 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update on Adult Immunization Recommendations of the Immunization Practices Advisory Committee (ACIP)This statement on adult immunization is a supplement to the "General Recommendations on Immunization" of the Immunization Practices Advisory Committee (ACIP) (1) and updates the previous supplement published in September 1984. This statement presents an overview on immunization for adults and makes specific immunization recommendations. The statement provides information on vaccine-preventable diseases; indications for use of vaccines, toxoids, and immune globulins recommended for adults; and specific side effects, adverse reactions, precautions, and contraindi- cations associated with use of these immunobiologics. It also gives immunization recommendations for adults in specific age groups and for those who have special immunization requirements because of occupation, life-style, travel, environmental situations, and health status. This statement is a compendium of ACIP recommendations and will not be updated regularly. The ACIP periodically reviews individual immunization statements that are published in the MMWR. The reader must use the detailed, up-to-date individual statements in conjunction with this compendium to keep abreast of current information. A list of the current ACIP recommendations for specific diseases and vaccines can be found in Appendix 1. INTRODUCTION General Considerations Immunization policies have primarily been directed towards vaccinating infants, children, and adolescents. Although vaccination is routine in pediatric practice, it is not commonplace in the practice of physicians who treat adults. The widespread implementation of childhood vaccination programs has substantially reduced the occurrence of many vaccine-preventable diseases. However, successful childhood vaccination alone will not eliminate specific disease problems. A substantial proportion of the remaining morbidity and mortality from vaccine-preventable diseases presently occurs among older adolescents and adults. Persons who escaped natural infection or were not vaccinated with toxoids or vaccines against diphtheria, tetanus, measles, mumps, rubella, and poliomyelitis may be at risk of these diseases and their complications. Many factors have influenced the use of vaccines among adults, including lack of awareness of safe vaccines and vaccine- preventable health burdens, unfounded concerns about adverse reactions, and missed opportunities by health-care providers to vaccinate adults during office, clinic, or hospital visits. To improve adult immunization levels, the National Coalition for Adult Immunization (NCAI) was formed in 1988. The coalition consists of professional, private, public, and voluntary organizations with the common goal of improving vaccine use among adults by educating health-care providers and patients. A listing of member organizations is provided in Appendix 2. To reduce further the unnecessary occurrence of these vaccine- preventable diseases, health-care providers for older adolescents and adults should provide vaccinations as a routine part of their practice. In addition, the epidemiology of other vaccine-preventable diseases (e.g., hepatitis B, rabies, influenza, and pneumococcal disease) indicates that persons in certain age, occupational, environmental, and life-style groups and those with special health problems are at increased risk of these illnesses and should be vaccinated. Travelers to some countries may also be at increased risk of exposure to vaccine-preventable illnesses. Finally, foreign students, immigrants, and refugees may be susceptible to these diseases. A systematic approach to vaccination is necessary to ensure that every adult is appropriately protected against vaccine-preventable diseases. Every visit by an adult to a health-care provider should be an opportunity to provide this protection. However, several factors need to be considered before any patient is vaccinated. These include the susceptibility of the patient, the risk of exposure to the disease, the risk from the disease, and the benefits and risks of the immunizing agent. Physicians should maintain detailed records containing information about each person's previous vaccinations. The National Childhood Vaccine Injury Act of 1986 (NCVIA) requires physicians and other health-care providers who administer vaccines to maintain permanent vaccination records and to report occurrences of certain adverse events specified in the Act for all vaccines containing measles, mumps, rubella, poliomyelitis, diphtheria, tetanus, and pertussis antigens for all patients, adults as well as children (Table_1). Ideally, information for all vaccines and toxoids should be recorded. Information should also include the person's history of vaccine-preventable illnesses, occupation, and life-style. Vaccines and toxoids administered at appropriate ages and intervals should be documented in writing. Attention to factors such as military service and age may help to determine whether vaccines or toxoids are advisable for an individual. Persons who have served in the military can be considered to have been vaccinated against measles, rubella, tetanus, diphtheria, and polio. However, the practitioner should be aware that policies of the different branches of the military have varied over time and among the branches. After being administered any immunobiologic, the patient should be given written documentation of its receipt and information about which vaccines or toxoids will be needed in the future. For this purpose, a vaccination record such as the suggested form found in Appendix 3 should be used routinely. The patient or responsible person (e.g., guardian) should be given information on the risks of immunobiologics as well as their major benefits in preventing disease, both among individuals and in the community. No formal, legally acceptable statement has been universally adopted for the private medical sector. The NCVIA requires development and use of materials providing vaccine information for all covered vaccines. All physicians must give those materials, when available, to prospective vaccinees. However, CDC has developed "Important Information Statements" for use with vaccines purchased through federal contracts. (Many of these will be replaced by "Vaccine Information Pamphlets" in April 1992.) Practitioners may wish to consider these or similar materials for patients. Examples of Important Information Statements can be obtained from state and many local health departments. Forms are not available for all vaccines, however, especially those of limited use. Regardless, the ACIP recommends that health-care providers allow ample opportunity for questions before each vaccination. Modern immunobiologics are extremely safe and effective, but not completely so. Adverse events have been reported after administration of all immunobiologics. These adverse events range from frequent, minor, local reactions to extremely rare, severe systemic illness, such as paralysis associated with oral poliovirus vaccine, live, trivalent (OPV). Cause-and- effect relationships frequently cannot be established when adverse events occur after vaccination, because temporal association alone does not necessarily indicate causation. All temporally associated events severe enough to require the recipient to seek medical attention should be evaluated and reported in detail to the Vaccine Adverse Event Reporting System (VAERS) in order to improve knowledge about adverse reactions. (See "Requirements for Permanent Vaccination Records and Reporting of Adverse Events" section.) General vaccination considerations and recommendations are found in the ACIP statement "General Recommendations on Immunization" (1). The following recommendations apply to persons in the indicated groups. For more detailed information on immunobiologics -- including indications, side effects, adverse reactions, precautions, contraindications, dosages, and routes of administration -- providers should refer to the tables and appendices at the back of this supplement. Also, package inserts for the individual products should be consulted as necessary. Appendix 4 provides a list of vaccines, toxoids, and immune globulins available in the United States as of March 1, 1991. Reference can also be made to the Guide for Adult Immunization (2), published by the American College of Physicians, and to the recommendations of the U.S. Preventive Services Task Force (3). Age Groups The following text and Table_2 summarize the vaccines and toxoids recommended for most adults, by specific age groups. Table_3 summarizes the vaccines and toxoids recommended for normal infants and children. Refer to the section "Vaccine-Preventable Diseases and Their Immunobiologics" for other essential information. Adults 18-24 Years Old All young adults should complete a primary series of diphtheria and tetanus toxoids if they have not done so during childhood. A primary series for adults is three doses of preparations containing diphtheria and tetanus toxoids; the first two doses should be given at least 4 weeks apart and the third dose, 6-12 months after the second. Those who have completed a primary series should receive a booster dose every 10 years. Doses need not be repeated when the series schedule is delayed. The combined tetanus and diphtheria toxoids, adsorbed (for adult use) (Td), should be used. Persons with unknown or uncertain histories of receiving diphtheria or tetanus toxoids should be considered unvaccinated and should receive a full three- dose primary series of Td. Young adults should be immune to measles, rubella, and mumps. In 1989, as a result of outbreaks of measles in school and college settings, new recommendations were made to implement a routine two-dose schedule for measles-mumps-rubella vaccine, live (MMR). The schedule will usually be implemented gradually, one age group at a time, beginning with entry into kindergarten or first grade. Some areas of the country may implement the second dose of MMR at an older age (e.g., entry into middle school or junior high school). Young adults who are attending college (or other post- high school educational institutions) or who are newly employed in situations that place them at high risk of measles transmission (e.g., health-care facilities) should have documentation of having received two doses of live MMR on or after their first birthday or other evidence of immunity. Persons born after 1956 who are traveling to areas endemic with measles should be given two doses of live MMR. All other young adults in this age group should have documentation of a single dose of live MMR on or after their first birthday, documentation of physician-diagnosed disease, or laboratory evidence of immunity. Eventually, all persons in this age group will require two doses of measles vaccine. However, until the new recommendations are fully implemented, a single dose on or after the first birthday will be sufficient evidence of immunity for most persons. During outbreaks of measles, all persons at risk should have evidence of immunity to measles. Acceptable evidence of measles immunity consists of documentation of two doses of a live measles vaccine (preferably MMR), given at least 1 month apart after the first birthday; documentation of physician-diagnosed measles; or laboratory evidence of immunity to measles. During outbreaks of mumps and rubella, all persons at risk should have evidence of immunity to mumps and rubella. Acceptable evidence of mumps/rubella immunity consists of documentation of at least one dose of live mumps- and/or rubella-containing vaccine (preferably MMR), laboratory evidence of immunity, or physician-diagnosed mumps. Physician diagnosis is not adequate evidence of immunity against rubella. Persons vaccinated with killed-measles-virus vaccine (available in the United States from 1963 until 1967) or with a measles vaccine of unknown type should receive two doses of live-measles-virus vaccine at least 1 month apart to prevent measles disease or atypical measles syndrome -- if exposed to wild measles virus. Persons are considered immune to rubella only if they have a record of vaccination with rubella vaccine on or after their first birthday or laboratory evidence of immunity. MMR is the vaccine of choice if recipients are likely to be susceptible to more than one of the three diseases. Persons lacking adequate documentation should be vaccinated. Adults 25-64 Years Old All adults 25-64 years of age should have completed a primary series of diphtheria and tetanus toxoids. If needed, a primary series for adults is three doses of preparations containing diphtheria and tetanus toxoids -- the first two doses given at least 4 weeks apart and the third dose given 6-12 months after the second. Those who have completed a primary series should receive a booster dose every 10 years. To enhance protection against both diseases, Td should be used. Persons with unknown or uncertain histories of receiving diphtheria or tetanus toxoids should be considered unvaccinated and should receive a full three-dose primary series of Td. All adults