 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
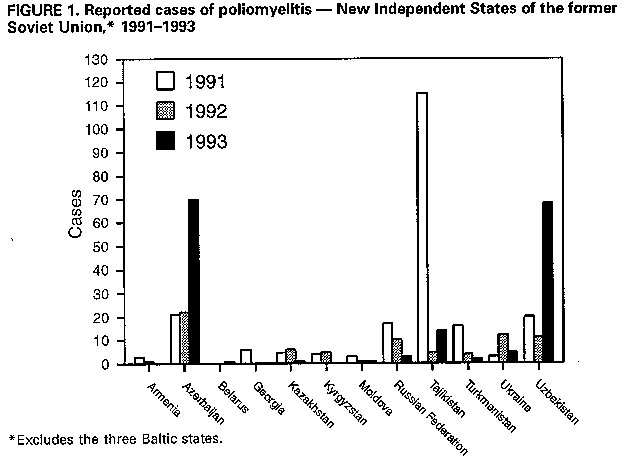
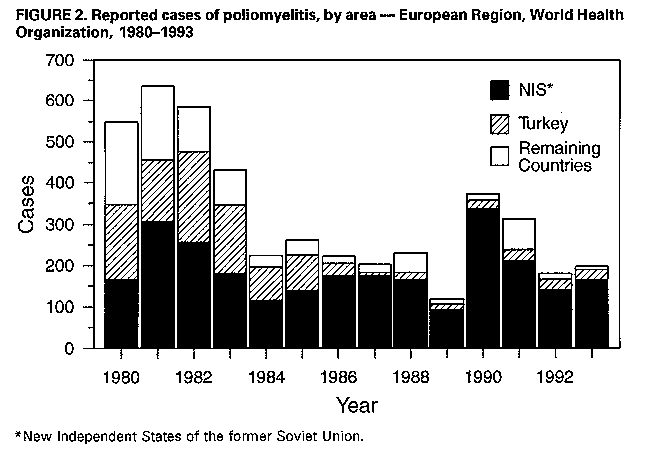
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. International Notes Status of Poliomyelitis Eradication -- Europe and the Central Asian Republics, 1993In 1989, the World Health Organization (WHO) Regional Office for Europe adopted a resolution to eradicate poliomyelitis from the European Region by the year 2000. This report summarizes progress toward that goal. In 1993, countries in the European Region of WHO (which includes the central Asian republics of the New Independent States (NIS) of the former Soviet Union) reported 198 cases of polio (presumed or known to be attributable to wild poliovirus), including one case classified as imported. In addition, 21 cases of vaccine-associated polio were reported. Each year during 1990-1992, a total of 373, 318, and 181 indigenous cases of polio, respectively, were reported in Europe. In 1993, outbreaks of polio occurred in Azerbaijan (70 cases) and Uzbekistan (68 cases). Polio was reported from 12 (24%) of the 50 countries in the European Region in 1993. Excluding the Netherlands, Romania, and Turkey, all these countries are republics of the NIS, located in Eastern Europe (Belarus, Moldova, Russian Federation, and Ukraine), the Transcaucasus Region (Azerbaijan), or in Central Asia (Kazakhstan, Tajikistan, Turkmenistan, and Uzbekistan). During 1991-1993, four countries (Azerbaijan, Tajikistan, Turkey, and Uzbekistan) consistently reported more than five cases of polio each year; each republic of the NIS reported at least one case (Figure_1). In 1980, the Soviet Union, Turkey, and the remaining European countries reported approximately one third of polio cases each. However, in 1993, the republics of the NIS reported 83% of cases (Figure_2). A recent analysis of geopolitical units (districts and oblasts) in the European Region that continue to report polio indicated a substantial decrease (50%) from 1992 to 1993 in the number of districts and oblasts in which wild poliovirus circulated (from 105 in 1992 to 52 in 1993). Individual countries in the region continue to refine and implement strategies to eradicate polio. In addition to strengthening routine vaccination-delivery systems, all polio-endemic countries (except the Federal Republic of Yugoslavia {Serbia and Montenegro} and Turkey) have adopted supplemental vaccination activities with oral poliovirus vaccine (OPV). Surveillance continues to be strengthened, with monitoring for acute flaccid paralysis (AFP) recently adopted in 11 additional countries (Bulgaria, Czech Republic, Hungary, Ireland, Poland, Romania, Russian Federation {some areas}, Slovakia, Turkey, Ukraine, and the United Kingdom). In the European Region, progress toward polio eradication was made despite civil unrest and war in some countries and the recent large-scale reemergence of diphtheria in Azerbaijan, Russian Federation, and Ukraine (1). In some areas, lack of financial resources resulted in insufficient supplies of OPV and other vaccines. In particular, the polio outbreaks in Azerbaijan and Uzbekistan can be attributed to shortages of OPV. However, countries with sufficient supplies of OPV also experienced endemic poliovirus transmission. For example, during 1989-1993, Turkey reported 14-27 cases of polio annually; the primary reason for the ongoing endemic spread of poliovirus in this country may be attributed to low OPV coverage among children aged less than 1 year (69% with three doses of OPV in 1992 versus 65% in 1993). Other countries with ongoing endemic poliovirus transmission and relatively low vaccination coverage levels during 1992 and 1993 include Azerbaijan (70% in 1992 versus 40% in 1993), Russian Federation (69% in 1992 versus 82% in 1993), Uzbekistan (85% in 1992 versus 46% in 1993), and Tajikistan (precise data are not available). Reported by: Regional Office for Europe, Copenhagen, Denmark; Expanded Program on Immunization, Global Program for Vaccines, World Health Organization, Geneva. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Polio Eradication Activity, National Immunization Program, CDC. Editorial NoteEditorial Note: Rapid progress toward global eradication of polio has been demonstrated through regional elimination of polio in the Western Hemisphere (2,3); steady movement toward elimination in countries of East Asia, including China (4), Philippines (5), and Vietnam (6); and development of polio-free zones in northern and southern Africa and on the Arabian Peninsula. However, increased efforts are needed in other areas, including the Indian subcontinent, sub-Saharan Africa, the Transcaucasus Region, and the central Asian republics (7). Many of the poliovirus genotypes responsible for recent epidemics in Europe (including the outbreak of 71 cases caused by poliovirus type 3 in the Netherlands during 1992-1993) probably originated from the Indian subcontinent (8). Countries in the European Region are categorized into three major areas with distinct epidemiologic characteristics. The western and central European countries, which have achieved high vaccination coverage and good sanitation, have eliminated polio as an indigenous disease; however, this area remains subject to importations of poliovirus, particularly among groups that routinely object to vaccination (e.g., members of religious groups in the Netherlands) or groups with suboptimal coverage (e.g., migrant or hard-to-reach populations {9}). The Balkan and Asia Minor countries (excluding Turkey) have controlled polio well, even though small outbreaks have occurred periodically -- most recently during 1990-1991 in Bulgaria (10) and Romania (CDC, unpublished data, 1993). In the NIS, two major geographic reservoirs of poliovirus have emerged -- the Transcaucasus Region and the central Asian republics. Increased efforts to eliminate polio in Europe must be aimed at the two geographic poliovirus reservoirs and the remaining polio-endemic countries. In all polio-endemic geopolitical units, routine vaccination coverage with three doses of OPV must be increased to more than 90% of children aged less than 1 year, and an additional dose of OPV should be administered at birth. In all polio-endemic countries, supplemental OPV vaccination activities (e.g., National Immunization Days *) should be implemented. Because the number of districts and oblasts in the European Region that reported cases of polio in 1993 has declined substantially, "mopping up" ** has become a feasible strategy. Nongovernmental organizations, particularly Rotary International, have been instrumental in raising funds to support the initiative to eradicate polio worldwide. Political commitment and funding by member countries of the European Region will be needed to eradicate polio from the area by the year 2000. References
* Mass campaigns over a short period (days to weeks) in which two doses of OPV are administered to all children in the target age group, regardless of prior vaccination history, with an interval of 4-6 weeks between doses. ** House-to house administration of two doses of OPV to all young children with an interval of 4-6 weeks between doses. This supplemental activity aims to reach primarily infants and children not covered by existing routine vaccination programs.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}