was 0.17 per 100,000 children aged less than 15 years and 0.25 per 100,000 children aged less than 5 years. In Swaziland, polio cases had been reported every year during the 1980s; however, since 1990, no cases have been reported. The national rehabilitation center registers persons with paralytic illnesses seeking rehabilitation services; none of the 22 persons registered during 1991-1992 had cases clinically compatible with polio. In South Africa, surveillance has been based on routine reporting of physician-diagnosed polio. AFP was designated as a reportable disease in April 1994, and AFP case investigation and response in accordance with WHO guidelines is now being implemented. In September 1994, the first review of the vaccination program in South Africa conducted by national health officials and international consultants concluded that the last confirmed cases of wild virus-associated polio occurred in 1989 during an outbreak in Natal/KwaZulu (3). Reported by: Ministry of Health, Botswana. Ministry of Health, Lesotho. Ministry of Health, Malawi. Ministry of Health, Mozambique. Ministry of Health, Namibia. Dept of Health, South Africa. Ministry of Health, Swaziland. Ministry of Health and Child Welfare, Zimbabwe. Expanded Program on Immunization, World Health Organization, Regional Office for Africa, Brazzaville. Rotary International, Evanston, Illinois. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Polio Eradication Activity, National Immunization Program, CDC. Editorial NoteEditorial Note: Although polio is now a rare disease in southern Africa, surveillance is neither sufficiently sensitive nor has the quality been evaluated adequately to determine whether wild poliovirus transmission has been interrupted. Therefore, efforts are needed to strengthen both the field epidemiology and laboratory components of surveillance to enable prompt detection, investigation, and notification of all AFP cases, the collection and testing of adequate stool specimens, and the application of the standard WHO polio case definition and case classification criteria. Private practitioners and traditional healers also must be encouraged to report AFP cases. Although Namibia was considered polio-free from 1990 through May 1993, a surveillance assessment was performed in November 1993 because of the occurrence of an outbreak of 56 cases (4). The outbreak was attributed to the importation of wild poliovirus across Namibia's northern border with Angola, where polio remains endemic, and was terminated by a nationwide mass vaccination campaign with oral poliovirus vaccine (OPV). The outbreak in Namibia has emphasized the urgent need to establish AFP surveillance and the continuing risk for importations leading to polio outbreaks in the countries of southern Africa. The surveillance assessment conducted in Zimbabwe in 1992 was the first systematic attempt to determine the rate of AFP in a sub-Saharan African population. The annual AFP rate in Zimbabwe was low in comparison with the reference rate of greater than or equal to 1.0 per 100,000 children aged less than 15 years used in the Americas to define a sensitive AFP surveillance system. Explanations that may account for this finding are that 1) persons with AFP may not seek medical care or may not be referred to higher level hospitals; 2) hospital records may not be complete; 3) discharge diagnoses may be inadequately coded; or 4) the true rate of nonpolio AFP in Zimbabwe may be lower than in populations in the Americas, although during 1979-1981, the annual incidence of Guillain-Barre syndrome (the most common nonpolio cause of AFP) in the western province of South Africa ranged from 1.7 to 3.3 cases per 100,000 children aged less than 13 years (5). The apparently low incidence or virtual absence of polio in the countries of southern Africa suggests that the reduction of poliovirus transmission has precluded the need for mass vaccination campaigns with OPV at the national level. This situation parallels that in 1987 in the southern cone countries of South America (Argentina, Chile, Paraguay, and Uruguay), which were characterized by relatively high (but geographically nonuniform) levels of OPV3 coverage and few or zero reported cases of polio. In these countries, polio-free status was achieved by 1989 through strategies of subnational mass vaccination campaigns with OPV in high-risk areas identified by low coverage or recent polio cases and aggressive AFP case ascertainment. In southern Africa, the low population density, low contact rates, and sustained high levels of routine vaccination coverage also may assist in achieving adequate herd immunity. The International Certification Commission on Polio Eradication has established criteria by which countries can attain polio-free status (6). For the countries of southern Africa to achieve this objective, efforts will be necessary to strengthen polio surveillance and to implement strategies recommended by WHO for the interruption of wild poliovirus transmission (7). In November 1993, the African region of WHO initiated efforts to strengthen both disease surveillance and polio eradication activities (8). References
TABLE 1. Vaccination coverage with three does of oral poliovirus
vaccine (OPV3) among children aged <1 year, 1990-1993, and number
of reported poliomyelitis cases, 1990-1994 -- southern Africa
==================================================================
OPV3 Reported no. polio cases
---------------------- --------------------------
Country 1990 1991 1992 1993 1990 1991 1992 1993 1994 *
------------------------------------------------------------------
Botswana 82 + 50 58 57 2 0 0 0 0
Lesotho 80 75 82 78 0 0 0 1 0
Malawi 85 78 84 + -- 3 3 0 0 0
Mozambique 46 46 50 49 1 3 2 3 0
Namibia 59 + 67 70 76 0 0 0 56 0
South Africa 76 82 79 81 5 2 0 0 0
Swaziland 89 79 86 + 73 0 0 0 0 0
Zimbabwe 76 78 + 81 73 0 0 0 0 0
------------------------------------------------------------------
* Provisional data based on reports received by World Health
Organization, Geneva, as of October 3, 1994.
+ Based on survey data rather than routine coverage reporting.
==================================================================
Return to top. Figure_1 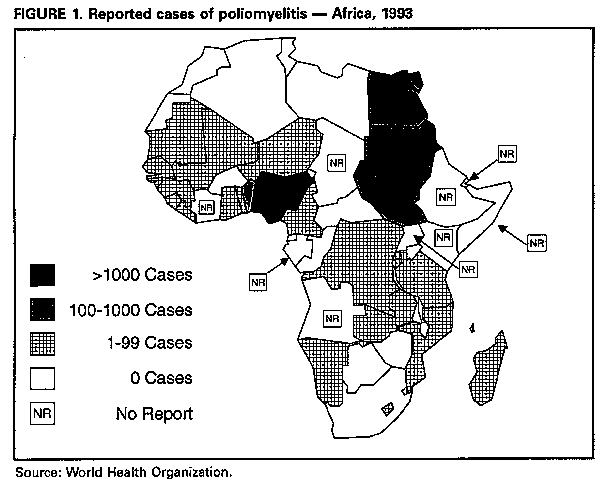 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}