born in 1957 or later who do not have a medical contraindi- cation should receive one dose of measles vaccine unless they have a dated record of vaccination with at least one dose of live measles vaccine on or after their first birthday, documentation of physician-diagnosed disease, or laboratory evidence of immunity. Serologic studies of hospital workers indicate that up to 9.3% of persons born before 1957 were not immune to measles (4,5). In addition, of all measles cases reported to the CDC from 1985 through 1990, 3.7% occurred among persons born before 1957. These data suggest that most persons born before 1957 can be considered immune to measles and do not need to be vaccinated. However, 97 (29%) of 341 health- care workers who had measles in the period 1985-1989 were born before 1957 (6). Therefore, because health-care workers are at particularly high risk of measles and a small proportion born before 1957 will be susceptible, vaccine should be offered to such persons if there is reason to believe that they may be susceptible. Some adults, such as college students, persons working in health-care facilities, and international travelers, are at increased risk of measles. Such persons should have evidence of two doses of live measles vaccine or other evidence of measles immunity, if born in 1957 or later. Although most adults are likely to have been infected naturally with mumps, mumps vaccine should be given to adults who are considered susceptible. Persons born in 1957 or later can be considered immune if they have evidence of one dose of live mumps vaccine or other evidence of mumps immunity. Unless proof of vaccination with rubella vaccine or laboratory evidence of immunity is available, rubella vaccine is recommended for adults, especially women of childbearing age. The vaccine of choice is MMR if recipients are likely to be susceptible to more than one of these three diseases. Adults Greater Than or Equal To 65 Years Old All older adults should have completed a primary series of diphtheria and tetanus toxoids. If needed, a primary series for adults is three doses of preparations containing diphtheria and tetanus toxoids; the first two doses should be given at least 4 weeks apart and the third dose 6-12 months after the second. Those who have completed a primary series should receive a booster dose every 10 years. Td should be used to provide protection against both diseases. Persons with unknown or uncertain histories of receiving diphtheria or tetanus toxoids should be considered unvaccinated and should receive a full three-dose primary series of Td. All older adults should receive influenza vaccine annually. They should also receive a single dose of pneumococcal polysaccharide vaccine. Revaccination should be strongly considered greater than or equal to 6 years after the first dose for those at highest risk of a) fatal pneumococcal disease (such as asplenic patients) or b) rapid decline in antibody levels (e.g., transplant recipients or those with chronic renal failure or nephrotic syndrome). Special Occupations Persons in specific occupations may be at increased risk of exposure to certain vaccine-preventable illnesses. Such persons may need selected vaccines and toxoids in addition to those routinely recommended for their age group. Table_4 provides a summary of immunobiologics recommended for various special occupational groups. The reader is referred to the section on "Vaccine-Preventable Diseases and Their Immunobiologics" for other essential information. Health- and Public-Safety-Related Occupations Because of their contact with patients or infectious material from patients, many health-care workers (e.g., physicians, nurses, dental professionals, medical and nursing students, laboratory technicians, and administrative staff) and public-safety workers (e.g., police, emergency medical personnel, firefighters) are at risk for exposure to and possible transmission of vaccine-preventable diseases. Optimal use of immunizing agents will not only safeguard the health of workers but also will protect patients from becoming infected. A consistent program of vaccinations could eliminate the problem of having susceptible health-care workers in hospitals and health departments (with the attendant risks to other workers and patients). The CDC publication "Immunization Recommendations for Health-Care Workers" (7) and the section below discuss this subject in detail. Hepatitis B virus (HBV) infection is a major occupational hazard for health-care and public-safety workers. The risk of acquiring HBV infection from occupational exposures depends on the frequency of percutaneous and permucosal exposures to blood or blood products. Any health-care or public- safety worker may be at risk for HBV exposure, depending on the tasks that he or she performs. If those tasks involve contact with blood or blood- contaminated body fluids, workers should be vaccinated. Vaccination should be considered for other workers, depending on their exposure to blood and/or bodily fluids. Selected staff of institutions for the develop- mentally disabled may be at increased risk of HBV infection because of exposure to human bites and contact with skin lesions, saliva, and other potentially infected secretions in addition to blood. The Occupational Safety and Health Administration, Department of Labor, is developing regulations that will require employers who have employees at risk of occupational exposure to hepatitis B to offer these employees hepatitis B (HB) vaccine at the employer's expense. These regulations are expected to accelerate and broaden the use of HB vaccine among health-care workers and to assure efforts to prevent this occupational disease. Among health-care personnel with frequent exposure to blood, the prevalence of serologic evidence of HBV infection ranges between approximately 15% and 30%. In contrast, the prevalence in the general population averages 5%. The cost-effectiveness of serologic screening to detect susceptible individuals among health-care personnel depends on the prevalence of infection and the costs of testing and of the HB vaccine. Each institution must decide whether serologic screening is cost effective. Vaccination of persons who already have antibodies to HBV has not been shown to cause adverse effects. HB vaccine provides protection against HBV for greater than or equal to 7 years after vaccination; booster doses are not recommended during this interval. The need for later booster doses will be assessed as additional information becomes available. Influenza vaccination is recommended yearly for physicians, nurses, and other personnel in hospital, chronic-care, and outpatient-care settings who have contact with high-risk patients in all age groups. Those who provide essential community services (e.g., public-safety workers) may consider receiving the vaccine also. Vaccination should reduce the possibility of transmitting influenza from health-care workers to patients and reduce health-care workers' risk of illness and absenteeism due to influenza. Transmission of rubella in health facilities (e.g., hospitals, physicians' or dentists' offices, and clinics) can disrupt hospital or office routines and cause considerable expense. Although no cases of congenital rubella syndrome (CRS) have been reported in association with rubella transmission in health facilities, therapeutic abortions have been sought by pregnant staff members after rubella infection (8). To prevent such situations, all medical, dental, laboratory, and other support health personnel, both male and female, who might be at risk of exposure to patients infected with rubella or who might have contact with pregnant patients should be vaccinated. Rubella vaccine is recommended for all such personnel unless they have either proof of vaccination with rubella vaccine on or after their first birthday or laboratory evidence of immunity. The vaccine of choice is MMR if recipients are likely to be susceptible to measles and/or mumps as well as to rubella. Measles and mumps transmission in health facilities can also be disruptive and costly. To prevent such situations, all new employees in health-care facilities who were born in 1957 or later who may have direct patient contact should be vaccinated. Such persons can be considered immune only if they have documentation of having received two doses of live measles vaccine and at least one dose of live mumps vaccine on or after their first birthday, a record of physician-diagnosed measles or mumps, or laboratory evidence of immunity. Institutions may wish to extend this requirement to all employees, not only beginning ones. If recipients are likely to be susceptible to rubella as well as to measles and mumps, MMR is the vaccine of choice. Adults born before 1957 can be considered immune to both measles and mumps because these infections were virtually universal before the availability of measles and mumps vaccines. However, because serologic studies of hospital workers indicate that up to 9.3% of those born before 1957 were not immune to measles (4,5) and because 97 (29%) of 341 health-care workers who had measles in the period 1985-1989 in medical facilities were born before 1957 (6), health facilities should consider requiring at least one dose of measles vaccine for older employees who are at risk of occupational exposure to measles and do not have proof of immunity to this disease. Poliovirus vaccine is not routinely recommended for persons older than high-school age (greater than or equal to 18 years old). However, hospital personnel who have close contact with patients who may be excreting wild polioviruses and laboratory personnel who handle specimens that may contain wild polioviruses should have completed a primary series of poliovirus vaccine. For personnel who do not have proof of having completed a primary series, completion with enhanced potency inactivated poliovirus vaccine (eIPV)is recommended. This vaccine is preferred because adults have a slightly increased risk of vaccine-associated paralysis after receiving OPV. In addition, because vaccine polioviruses may be excreted by OPV recipients for greater than or equal to 30 days, the use of OPV increases the risk of acquiring vaccine-associated paralytic poliomyelitis among susceptible immunocompromised OPV recipients and/or their close contacts. Smallpox (vaccinia) vaccination is indicated only for laboratory workers involved with orthopox viruses and certain health-care workers involved in clinical trials of vaccinia recombinant vaccines. When indicated, smallpox (vaccinia) vaccination should be given at least every 10 years. Plague vaccine is indicated for laboratory personnel working with Yersinia pestis possibly resistant to antimicrobial agents and for persons performing aerosol experiments with Y. pestis. Anthrax vaccine is indicated for laboratory personnel working with Bacillus anthracis. Preexposure rabies vaccination is indicated for laboratory workers directly involved with testing or isolating rabies virus. Veterinarians and Animal Handlers Veterinarians and animal handlers are at risk of rabies exposure because of occupational contact with domestic and wild animals. They should receive preexposure prophylaxis with human diploid cell rabies vaccine (HDCV). Preexposure vaccination against rabies does NOT eliminate the need for additional therapy after exposure to rabies. Preexposure vaccination does, however, simplify postexposure therapy by eliminating the need for human rabies immune globulin (HRIG) and by decreasing the number of postexposure doses of vaccine needed. Persons at continued risk of frequent exposure should receive a booster dose of HDCV every 2 years or have their serum tested for rabies antibody every 2 years; if the titer is inadequate (<5 by the rapid fluorescent-focus inhibition test), they should receive a booster dose. Plague vaccine should be considered in the western United States for veterinarians and their assistants who may be exposed to bubonic or pneumonic infection in animals, particularly domestic cats. Selected Field Personnel Plague vaccine is indicated for field personnel who cannot avoid regular exposure to potentially plague-infected wild rodents and rabbits and their fleas. Preexposure rabies vaccine prophylaxis should be considered for field personnel who are likely to have contact with potentially rabid dogs, cats, skunks, raccoons, bats, or other wildlife species. Selected Occupations Anthrax vaccine is indicated for individuals who come in contact in the workplace with imported animal hides, furs, bonemeal, wool, animal hair (especially goat hair), and bristles. Sewage workers, as all other adults, should be adequately vaccinated against diphtheria and tetanus. Sewage workers are not at increased risk of polio, typhoid fever, or hepatitis A; poliovirus and typhoid vaccines and immune globulin (IG) are not routinely recommended for them. Life-Styles Various life-styles may increase the risk of exposure to certain vaccine-preventable illnesses. Persons with these life-styles may require vaccines in addition to those routinely recommended for their age group. Table_4 provides a summary of