 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
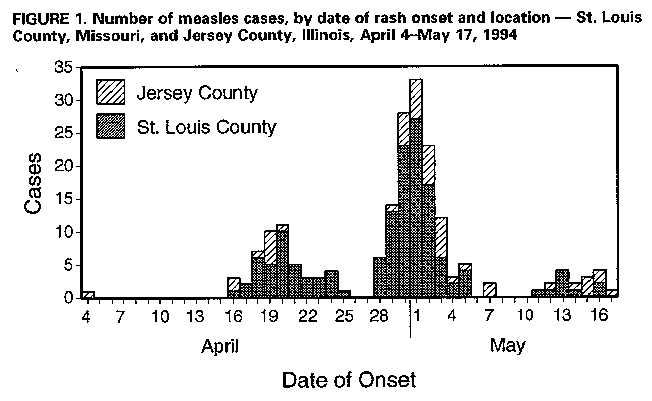
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Measles Among Christian Science Students -- Missouri and Illinois, 1994During April 4-May 17, 1994, the largest U.S. measles outbreak since 1992 occurred among students in two communities that do not routinely accept vaccination. This report summarizes the investigation of and control measures for this outbreak. The outbreak began in a 14-year-old Christian Science high school student who developed a rash on April 4, 2 weeks after skiing in Colorado where a measles outbreak was occurring. The student lived with her family in a community associated with a Christian Science college in Jersey County, Illinois, and commuted approximately 30 miles to a Christian Science boarding school (kindergarten through grade 12 {K-12}) in St. Louis County, Missouri. From April 16 through May 19, 141 persons with measles (age range: 1-24 years) were reported to the St. Louis County Health Department, and 49 persons with measles (age range: 4-25 years) were reported to the Jersey County Health Department (Figure_1). All cases met the measles clinical case definition (1) and were epidemiologically linked to the boarding school and/or college. Fourteen cases were serologically confirmed by detection of immunoglobulin M antibody. All cases occurred among persons not vaccinated before the outbreak. Eighteen prospective students from outside St. Louis County attended a carnival at the boarding school on April 16; eight developed measles after returning home (three to Maine, two to California, and one each to Missouri, New York, and Washington). Two cases of serologically confirmed measles occurred in persons outside the Christian Science communities. One case occurred in an unvaccinated 35-year-old physician who attended a tennis tournament on April 30 where students from the affected college competed. The other case occurred in a 9-month-old infant who visited a restaurant on April 30 where the college tennis team was eating. Control measures included offering measles vaccine to students in the affected communities and isolating persons with rashes and those considered susceptible to measles. On April 19, the boarding school and college began isolating persons with rashes in a separate building on each campus and placing 24-hour guards at campus entrances. Only persons with proof of immunity to measles were permitted to enter or leave the campuses. Isolation measures on both campuses remained in effect until 14 days after the appearance of rash in the last persons with measles for each school. Students who did not live on campus and had no proof of vaccination were voluntarily isolated in their homes, unless they were born before 1957 or could provide documentation of 1) previous physician-diagnosed measles, 2) laboratory evidence of measles immunity, 3) two doses of measles vaccine at least 1 month apart on or after their first birthday, or 4) one dose of measles vaccine on or after April 18, 1994. Measles vaccination was offered to Christian Science students and persons in the surrounding communities at special clinics offered by the public health departments in both Missouri and Illinois. A total of 149 Christian Science students (K-12) and their siblings were vaccinated in Missouri and 451 in Illinois. Of the 149 students at the boarding school who received measles-mumps-rubella vaccine (MMR) during outbreak control, 61 (41%) developed measles within 2 weeks after vaccination. Siblings of persons with measles who were enrolled in public schools in St. Louis County were voluntarily isolated at home. Active surveillance for persons with rashes was initiated in the county public schools on May 9 and consisted of a daily telephone call from the health department to the head nurse in each school district who monitored all student absentees for rash illness. A second dose of measles vaccine was administered to 675 students in vaccination clinics conducted in four public schools in St. Louis County and three public schools in the city of St. Louis where rash cases were detected. No outbreak-control vaccination was conducted in Illinois public schools because two doses of measles vaccine had been mandated for all K-12 schoolchildren since 1993, and compliance with this law was considered to be high. As of June 29, no additional measles cases had been reported among persons outside the Christian Science community in St. Louis County or elsewhere in Missouri or in Illinois. In response to the outbreak, St. Louis County will require two doses of measles vaccine for all schoolchildren by the start of the 1994-95 school year. Reported by: L Fisher, M Williams, L Feltmann, St. Louis County Dept of Health, Clayton; D Donnell, T Hicks, Missouri Dept of Health. T Macias, L Watson, Jersey County Health Dept, Jerseyville; C Jennings, Illinois Dept of Public Health. National Immunization Program, CDC. Editorial NoteEditorial Note: The magnitude of this outbreak illustrates the potential challenges that groups that do not routinely accept vaccination present for eliminating indigenous measles in the United States by 1996 (2,3). Communities that do not accept vaccination are at risk for recurring outbreaks and may provide foci of infection that can result in further transmission. Measles outbreaks had occurred at both the school and college in this report during 1978, 1980, 1985, and 1989; three students died from measles-related complications in the 1985 outbreak (2). From January 1 through June 10, 1994, outbreaks among persons who do not accept vaccination in Illinois, Missouri, Nevada, and Utah accounted for approximately 50% of all reported measles cases (excluding U.S. territories). Although Christian Science doctrine does not forbid medical care, many Christian Science parents claim religious exemption from childhood vaccination requirements. Vaccination is accepted by some members, particularly when the consequences of illness are considered less acceptable. During this outbreak, many Christian Science students accepted vaccination to attend school. However, individual decisions to be vaccinated may not be made until an outbreak is established and its potential impact becomes apparent. During measles outbreaks in educational institutions, revaccination with MMR is recommended (4). If measles vaccine is administered within 72 hours of exposure, it may prevent or modify illness (4). The 41% postexposure vaccine failure rate in this outbreak underscores the need for a sensitive and timely measles surveillance system to identify cases promptly and to administer vaccine as early as possible. Persons vaccinated more than 72 hours postexposure may develop infection and contribute to further spread of measles. Factors that may have contributed to limiting this outbreak include the self-imposed isolation of persons with and those susceptible to measles in the Christian Science community, high vaccination levels for one dose of measles vaccine among Missouri students and two doses among Illinois students, cooperation from private physicians in providing a second dose of measles vaccine to school-aged children both before and during the outbreak, and media coverage of the outbreak encouraging parents to obtain a second dose of measles vaccine for their children. The findings in this report illustrate that transmission of measles can be prevented or minimized by 1) maintaining high vaccination levels in the general population, 2) conducting active surveillance in populations that do not routinely accept vaccination, and 3) initiating aggressive control efforts during an outbreak. Public health officials should emphasize in communities that do not routinely accept vaccination the importance of vaccination, active surveillance, and timely reporting of contagious diseases to the public health department. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}