the vaccines recommended. Homosexually Active Males Homosexually active males are at high risk of HBV as well as human immunodeficiency virus (HIV) infection. Between 35% and 80% have serologic evidence of HBV infection. Susceptible homosexual males should be vaccinated with HB vaccine as early as possible after they begin homosexual activity because 10%-20% can be expected to acquire HBV infection each year. Because of the high prevalence of infection, serologic screening of homosexual males before vaccination may be cost effective regardless of age or length of homosexual activity. Homosexual men known to have HIV infection should be tested for antibody to hepatitis B surface antigen (HBsAg) 1-6 months after completing the vaccine series (HB vaccine is less effective among HIV-infected persons than among similar persons without HIV infection). Revaccination with one or more doses should be considered if the level of antibody to HBsAg (anti-HBs) is <10 milli-international units {mIU}/milliliter (mL). Injecting Drug Users Injecting drug users are at high risk of HBV as well as HIV infection. Serologic evidence of HBV infection has been found in 60%-80% of these individuals. Efforts should be made to vaccinate susceptible users with HB vaccine as early as possible after their drug use begins, because 10%-20% can be expected to acquire HBV infection each year. Because of the high prevalence of infection, serologic screening of injecting drug users before vaccination to avoid unnecessary vaccination is cost effective. Injecting drug users with known HIV infection should be tested for antibody to HBsAg 1-6 months after completion of the vaccine series; revaccination with one or more doses should be considered if their anti-HBs level is <10 mIU/mL. Drug users are also at increased risk of tetanus; their tetanus vaccination status should therefore be kept up to date with Td. Heterosexually Active Persons Heterosexually active persons with multiple sex partners are at increased risk of HBV infection. Vaccination is recommended for persons who are diagnosed to have other sexually transmitted diseases, for male or female prostitutes, and for persons who have had sexual activity with multiple partners during the previous 6 months. Environmental Situations Certain environments may place an individual at increased risk of vaccine-preventable diseases. Table_4 summarizes additional vaccines recommended for persons in selected environments. The section on "Vaccine- Preventable Diseases and Their Immunobiologics" contains other essential information. Inmates of Long-Term Correctional Facilities Serologic evidence of HBV infection has been found among 10%-80% of male prisoners. Although the frequency of transmission during imprisonment has not been clearly documented, the environment of long-term correctional facilities may be associated with a high risk of transmission of HBV infection because of the likelihood of homosexual behavior and of injecting drug use. In selected long-term institutional settings, prison officials may elect to undertake serologic HBV screening and vaccination programs. Measles and rubella outbreaks have been documented in long-term correctional facilities. All inmates of such facilities should be vaccinated against measles and rubella. If recipients are likely to be susceptible to mumps as well as to measles and rubella, MMR is the vaccine of choice. All inmates of such facilities greater than or equal to 65 years of age and those with high-risk conditions, including HIV infection, should receive yearly influenza vaccination. Pneumococcal vaccination within the past 6 years should also be documented. Residents of Institutions for the Developmentally Disabled Institutions for the developmentally disabled provide a setting conducive to the transmission of HBV infection through human bites and contact with residents' blood, skin lesions, saliva, and other potentially infectious secretions. Serologic evidence of HBV infection has been found among 35%-80% of residents of such institutions. Persons newly admitted to these institutions should be vaccinated as soon as possible. For current residents, screening and vaccination of susceptible residents is recommended. Because of the high prevalence of infection, serologic screening before vaccination of those already institutionalized may be cost effective; however, screening of new admissions very likely will not be. Residents of group homes, foster homes, and similar settings who have household contact with an HBV carrier should also be vaccinated. Many of the residents of these institutions have chronic medical conditions that put them at risk for complications from influenza illness; therefore, all residents should receive influenza vaccine yearly. Household Contacts of HBV Carriers Household contacts of HBV carriers are at high risk of infection. When HBV carriers are identified through routine screening of donated blood, prenatal screening, or other screening programs, the carriers should be notified of their status. All household contacts should be tested and susceptible contacts vaccinated. Homeless Persons There are limited data on vaccine-preventable diseases among the homeless. However, such persons will need completed vaccinations for tetanus, diphtheria, measles, mumps, rubella, influenza, and pneumococcal disease. Also, some will be at risk for HBV infection and some will require tuberculin skin testing. The vaccination status of homeless persons should be assessed whenever they are seen in any medical setting. Travel The risk of acquiring illness during international travel depends on the areas to be visited and the extent to which the traveler is likely to be exposed to diseases. When considering travel, people often seek advice regarding vaccination from health-care personnel. This provides a good opportunity to review the person's vaccination status and to administer primary series or booster doses, if needed. In most countries, measles, mumps, and rubella remain uncontrolled. Therefore, the risk of acquiring these diseases while traveling outside the United States is greater than the risk incurred within the United States. Approximately 61% of imported measles cases reported for 1985-1989 occurred among citizens returning to the United States (CDC, unpublished data). To minimize diseases imported by U.S. citizens, all persons traveling abroad should be immune to measles. Consideration should be given to providing a dose of measles vaccine to persons born in or after 1957 who travel abroad, who have not previously received two doses of measles vaccine, and who do not have other evidence of measles immunity (e.g., physician-diagnosed measles or laboratory evidence of measles immunity). If recipients are likely to be susceptible to mumps or rubella in addition to measles, MMR is the vaccine of choice. Travelers, particularly women of childbearing ages, should be immune to rubella before leaving the United States. In developed countries such as Japan, Canada, Australia, New Zealand, and European countries, the risk of acquiring other vaccine-preventable diseases such as poliomyelitis, diphtheria, and tetanus is usually no greater than the risk incurred while traveling in the United States. In contrast, travelers to developing countries are at increased risk of exposure to many infections, including wild polioviruses and diphtheria. Accordingly, such travelers should be immune to poliomyelitis and diphtheria in particular. For protection against poliomyelitis, unvaccinated adults should receive at least two doses of eIPV 1 month apart, preferably a complete primary series, before traveling to a developing country or any country with endemic polio; eIPV is preferred because the risk of vaccine- associated paralysis is slightly higher for adults than for children. If travel plans do not permit this interval, a single dose of either OPV or eIPV is recommended. For adults previously incompletely vaccinated with OPV or inactivated poliovirus vaccine (IPV), the remaining doses of either vaccine required for completion of the primary series should be given, regardless of the interval since the last dose or the type of vaccine previously received. Travelers to developing countries who have previously completed a primary series of OPV should receive a single supplementary dose of OPV. Those who have previously received a primary series of IPV should receive a single supplementary dose of either OPV or eIPV. The need for further doses of either vaccine has not been established. Persons whose age or health status places them at increased risk of complications from influenza illness and who are planning travel to the tropics at any time of year or the southern hemisphere during April through September should review their influenza vaccination history. If not vaccinated during the previous fall or winter, such persons should consider influenza vaccination before travel. Persons in the high-risk categories should be especially encouraged to receive the most currently available vaccine. Persons at high risk given the previous season's vaccine in preparation for travel should be revaccinated in the fall or winter with the current vaccine and therefore may receive two doses of influenza vaccine within 1 year. Selective vaccination of travelers with vaccines against yellow fever, cholera, typhoid, plague, meningococcal disease, rabies, or HBV infection, or administration of IG to prevent hepatitis A, is recommended on the basis of known or perceived disease-specific risks in the country or countries to be visited and the type and duration of travel within a country. For cholera and yellow fever, vaccination requirements may have been established by the country to be visited. Countries currently reporting yellow fever, cholera, and plague are identified biweekly in the "Summary of Health Information for International Travel." * Information on known or possibly infected areas is published annually in "Health Information for International Travel," * which also lists specific requirements for cholera and yellow fever vaccinations for each country. All state health departments and many county and city health departments receive both publications. They may also be obtained by calling CDC Information Services at 404-639-1819. For entry into countries requiring yellow fever or cholera vaccination, travelers must have an International Certificate of Vaccination validated by an appropriate authority. State or local health departments can provide the addresses of persons or centers able to validate certificates. Additional information on specific vaccine-preventable illnesses that a traveler might encounter is provided in the sections describing specific vaccines. Foreign Students, Immigrants, and Refugees In many countries, children and adolescents are not routinely vaccinated against diphtheria, tetanus, measles, mumps, rubella, and poliomyelitis. As a result, persons entering the United States as college or postgraduate students, immigrants, or refugees may be susceptible to one or more of these diseases. Refugees from areas of high HBV endemicity (e.g., Southeast Asia) should be screened for HBsAg and anti-HBs. Susceptible household and sexual contacts of HBsAg carriers should receive HB vaccine. Unless foreign students, immigrants, and refugees can provide a vaccination record documenting the receipt of recommended vaccines or toxoids at appropriate ages and intervals or laboratory evidence of immunity, they should receive the appropriate vaccines for their age, as noted in the "Age Groups" section and in Table_2. Special Health Status Some vaccines may be contraindicated for persons with certain health problems; other vaccines may be indicated because of an underlying health condition. Table_5 provides a summary of immunobiologics indicated or contraindicated for persons with selected health problems. Pregnancy When any vaccine or toxoid is to be given during pregnancy, delaying until the second or third trimester, when possible, is a reasonable precaution to minimize concern about possible teratogenicity. Pregnant women not vaccinated previously against tetanus and diphtheria should receive two doses of Td, properly spaced. Those who have previously received one or two doses of tetanus or diphtheria toxoid should complete their primary series during pregnancy. A primary series is three doses of preparations containing diphtheria and tetanus toxoids, with the first two doses given at least 4 weeks apart and the third dose given 6-12 months after the second. Pregnant women who have completed a primary series should receive a booster dose of Td if greater than or equal to 10 years have elapsed since their last dose. Because of a theoretical risk to the developing fetus, live-virus vaccines usually should not be given to pregnant women or to those likely to become pregnant within 3 months. If, however, immediate protection against poliomyelitis or yellow fever is needed because of imminent exposure, OPV or yellow fever vaccine may be given. If the only reason to vaccinate a pregnant woman with yellow fever vaccine is an international travel requirement, efforts should be made to obtain a waiver letter. The ACIP strongly recommends that rubella vaccine be administered in the postpartum period to women not known to be immune, preferably before discharge from the hospital. Data are not available on the safety of HB vaccines for the developing fetus. Because the vaccines contain only noninfectious HBsAg particles, the fetus should not be at risk. In contrast, HBV infection in a pregnant woman may result in severe disease for the mother and chronic infection of the newborn. Therefore, pregnancy or lactation should not be considered a contraindication to the use of this vaccine for persons who are otherwise eligible. Prenatal screening of all pregnant women for HBsAg is recommended. Such screening identifies those who are HBsAg positive and allows treatment of their newborns with hepatitis B immune globulin (HBIG) and HB vaccine, a regimen that is 85%-95% effective in preventing the development of chronic carriage of the HBV. Pregnant women who have other medical conditions that increase their risks for complications from influenza should be vaccinated; the vaccine is considered safe for pregnant women. Administering the vaccine after the first trimester is a reasonable precaution to minimize any concern over the theoretical risk of teratogenicity. However, it is undesirable to delay vaccinating pregnant women who have high-risk conditions and who will still be in the first trimester of pregnancy when the influenza season begins. The safety of pneumococcal vaccine for pregnant women has not been evaluated. Ideally, women at high risk of pneumococcal disease should be vaccinated before pregnancy. Information about immunobiologics and vaccine-preventable diseases during pregnancy is summarized in Appendix 5. Conditions that Compromise the Immune System Persons receiving immunosuppressive therapies or with conditions that compromise their immune responses (e.g., leukemia, lymphoma, generalized malignancy, and HIV infection) should receive annual influenza vaccinations with the currently formulated vaccine. Persons with these conditions have been associated with increased risk of pneumococcal disease or its complications and should receive a single dose of pneumococcal polysaccharide vaccine; revaccination should be considered 6 years after the first dose. Haemophilus influenzae type b (Hib) conjugate vaccine (HbCV) is of unproven benefit in immunocompromised persons but may be considered for those with anatomic or functional asplenia or HIV infection. The effectiveness of these vaccines among such persons may be limited, but the risk of disease is substantial and adverse reactions are minimal. Bacille Calmette-Guerin (BCG), oral typhoid vaccine, or live-virus vaccines should not be given to persons who are immunocompromised as a result of immune deficiency diseases, leukemia, lymphoma, or generalized malignancy or who are immunosuppressed as a result of therapy with cortico- steroids, alkylating drugs, antimetabolites, or radiation. However, susceptible patients with leukemia in remission who have not had chemotherapy for at least 3 months may receive live-virus vaccines. The exact interval between discontinuing immunosuppressives and regaining the ability to respond to individual vaccines is not known. Estimates of experts vary from 3 months to 1 year (9). In addition, persons with asymptomatic HIV infection should be vaccinated against measles, mumps, and rubella. Such vaccination should be considered for persons with symptomatic HIV infection because of the danger of serious or fatal measles and the accumulating evidence of the safety of administering MMR to these patients (Table_6). Short-term (<2-week) corticosteroid therapy, topical steroid therapy (e.g., nasal or skin), and intra-articular, bursal, or tendon injections with corticosteroids should not be immunosuppressive and do not contra- indicate vaccination with live-virus vaccines. Vaccination should be avoided if systemic immunosuppressive levels are achieved by topical application. Vaccines given to immunocompromised patients cannot be assumed to be as effective as when given to normal individuals. When available, postvaccin- ation antibody titrations can be done, but, in the absence of specific antibody information, appropriate immune globulins should be considered for exposures to vaccine-preventable diseases, as discussed in the "Immune Globulins" section. Hemodialysis and Transplantation Persons receiving hemodialysis have been at high risk of infection with HBV, although environmental control measures have reduced this risk during the past decade. Nationwide, an estimated 15% of hemodialysis patients have serologic evidence of HBV infection, and routine serologic screening of hemodialysis patients is currently recommended. Susceptible patients who will soon require or are currently receiving long-term hemodialysis should receive three doses of HB vaccine as soon as possible. Larger doses (two to four times those for healthy adults) and/or increased numbers of doses are recommended for these patients because of lower vaccine immunogenicity. The individual manufacturer's vaccine package inserts should be inspected to learn the proper dosages of each vaccine. Postvaccination screening to demonstrate antibody to HBsAg is recommended in this group. Approximately 60% of hemodialysis patients who receive recommended doses of HB vaccine develop protective antibodies against HBV. Revaccination with one or more additional doses should be considered for persons who do not respond to vaccination. In hemodialysis patients, protection lasts only as long as anti-HBs levels remain >10 mIU/mL. Such patients should be tested for anti- HBs annually and revaccinated when anti-HBs declines below this level. Because renal transplant recipients and persons with chronic renal disease are at increased risk of adverse consequences (including transplant rejection) from infections of the lower respiratory tract, these persons should receive annual influenza vaccination with the current formulated vaccine. Because these patients are also at increased risk of developing pneumococcal infection and experiencing more severe pneumococcal disease, they should receive pneumococcal polysaccharide vaccine. Splenic Dysfunction or Anatomic Asplenia Persons with splenic dysfunction or anatomic asplenia are at increased risk of contracting fatal pneumococcal bacteremia and should receive pneumococcal polysaccharide vaccine. They are also at risk for meningococcal bacteremia and should receive meningococcal polysaccharide vaccine. The theoretical increased risk for invasive Hib disease suggests that such persons may be considered for HbCV. Persons scheduled for elective splenectomy should receive both pneumococcal and meningococcal polysaccharide vaccines at least 2 weeks before the operation. Factor VIII and IX Deficiencies Patients with clotting disorders who receive factor VIII or IX concentrates have an increased risk of HBV infection. Such patients without serologic markers for hepatitis B should be vaccinated against hepatitis B before receiving any blood products. To avoid hemorrhagic complications, vaccination should be given subcutaneously (SC), rather than intramus- cularly (IM) as in the nonhemophilic patient. Prevaccination serologic screening for HBV markers is recommended for patients who have already received multiple infusions of these products. Chronic Alcoholism Persons with chronic alcoholism may be at increased risk of contracting a pneumococcal infection or having a more severe pneumococcal illness. Such persons, especially those with cirrhosis, should receive pneumococcal polysaccharide vaccine. High-Risk Diseases Persons with disease conditions that increase the risk of adverse consequences from lower-respiratory-tract infections should receive annual influenza vaccination with the current formulated vaccine. These conditions include the following: acquired or congenital heart disease with actual or potentially altered circulatory dynamics; any chronic disorder or condition that compromises pulmonary function; diabetes mellitus or other metabolic diseases that increase the likelihood that infections will be more severe; chronic renal disease with azotemia or nephrotic syndrome; and chronic hemoglobinopathies, such as sickle cell disease. Some chronic illnesses (e.g., chronic pulmonary disease, congestive heart failure, diabetes mellitus) predispose individuals to an increased risk of pneumococcal illness or its complications. Such persons should receive pneumococcal polysaccharide vaccine. REQUIREMENTS FOR PERMANENT VACCINATION RECORDS AND REPORTING ADVERSE EVENTS NCVIA requires physicians and other health-care providers who administer vaccines to maintain permanent vaccination records and to report occurrences of certain adverse events specified in the Act (Table_1). The vaccines and toxoids to which these requirements apply are measles, mumps, and rubella single-antigen vaccines and combination vaccines (MMR, measles, rubella vaccine, live {MR}); diphtheria and tetanus toxoids, adsorbed (pediatric) (DT); Td; tetanus toxoid, adsorbed (T); OPV; IPV; diphtheria and tetanus toxoids and pertussis vaccine, adsorbed (pediatric) (DTP); and pertussis vaccine (P). Requirements for Recording All health-care providers who administer one or more of these vaccines or toxoids are required to ensure that the recipient's permanent medical record (or a permanent office log or file) states the date the vaccine was administered, the vaccine manufacturer, the vaccine lot number, the name, the address, and the title of the person administering the vaccine. The term health-care provider is defined as any licensed health-care professional, organization, or institution, whether private or public (including federal, state, and local departments and agencies), under whose authority a specified vaccine is administered. Requirements for Reporting Adverse Events Health-care providers are required to report selected events occurring after vaccination to the Vaccine Adverse Events Reporting System (VAERS). Reportable adverse events are shown in Table_1 and include events described in the vaccine manufacturer's package insert as contraindications to receiving additional doses of vaccine. Adverse events other than those listed on Table_1 or occurring after administration of other vaccines, especially events that are serious or unusual, can also be reported to VAERS. VAERS forms and instructions are available in the "FDA Drug Bulletin" (Food and Drug Administration) and the "Physicians' Desk Reference" or by calling VAERS at 1-800-822-7967. Vaccine Injury Compensation The National Vaccine Injury Compensation Program is a system under which compensation can be paid on behalf of an individual who died or was injured as a result of being given a vaccine. The program is intended as an alternative to civil litigation under the traditional torts system in that negligence need not be proven. The program was created by NCVIA and became effective on October 1, 1988. The law established a vaccine injury table (Table_1), which lists the vaccines covered by the program as well as the injuries, disabilities, illnesses, and conditions (including death) for which compensation may be paid. The program also sets out the period of time during which the first symptom or significant aggravation of the injury must appear. This period often differs from that required for reporting. Persons may be compensated for an injury listed in Table_1 or one that can be demonstrated to result from administration of a listed vaccine. Additional information about the program is available from: Administrator National Vaccine Injury Compensation Program Health Resources and Services Administration 6001 Montrose Road, Room 702 Rockville, MD 20852 Telephone: (301) 443-6593 Persons wishing to file a claim for a vaccine injury should call or write to: U.S. Claims Court 717 Madison Place, N.W. Washington, D.C. 20005 Telephone: (202) 633-7257 VACCINE-PREVENTABLE DISEASES AND THEIR IMMUNOBIOLOGICS Vaccines, toxoids, and immune globulins are available for use in preventing many diseases. These diseases and their specific immunobiologics are presented in this section. For each immunobiologic, the dosage, route of delivery, indications for use, side effects, adverse reactions, precautions, and contraindications are described here. These are also summarized in Table_7. Toxoids Diphtheria The occurrence of diphtheria has decreased dramatically in the United States, largely because of the widespread use of diphtheria toxoid. Only 11 cases of respiratory diphtheria were reported in the period 1985-1989. Seven of these 11 cases occurred among adults greater than or equal to 20 years of age, and three among adults greater than or equal to 60 years of age. Diphtheria occurs primarily among unvaccinated or inadequately vaccinated individuals. Limited serosurveys done since 1977 indicate that 22%-62% of adults 18-39 years of age and 41%-84% of those greater than or equal to 60 years of age lack protective levels of circulating antitoxin against diphtheria (10-13). Diphtheria toxoid. Complete and appropriately timed vaccination is at least 85% effective in preventing diphtheria. The combined preparation Td is recommended for use among adults because a large proportion of them lack protective levels of circulating antibody against tetanus (10-13). Further- more, Td contains much less diphtheria toxoid than other diphtheria toxoid- containing products, and, as a result, reactions to the diphtheria component are less likely. Vaccination with any diphtheria toxoid does not, however, prevent or eliminate carriage of Corynebacterium diphtheriae. Toxoid indications. All adults lacking a completed primary series of diphtheria and tetanus toxoids should complete the series with Td. A primary series for adults is three doses of preparations containing diphtheria and tetanus toxoids, with the first two doses given at least 4 weeks apart and the third dose given 6-12 months after the second. All adults for whom greater than or equal to 10 years have elapsed since completion of their primary series or since their last booster dose should receive a dose of Td. Thereafter, a booster dose of Td should be administered every 10 years. There is no need to repeat doses if the schedule for the primary series or booster doses is delayed. Tetanus The occurrence of tetanus has decreased dramatically, largely because of the widespread use of tetanus toxoid. Nevertheless, the number of cases remained relatively constant from 1986 through 1989, during which 48-64 cases were reported annually. Tetanus occurs almost exclusively among unvaccinated or inadequately vaccinated persons. Immune pregnant women transfer temporary protection against tetanus to their infants through transplacental maternal antibody. In the period 1982-1989, persons greater than or equal to 20 years of age accounted for 95% of the 513 reported tetanus cases for which patient ages were known; persons greater than or equal to 60 years of age accounted for 59%. The age distribution of persons who died from tetanus was similar. Serosurveys done since 1977 indicate that 6%-11% of adults 18-39 years of age and 49%-66% of those greater than or equal to 60 years of age lack protective levels of circulating antitoxin against tetanus (10-13). Although surveys of emergency rooms suggest that only 1%-6% of all persons who receive medical care for injuries that can lead to tetanus receive inadequate prophylaxis (14), in 1987-1988, 81% of the people who developed tetanus after an acute injury and sought medical care did not receive adequate prophylaxis as recommended by the ACIP (14). Tetanus toxoid. Complete and appropriately timed vaccination is nearly 100% effective in preventing tetanus. Td is the preferred preparation for active tetanus immunization of adults because a large proportion of them also lack protective levels of circulating antitoxin against diphtheria (10-13). Toxoid indications. All adults lacking a complete primary series of diphtheria and tetanus toxoids should complete the series with Td. A primary series for adults is three doses of preparations containing tetanus and diphtheria toxoids, with the first two doses given at least 4 weeks apart and the third dose given 6-12 months after the second. Persons who have served in the military can be considered to have received a primary series of diphtheria and tetanus toxoids. The practitioner should be aware that policies of the different branches of the military have varied among themselves and over time. All adults for whom greater than or equal to 10 years have elapsed since completion of their primary series or since their last booster dose should receive a booster dose of Td. Thereafter, a booster dose of Td should be administered every 10 years. Doses need not be repeated if the primary schedule for the series or booster doses is delayed. The recommended pediatric schedule for DTP includes a booster dose at age 4-6 years. The first Td booster is recommended at age 14-16 years (10 years after the dose at age 4-6 years). One means of ensuring that persons continue to receive boosters every 10 years is to vaccinate persons routinely at mid-decade ages (e.g., 25 years of age, 35 years of age). For wound management, the need for active immunization, with or without passive immunization, depends on the condition of the wound and the patient's vaccination history. A summary of the indications for active and passive immunization is provided in Table_8. Only rarely have cases of tetanus occurred among persons with a documented primary series of toxoid injections. Evidence indicates that complete primary vaccination with tetanus toxoid provides long-lasting protection (greater than or equal to 10 years among most recipients). Consequently, after complete primary tetanus vaccination, boosters are recommended at 10-year intervals. For clean and minor wounds occurring during the 10-year interval, no additional booster is recommended. For other wounds, a booster is appropriate if the patient has not received tetanus toxoid within the preceding 5 years. Antitoxin antibodies develop rapidly in persons who have previously received at least two doses of tetanus toxoid. Persons who have not completed a full primary series of injections or whose vaccination status is unknown or uncertain may require tetanus toxoid and passive immunization at the time of wound cleaning and debridement. Ascertaining the interval since the most recent toxoid dose is not sufficient. A careful attempt should be made to determine whether a patient has previously completed primary vaccination and, if not, how many doses have been given. Persons with unknown or uncertain previous vaccination histories should be considered to have had no previous tetanus toxoid doses. In managing the wounds of adults, Td is the preferred preparation for active tetanus immunization. This toxoid preparation is also used to enhance protection against diphtheria, because a large proportion of adults are susceptible. Thus, if advantage is taken of visits for care of acute health problems, such as for wound management, some patients who otherwise would remain susceptible can be protected against both diseases. Primary vaccination should ultimately be completed for persons documented to have received fewer than the recommended number of doses, including doses given as part of wound management. If passive immunization is needed, human tetanus immune globulin (TIG) is the product of choice. The currently recommended prophylactic dose of TIG for wounds of average severity is 250 units IM. When T or Td and TIG are given concurrently, separate syringes and separate sites should be used. Most experts consider the use of adsorbed toxoid mandatory in this situation. Toxoid Side Effects and Adverse Reactions Local reactions (usually erythema and induration, with or without tenderness) can occur after Td is administered. Fever and other systemic symptoms are less common. Arthus-type hypersensitivity reactions, characterized by severe local reactions starting 2-8 hours after an injection and often associated with fever and malaise, may occur, particularly among persons who have received multiple boosters of tetanus toxoid, adsorbed (T). Rarely, severe systemic reactions, such as generalized urticaria, anaphylaxis, or neurologic complications, have been reported after administration of tetanus and diphtheria toxoids. Peripheral neuropathy has been reported rarely after administration of T, although a causal relationship has not been established. Toxoid Precautions and Contraindications Although no evidence suggests that diphtheria and tetanus toxoids are teratogenic, waiting until the second trimester of pregnancy to administer Td is a reasonable precaution. A history of a neurologic reaction or a severe hypersensitivity reaction (e.g., generalized urticaria or anaphylaxis) after a previous dose is a contraindication to diphtheria and tetanus toxoids. Local side effects alone do not preclude continued use. If a prior systemic reaction suggests allergic hypersensitivity, appropriate skin testing to document immediate hypersensitivity may be useful before T vaccination is discontinued. Protocols exist for using both Td and single-antigen tetanus toxoids for skin testing (15). Mild, nonspecific skin-test reactivity to T toxoid is common. Most vaccinees develop a delayed but inconsequential cutaneous hypersensitivity to the toxoid. Persons experiencing severe Arthus-type hypersensitivity reactions to a dose of T usually have very high serum tetanus antitoxin levels and should not be given even emergency booster doses of Td more frequently than every 10 years. If a contraindication to using preparations containing T exists in a person who has not completed a primary immunizing course of T and other than a clean minor wound is sustained, only passive immunization should be given using TIG. Although a minor illness, such as a mild upper respiratory infection, should not be cause for postponing vaccination, a severe febrile illness is reason to defer routine vaccination. Live-Virus Vaccines Measles Before the introduction of measles vaccine in 1963, approximately 500,000 cases of measles and 500 measles-associated deaths were reported annually in the United States. Because of the widespread use of measles vaccine, the number of reported measles cases decreased to an all-time low of 1,497 in 1983. From 1984 through 1988, the annual number of reported measles cases averaged 3,600, which represents <1% of the cases reported annually in the prevaccine era. In 1989 and 1990, a substantial increase in cases was reported, primarily because of a large number of outbreaks among unvaccinated preschool-age children and vaccinated high-school and college- age students. The 27,786 cases provisionally reported in 1990 represent the largest number of cases reported in any year since 1978. Measles cases were reported from 49 states and the District of Columbia. Adults greater than or equal to 20 years of age accounted for 22% of cases, of which 67% were not appropriately vaccinated (unvaccinated with vaccine indicated). Twenty- five percent of these adults with measles required greater than or equal to 1 day of hospitalization. A provisional total of 130 measles-associated deaths was reported in 1989 and 1990; 36 (28%) of these were persons greater than or equal to 20 years of age. At least 267 measles outbreaks were reported; 17 (6%) occurred on college campuses. Two percent of reported cases were among college students or were epidemiologically linked to campus outbreaks. Encephalitis or death follows measles disease in approximately one case per 1,000. Aside from infants, the risk of encephalitis is greatest among adult patients. Measles illness during pregnancy increases rates of spontaneous abortion, premature labor, and low birth weight for infants. Although cases of congenital malformation after measles infection during pregnancy have been reported, no specific syndrome has been demonstrated. Measles vaccine. Measles vaccine produces a mild or inapparent noncommunicable infection. A single subcutaneously administered dose of live measles vaccine provides durable protection against measles illness for greater than or equal to 95% of susceptible children vaccinated at greater than or equal to 15 months, extending probably for their lifetime. The vaccine of choice is MMR. Vaccine indications. All adults born in 1957 or later who do not have a medical contraindication should receive one dose of measles vaccine unless they have a dated record of vaccination with at least one dose of live measles vaccine on or after their first birthday, documentation of physician-diagnosed disease, or laboratory evidence of immunity. Most persons born before 1957 can be considered immune and do not need vaccination. Of all measles cases reported to CDC from 1985 through 1990, 96.3% occurred among persons born in 1957 or later. However, because a small proportion will be susceptible, vaccine should be offered to such individuals, particularly health-care workers, if there is reason to believe that they may be susceptible. Serologic studies of hospital workers indicate that up to 9.3% of persons born before 1957 were not immune to measles (4,5). Ninety-seven (29%) of 341 health-care workers who developed measles in the period 1985-1989 were born before 1957 (6). As noted above, a single dose of live measles vaccine given on or after the first birthday can be expected to provide long-lasting immunity to measles in at least 95% of recipients. In most situations, a high rate of vaccination resulting in 95% of the population being immune is sufficient to prevent transmission of measles. However, in some circumstances, 5% susceptibility provides enough nonimmune persons to sustain transmission of measles. This situation occurs most commonly in school and college settings, where large numbers of young adults congregate. Other circum- stances in which transmission may occur despite high levels of immunity are in hospitals and other health-care facilities and among persons traveling in places where measles is endemic. In these situations, assuring high levels of immunity to measles among vaccinees by providing a second dose of measles vaccine is desirable. The two-dose schedule is expected to provide protection to most persons who do not respond to their initial vaccination. Entrants into colleges, universities, and other institutions of post- high school education as well as employees in health-care facilities who do not have evidence of immunity to measles (documented physician-diagnosed measles or laboratory evidence of immunity) should be required to provide documentation of two doses of measles vaccine on or after their first birthday. Use of MMR is preferred for both vaccine doses to assure immunity to all three viruses. Individuals who have no documentation of ever having received any doses of measles vaccine and who do not have other evidence of measles immunity should be given one dose of measles vaccine on entry into college or when beginning employment; they should be revaccinated with a second dose not less than 1 month later. If feasible, colleges and health- care facilities may wish to extend this requirement to all students and employees. During outbreaks of measles in schools, colleges, or health-care facilities, all persons born in 1957 or later who cannot provide evidence of receiving two doses of measles vaccine or other evidence of measles immunity should receive one dose of measles-containing vaccine. Those persons should receive their second dose of vaccine not less than 1 month later. Because some medical personnel who have acquired measles in medical facilities were born before 1957, vaccination of older employees who may have occupational exposure to measles should also be considered during outbreaks. An estimated 600,000-900,000 persons in the United States received killed measles vaccine in the period 1963-1967. Individuals who received killed measles vaccine, killed measles vaccine followed within 3 months by live measles vaccine, measles vaccine of unknown type in the period 1963-1967, or vaccine before their first birthday should be considered unvaccinated and should receive at least one dose of live measles vaccine. If these persons are beginning college or other post-high school education or beginning employment in a medical setting, they should receive two doses of measles vaccine at least 1 month apart, as described above. Because the risk of acquiring measles outside the United States is greater than the risk incurred in the United States, travelers should be immune to measles before leaving the United States. Consideration should be given to providing a dose of measles vaccine to persons born during or after 1957 who travel abroad, who have not previously received two doses of measles vaccine, and who do not have other evidence of measles immunity. Young adults who are exposed to measles and who have no or uncertain documentation of live measles vaccination on or after their first birthday, no record of physician-diagnosed measles, and no laboratory evidence of immunity should be vaccinated within 72 hours after exposure; vaccination is most likely to be protective during that time. If the exposure did not result in infection, the vaccine should induce protection against subsequent measles infection. An acceptable alternative is to use immune globulin (IG), which can prevent or modify infection if administered within 6 days after exposure. This alternative is principally indicated when measles vaccine is contraindicated. IG should not be used in an attempt to control measles outbreaks. The recommended dose of IG is 0.25 mL/kg IM, not to exceed 15 mL. Live measles vaccine should be given 3 months after IG is administered, by which time the passive measles antibodies should have disappeared. Because postexposure vaccination or administration of IG is not completely effective, medical personnel should be removed from patient contact 5-21 days after exposure. Vaccine side effects and adverse reactions. A temperature of greater than or equal to 103 F (39.4 C) may develop among approximately 5%-15% of vaccinees, usually beginning between the fifth and twelfth days after vaccination; fever usually lasts 1-2 days and, rarely, up to 5 days. Rashes have been reported among approximately 5% of vaccinees. Encephalitis after measles vaccination is extremely rare, and its incidence cannot be discerned from the background incidence rate of encephalitis of an unknown etiology. The incidence of postvaccination encephalitis is much lower than the incidence after natural measles. Reactions after live measles vaccination occur among 4%-55% of prior recipients of killed measles vaccine. The reactions are generally mild, consisting of a local reaction with or without a low-grade fever of 1-2 days duration. Such reactions can be fairly severe but are milder than atypical measles syndrome, an illness that may affect prior recipients of killed measles vaccine who are exposed to natural measles. No evidence suggests increased risk from live measles vaccination among persons who are already immune to measles as a result of either previous vaccination or natural disease. Vaccine precautions and contraindications. Vaccination should not be postponed because of a minor illness, such as a mild upper-respiratory infection. However, vaccination of persons with severe febrile illnesses should be postponed until recovery. Vaccine should be given 14 days before -- or deferred for at least 6 weeks and preferably 3 months after -- a person has received IG, whole blood, or other blood products containing antibody. Because of a theoretical risk to the developing fetus, measles vaccine should not be given to pregnant women. Measles vaccine also should not be given to persons who are immunocom- promised as a result of immune deficiency diseases, leukemia, lymphoma, or generalized malignancy or who are immunosuppressed as a result of therapy with corticosteroids, alkylating drugs, antimetabolites, or radiation. However, persons with leukemia who are in remission and have not received chemotherapy for at least 3 months and HIV-infected persons should be vaccinated against measles, if considered susceptible. (See "Conditions that Compromise the Immune System" and Table_5 and Table_6.) No evidence suggests that live measles vaccine exacerbates tuberculosis. If tuberculin skin testing is needed, the testing should be done on the day of vaccination and read 48-72 hours later. A recent vaccinee should wait 4-6 weeks after receiving measles vaccine before a tuberculin skin test is administered, because measles vaccination may temporarily suppress tuberculin reactivity. Persons with a history of any sign or symptom of an anaphylactic reaction (e.g., hives, swelling of the mouth and throat, difficulty breathing, hypotension, or shock) after ingestion of eggs or receipt of neomycin should be given measles vaccine only with extreme caution. Protocols have been developed for vaccinating such persons (16). Persons with reactions that are not anaphylactic are not at increased risk and can be vaccinated. Mumps The reported occurrence of mumps cases in the United States has decreased steadily since the introduction of live mumps vaccine. In 1985, a record low of 2,982 cases was reported; this number represented a 98% decline from the 185,691 cases reported in 1967, the year live mumps vaccine was licensed. However, reported cases increased to 7,790 in 1986, followed by 12,848 cases in 1987. In 1988, 1989, and 1990, totals of 4,866, 5,712, and 5,075 cases, respectively, were reported. Largely because of expense, mumps vaccine was not recommended by the ACIP for routine use until 1977, which led to the development of a relatively underimmunized cohort of teenagers and young adults (17). Data from the U.S. Immunization Survey suggest that only approximately 50% of persons of college age in 1986 had received mumps vaccine. In 1989, 38% of reported mumps cases for whom age was known occurred among persons greater than or equal to 15 years of age, compared with 12% in 1977. Although mumps disease is generally self limiting, meningeal signs may appear in up to 15% of cases, and orchitis in 20%-30% of clinical cases among postpubertal males. Sterility is a rare sequela of mumps orchitis among males. Unilateral sensorineural deafness occurs at a rate of one case per 20,000 cases of mumps. Mumps vaccine. Live mumps vaccine has been available since 1967. A single dose of live mumps vaccine administered SC provides protective and long-lasting levels of antibody in >90% of recipients. Clinical vaccine efficacy reports range between 75% and 95%. If recipients are likely to be susceptible to measles and/or rubella as well as to mumps, MMR is the vaccine of choice. Vaccine indications. Mumps vaccine is indicated for all adults believed to be susceptible. Persons should be considered susceptible to mumps unless they have documentation of physician-diagnosed mumps, adequate immunization with live mumps vaccine on or after their first birthday, or laboratory evidence of immunity. Most adults born before 1957 are likely to have been infected naturally and can be considered immune, even if they did not have clinically recognizable mumps disease. Killed mumps vaccine was available from 1950 until 1978. Persons who received killed mumps vaccine might benefit from vaccination with live mumps vaccine. Revaccination with MMR is recommended under certain circumstances for measles (see "Measles" section) and may also be important for mumps because recent studies have shown that mumps can occur in highly vaccinated populations. Persons who are unsure of their mumps disease/vaccination history should be vaccinated. Vaccine side effects and adverse reactions. Parotitis and fever after vaccination have been reported rarely. Allergic reactions including rash, pruritus, and purpura have been associated temporally with mumps vaccination but are uncommon, usually mild, and of brief duration. The frequency of reported central nervous system (CNS) dysfunction after mumps vaccination is not greater than the observed background incidence rate in the general population. Because of the recommendation to use MMR for revaccination against measles, many persons will receive two doses of live mumps vaccine. No evidence suggests an increased risk from live mumps vaccination among persons who are already immune to mumps as a result of either previous vaccination or natural disease. Vaccine precautions and contraindications. Vaccine should be given at least 14 days before, or deferred for at least 6 weeks -- and preferably 3 months -- after a person has received IG, whole blood, or other blood products containing antibody. Because of the theoretical risk of fetal harm after administration of a live-virus vaccine to a pregnant woman, avoiding administering mumps vaccine to pregnant women is prudent. Mumps vaccine should not be given to persons who are immunocompromised as a result of immune deficiency diseases, leukemia, lymphoma, or generalized malignancy or to persons who are immunosuppressed as a result of therapy with corticosteroids, alkylating drugs, antimetabolites, or radiation. Mumps vaccine should be given to asymptomatic HIV-infected individuals and may be considered for those who are symptomatic. (See "Conditions that Compromise the Immune System" and Table_5 and Table_6.) Persons with a history of any sign or symptom of an anaphylactic reaction (e.g., hives, swelling of the mouth and throat, difficulty breathing, hypotension, or shock) after ingestion of eggs or receipt of neomycin should be vaccinated only with extreme caution. Protocols have been developed for vaccinating persons with severe egg allergy (16). Persons with reactions that are not anaphylactic are not at increased risk and can be vaccinated. Rubella Preventing fetal infection and consequent CRS are the objectives of rubella immunization. Fetal infection occurring during the first trimester of pregnancy can lead to CRS in up to 80% of fetuses. Also, fetal death because of miscarriage or therapeutic abortion after maternal rubella disease or exposure during the first trimester continues to occur frequently. The number of reported rubella cases has decreased steadily from >56,000 cases in 1969, the year rubella vaccine was licensed, to 225 cases in 1988. Until the mid-1970s, the strategy was to vaccinate all children; this strategy dramatically reduced the incidence of rubella but had less impact on older age groups, resulting in an increased proportion of cases in adolescents and adults. During the period 1976-1979, >70% of the reported rubella cases occurred among persons greater than or equal to 15 years of age. During 1980 to 1990, this percentage varied widely, reaching a low of 38% in 1988. However, a fivefold increase in rubella incidence occurred between 1988 and 1990. Provisional data indicate that incidence rose sharply among persons greater than or equal to 15 years of age to approximately 57% of 931 cases (with known age) in 1990. A cluster of at least 11 CRS cases among infants born in 1990 was reported to the National CRS Registry. Increased efforts to increase delivery of vaccine to college- age and older persons have led to the current decline in the incidence rates for these age groups. However, an estimated 6%-11% of young adults remain susceptible to rubella, and limited outbreaks continue to be reported in universities, colleges, and places of employment -- notably hospitals. Vaccination of young children has prevented widespread epidemics of rubella and of CRS and eventually will lead to the elimination of CRS as vaccinated cohorts enter the childbearing age. However, increased efforts to ensure that all adults, particularly women of childbearing age, are vaccinated will hasten the elimination of rubella and CRS in the United States. Additional aids to eliminate rubella and CRS include achieving and maintaining high vaccination levels, maintaining vigorous surveillance, and practicing aggressive outbreak control. Rubella vaccine. A single SC-administered dose of live, attenuated rubella vaccine provides long-term (probably lifetime) immunity among approximately 95% of vaccinees. Moreover, there has been no identified transmission of vaccine virus in studies of >1,200 susceptible household contacts of vaccinees and in >20 years of experience with live rubella vaccine. If recipients are likely to be susceptible to measles and/or mumps as well as to rubella, MMR is the vaccine of choice. Vaccine indications. Rubella vaccine is recommended for adults, particularly females, unless proof of immunity is available (i.e., documented rubella vaccination on or after the first birthday or positive results from a serologic test) or unless the vaccine is specifically contraindicated. In particular, nonpregnant susceptible women of childbearing age should be provided rubella vaccination a) during routine internal medicine and gynecologic outpatient care, b) during routine care in a family planning clinic, c) after premarital screening, d) before discharge from a hospital for any reason, and e) after childbirth or abortion. Ideally, any contact with the health-care system should be used as an opportunity to vaccinate susceptible women. Also, evidence of rubella immunity should be required for all persons in colleges and universities. Health-care programs in workplaces and in other places where women of childbearing age congregate should ensure that the vaccination status of every employee is evaluated and that rubella vaccination is made available. All hospital personnel (male and female) who might be at risk of exposure to patients infected with rubella or who might have contact with pregnant patients or personnel should be immune to rubella. Consideration should be given to making rubella immunity a condition for employment. Finally, since the risk of acquiring rubella while traveling outside the United States is greater than the risk incurred within the United States, all women travelers, particularly those of childbearing age, should be immune before leaving the United States. Vaccine side effects and adverse reactions. Up to 25% of susceptible postpubertal female vaccinees in large-scale field trials have had arthralgia after vaccination; arthritis signs and symptoms occur transiently among 10% of recipients. Arthralgia and transient arthritis occur more frequently and tend to be more severe among susceptible women than among seropositive women and children. When joint symptoms or other types of pain and paresthesias do occur, they usually begin 1-3 weeks after vaccination, persist from 1 day to 3 weeks, and rarely recur. Adults with joint problems usually have not had to disrupt work activities. Sporadic cases of persistent joint symptoms among susceptible vaccinees, primarily adult women, have been reported. Although one group of investigators has reported the frequency of chronic joint symptoms and signs among adult women to be as high as 5%-11% (18,19), other data from the United States and experience from other countries that use the RA 27/3 strain suggest that such phenomena are rare. In comparative studies, the frequency of chronic joint complaints is substantially higher after natural infection than after vaccination (19). Complaints of transient peripheral neuritis, such as paresthesias and pain in the arms and legs, have occurred very rarely and only among susceptible vaccinees; these symptoms rarely persist. Because a two-dose schedule of MMR is being implemented in the United States, some persons will receive two doses of rubella vaccine. There is no conclusive evidence of any increased risk of the reactions described above for persons who are already immune when vaccinated. Vaccine precautions and contraindications. Rubella vaccine should be given at least 14 days before administration of IG or deferred for at least 6 weeks -- and preferably 3 months -- after administration. On the other hand, previous administration of whole blood or other blood products containing antibody (e.g., human anti-Rho {D} IG) does not interfere with an immune response and is not a contraindication to postpartum vaccination. However, in this situation, serologic testing should be done 6-8 weeks after vaccination to assure that seroconversion has occurred. Rubella vaccine should not be given to pregnant women or to those likely to become pregnant within 3 months after receiving the vaccine. Through 1988, CDC monitored prospectively 305 susceptible pregnant women who had received rubella vaccine within 3 months before or after conception and carried their pregnancies to term. Ninety-four received Cendehill or HPV-77, 210 received RA 27/3, and one received an unknown strain of vaccine. None of the infants had malformations compatible with CRS. The ACIP believes that the risk of vaccine-associated malformation is so small as to be negligible. Although a final decision must rest with the individual patient and her physician, the ACIP believes that rubella vaccination during pregnancy should not ordinarily be a reason to recommend interruption of pregnancy. Because of the theoretical risk to the fetus, reasonable precautions should be taken before women of childbearing age are vaccinated. These precautions include a) asking women if they are pregnant, b) excluding those who say they are, and c) explaining the theoretical risks of the vaccine to the others and counseling them not to become pregnant for 3 months after vaccination. If a pregnant woman is vaccinated or if a woman becomes pregnant within 3 months after vaccination, she should be counseled on the theoretical risks to the fetus. Rubella vaccine should not be given to persons who are immunocom- promised as a result of immune deficiency diseases, leukemia, lymphoma, or generalized malignancy or who are immunosuppressed as a result of therapy with corticosteroids, alkylating drugs, antimetabolites, or radiation. HIV infection is an exception; rubella vaccine should be given to asymptomatic HIV-infected persons and may be considered for those who are symptomatic. (See "Conditions that Compromise the Immune System" and Table_5 and Table_6.) Rubella vaccine is prepared in human diploid cell cultures and has rarely been reported to be associated with allergic reactions. The vaccine does contain trace amounts of neomycin to which patients may be allergic. Persons with a history of any sign or symptom of an anaphylactic reaction (e.g., hives, swelling of the mouth and throat, difficulty breathing, hypotension, or shock) after receipt of neomycin should not receive rubella vaccine. Persons with reactions to neomycin that are not anaphylactic are not at increased risk and can be vaccinated. Rubella vaccine does not contain penicillin. Smallpox (Vaccinia) In May 1980, the World Health Organization (WHO) declared the world free of smallpox (vaccinia). A smallpox vaccination certificate is not required by any country as a condition of entry for international travelers. In May 1983, the distribution of vaccine for civilian use in the United States was discontinued. Vaccine indications. Only laboratory personnel working with orthopox viruses and certain health-care workers involved in clinical trials of vaccinia recombinant vaccines may need to be given smallpox vaccine. Otherwise, there are no indications for its use in civilian populations. No evidence suggests that smallpox vaccination has therapeutic value in the treatment of recurrent herpes simplex infection, warts, or any other disease. Smallpox vaccine should never be used therapeutically for these or any other conditions. When indicated, smallpox vaccination should be given every 10 years. For advice on vaccine administration and contraindications, contact the CDC Drug Service, Building 1, Room 1259, CDC, Atlanta, GA 30333, telephone: 404-639-3356, or the Division of Immunization, CDC Mailstop (E05), Atlanta, GA 30333, telephone: 404-639-1870. Varicella Zoster Most adults (85%-95%) with negative or unknown histories of varicella (chickenpox) are likely to be immune. Primary varicella can be more severe among adults than it is among normal (immunocompetent) children; however, the risk of serious complications among normal adults is substantially less than it is among those who are immunocompromised. Live, attenuated varicella-zoster vaccine may be licensed for use in normal children in the near future. Its potential use among adults, particularly health-care workers, has not been defined. Yellow Fever Cases of yellow fever are reported only from Africa and South America. Two forms of yellow fever -- urban and jungle -- are distinguishable epidemiologically. Clinically and etiologically, the two forms are identical. Urban yellow fever is an epidemic viral disease transmitted from infected to susceptible persons by the Aedes aegypti mosquito. In areas where the Ae. aegypti mosquito has been eliminated or suppressed, urban yellow fever has disappeared. However, periodic reinfestations of some countries in Central and South America have occurred in recent years, and other countries remain infested. In West Africa, an Ae. aegypti-transmitted epidemic involving an urban population occurred as recently as 1987. Jungle yellow fever is an enzootic viral disease transmitted among nonhuman hosts by a variety of mosquito vectors. Only in forested areas of South America and forest-savannah zones of tropical Africa has it been observed, but it occasionally extends into Central America and the island of Trinidad. In South America, 100-300 cases are recognized annually, mainly among persons with occupational exposure in forested areas; the disease is, however, believed to be greatly underreported. In Africa, sporadic endemic cases and epidemics that affect thousands of persons are spread by forest mosquito vectors. The cycle of jungle yellow fever may be active but unrecognized in forested areas of countries within the endemic yellow fever zone (Figure_1). Yellow fever vaccine. The yellow fever vaccine available in the United States is an attenuated, live-virus vaccine prepared from the 17D strain of virus grown in chick embryos. Immunity is induced by a single SC injection of 0.5 mL of reconstituted vaccine and persists for >10 years. Yellow fever vaccines must be approved by WHO and administered at an approved Yellow Fever Vaccination Center. Centers can be identified by contacting state and local health departments. Vaccinees should have an International Certificate of Vaccination filled out, dated, signed, and validated with the stamp of the center where the vaccine is given. Vaccine must be received 10 days to 10 years before travel for the certificate to be valid. Vaccine indications. Vaccination is recommended for persons traveling or living in areas in which yellow fever infection occurs -- currently parts of Africa and Central and South America. Information on known or probably infected areas is published annually in "Health Information for International Travel". Countries currently reporting yellow fever are noted biweekly in "Summary of Health Information for International Travel" (see page 11). All state health departments and many county and city health departments receive these publications. The actual areas of yellow fever activity far exceed the zones officially reported to be infected. Vaccination is also recommended for laboratory personnel who might be exposed to virulent yellow fever virus. Booster doses are needed at 10-year intervals. Some countries, especially in Africa, require evidence of vaccination from all entering travelers. Other countries may waive the requirements for travelers coming from noninfected areas and staying <2 weeks. Some countries require a traveler, even if only in transit, to have a valid certificate if the traveler has visited any country thought to harbor yellow fever virus. Requirements of individual countries may change, and the most current information is published biweekly in "Summary of Health Information for International Travel" and summarized annually in "Health Information for International Travel" (see page 11). Vaccine side effects and adverse reactions. Reactions to 17D yellow fever vaccine are generally mild. From 2% to 5% of vaccinees have mild headache, myalgia, low-grade fever, or other minor symptoms 5-10 days after vaccination. Fewer than 0.2% curtail regular activities. Immediate hyper- sensitivity reactions, characterized by rash, urticaria, and/or asthma, are extremely uncommon and occur principally among persons with a history of egg allergy. Although >34 million doses of vaccines have been distributed, only two cases of encephalitis temporally associated with vaccinations have been reported in the United States; in one fatal case, 17D virus was isolated from the brain. Vaccine precautions and contraindications. Yellow fever vaccine should not be given to persons who are immunocompromised as a result of immune deficiency diseases (including symptomatic HIV infection), leukemia, lymphoma, or generalized malignancy, or to persons who are immunosuppressed as a result of therapy with corticosteroids, alkylating drugs, antimeta- bolites, or radiation. (See "Conditions that Compromise the Immune System.") Persons who have asymptomatic HIV infection and who cannot avoid potential exposure to yellow fever virus should be offered the choice of vaccination. Although specific information is not available on adverse effects of yellow fever vaccine on the developing fetus, avoiding vaccination of pregnant women and advising that they postpone travel to areas where yellow fever occurs until after delivery seems prudent. Pregnant women who must travel to areas in which the risk of yellow fever is high should be vaccinated. The risk of yellow fever infection far outweighs the small theoretical risk to mother and fetus from vaccination in such circumstances. However, if international travel regulations constitute the only reason to vaccinate a pregnant woman or a patient hypersensitive to eggs, efforts should be made to obtain a letter of waiver from a physician clearly stating the contraindication to vaccination. Ideally, this letter should be written on letterhead stationery and bear the stamp used by health departments and official immunization centers to validate the International Certificates of Vaccination. Under these conditions, travelers should obtain specific, authoritative advice from the country or countries they plan to visit. The countries' embassies or consulates may be contacted and a letter substantiating the waiver of requirements should be obtained. Because live yellow fever vaccine is produced in chick embryos, persons with a history of any signs or symptoms of an anaphylactic reaction (e.g., hives, swelling of the mouth and throat, difficulty breathing, hypotension, or shock) after eating eggs should not receive yellow fever vaccine. If vaccination of an individual with a questionable history of egg hyper- sensitivity is considered essential because of a high risk of exposure, an intradermal (ID) test dose may be administered under close medical supervision. Specific directions for skin testing are found in the package insert. Some data have indicated that persons given yellow fever and cholera vaccines simultaneously or 1-3 weeks apart had lower than normal antibody responses to both vaccines. Unless there are time constraints, cholera and yellow fever vaccines should be administered at a minimum interval of 3 weeks. If the vaccines cannot be administered at least 3 weeks apart, they can be administered simultaneously or at any time within the 3-week interval. Yellow fever vaccine may be given simultaneously with measles, BCG, or hepatitis B vaccines, as well as with IG. Both Live-Virus and Inactivated-Virus Vaccines Poliomyelitis The risk of poliomyelitis is very small in the United States; however, epidemics could occur if the high immunity level of the general population is not maintained by vaccinating children routinely or if wild poliovirus is introduced into susceptible populations in communities with low immunization levels. In the United States, inapparent infection with wild poliovirus strains no longer contributes significantly to establishing or maintaining immunity. Most adults are already immune. Poliovirus vaccines. Two types of poliovirus vaccines are currently licensed in the United States: OPV and eIPV. A primary vaccination series with either vaccine produces immunity to all three types of poliovirus in >95% of recipients. The primary series of OPV consists of three doses: two doses given 6-8 weeks apart and a third dose given at least 6 weeks and customarily 12 months after the second. The primary series for eIPV consists of three doses: two doses each given 4-8 weeks apart and a third dose given 6-12 months after the second. A primary vaccine series need not be given to adults living in the United States who have not had a primary series as children. However, for adults who have not had a primary series and who are at greater risk of exposure than the general population to wild polioviruses because of foreign travel or health occupation, eIPV is preferred because the risk of OPV-associated paralysis is slightly higher among adults than among children. Poliovirus vaccine is not routinely recommended for persons older than high school age (greater than or equal to 18 years old). Vaccine indications. Travelers to areas where wild poliovirus is epidemic or endemic should have completed a primary series of poliovirus vaccine. For previously unvaccinated adults, eIPV is indicated. However, if <4 weeks is available before protection is needed, a single dose of OPV or eIPV is recommended. Travelers who have previously received less than a full primary course of OPV or IPV should be given the remaining required doses of either vaccine, regardless of the interval since the last dose and the type of vaccine previously received. Travelers to developing countries who have previously completed a primary series of OPV should receive a single dose of OPV. Those who have previously received a primary series of IPV should receive a dose of either OPV or eIPV. The need for further doses of either vaccine has not been established. Health-care personnel in close contact with patients who may be excreting wild polioviruses and laboratory personnel handling specimens that may contain wild polioviruses should have completed a primary series of poliovirus vaccine. Because of the slightly increased risk to adults of vaccine-associated paralysis after OPV administration, eIPV is indicated; also, virus may be shed after receipt of OPV vaccine and may inadvertently expose susceptible immunocompromised contacts to live vaccine virus. Vaccine adverse reactions Inactivated poliovirus vaccine. No serious side effects of currently available eIPV have been documented. Because eIPV contains trace amounts of streptomycin and neomycin, hypersensitivity reactions are possible among persons sensitive to these antibiotics. Persons with signs and symptoms of an anaphylactic reaction (e.g., hives, swelling of mouth and throat, difficulty breathing, hypotension, or shock) after receipt of streptomycin or neomycin should not receive eIPV. Persons with reactions that are not anaphylactic are not at increased risk and may be vaccinated. Oral poliovirus vaccine. In rare instances, administration of OPV has been associated with paralysis among healthy recipients and their contacts. Although the risk of vaccine-associated paralytic poliomyelitis is extremely small for immunologically normal vaccinees (approximately one case per 1.4 million first doses distributed and one case per 41.5 million subsequent doses) and for their susceptible immunologically normal household contacts (approximately one case per 1.9 million first doses distributed and one case per 13.8 million subsequent doses), vaccinees should be informed of this risk (20). Vaccine precautions and contraindications Inactivated poliovirus vaccine. No convincing evidence of adverse effects of eIPV for the pregnant woman or developing fetus exists; regardless, theoretically vaccination of pregnant women should be avoided. However, if immediate protection against poliomyelitis is needed, OPV, not eIPV, is recommended. Oral poliovirus vaccine. Unlike other live-virus vaccines that are administered parenterally, OPV is administered orally. IG and other antibody-containing blood products do not appear to interfere with the immune response to OPV. OPV should not be administered to persons who are or may be immuno- compromised as a result of immune deficiency diseases, HIV infection, leukemia, lymphoma, or generalized malignancy or to persons who are or may be immunosuppressed as a result of therapy with corticosteroids, alkylating drugs, antimetabolites, or radiation. (See "Conditions that Compromise the Immune System.")If polio vaccination is indicated for immunosuppressed patients, their household members, or other close contacts, these persons should be given eIPV rather than OPV. Although OPV has not been harmful when administered to asymptomatic HIV-infected children, eIPV is the vaccine of choice if the patient is known or suspected to be infected. The use of eIPV not only eliminates any theoretical risk to the vaccinee but also prevents the possibility of vaccine virus spread to immunocompromised close contacts. Although a protective immune response cannot be assured in the immunocompromised patient, some protection may be provided. OPV should not be used for vaccinating household contacts of patients immunocompromised as a result of immune deficiency disease, HIV infection, leukemia, lymphoma, or generalized malignancy or for vaccinating patients immunosuppressed as a result of therapy with corticosteroids, alkylating drugs, antimetabolites, or radiation. If protection is indicated, eIPV should be used for vaccinating household contacts of such patients. OPV should not be given to anyone in a family with a known family history of immunodeficiency until the immune status of all family members is documented. When children in the household receive OPV, adults who are not adequately vaccinated against poliomyelitis are at a very small risk of contracting OPV-associated paralytic poliomyelitis. Because of the overriding importance of ensuring prompt and complete vaccination of the child and the extreme rarity of OPV-associated disease in contacts of vaccinees, the ACIP recommends the administration of OPV to a child, regardless of the poliovirus-vaccine status of adult household contacts. This is the standard practice in the United States. The responsible adult should be informed of the small risk involved and of the precautions to be taken, such as hand washing after changing a diaper. An acceptable alternative, if there is strong assurance that ultimate, full vaccination of the child will not be jeopardized or unduly delayed, is to vaccinate adults with eIPV or OPV, as appropriate to their immunity status, before giving OPV to the child. Inactivated-Virus Vaccines Hepatitis B Virus Infection The estimated lifetime risk of acquiring HBV infection in the United States is approximately 5% for the population as a whole but may approach 100% for the highest risk groups. Annually, an estimated 300,000 HBV infections occur in the United States, leading to approximately 10,000 hospitalizations and 250 deaths due to fulminant hepatitis B. In 1988, 89% of HBV cases for which the patient's age was known occurred among persons greater than or equal to 20 years of age. Between 6% and 10% of adults with HBV infection become carriers. The United States currently has 750,000-1,000,000 carriers. Chronic active hepatitis occurs among an estimated 25% of carriers. Each year in the United States, approximately 4,000 persons die of HBV-related cirrhosis and 800 of HBV- related liver cancer. Hepatitis B vaccine. Two types of HB vaccines are currently licensed in the United States. Plasma-derived HB vaccine consists of a suspension of inactivated, alum-adsorbed 22-nm HBsAg particles that have been purified from human plasma. Although still available, plasma-derived vaccine is no longer being produced in the United States. Currently licensed recombinant HB vaccines are produced by Saccharomyces cerevisiae (common baker's yeast), into which a plasmid containing the gene for the HBsAg has been inserted. These vaccines contain >95% HBsAg protein. Dosages of vaccines vary with manufacturer and age of the recipient. Package inserts should be consulted for proper dosages. Both types of vaccines are given as three-dose series, with the first two doses given 1 month apart, and the third dose 5 months after the second. An alternative schedule for one vaccine, with three doses 1 month apart followed by a fourth dose 12 months after the first, has been approved for postexposure prophylaxis or for more rapid induction of immunity. However, no clear evidence that this regimen offers greater protection than the standard schedule exists. Duration of protection from HB vaccines is at least 7 years among healthy adults; the possible need for booster doses will be assessed as further information becomes available. Because the prevalence of HBV infection varies widely among various population groups, serologic screening to detect susceptible individuals before vaccination may or may not be cost effective. Cost-effectiveness depends on the known or expected prevalence of immune individuals in the target population, the cost of screening, and the cost of HB vaccine. Postvaccination testing for immunity is not recommended routinely but is advised for persons whose subsequent management depends on knowing their immune status (dialysis patients and staff) and for those in whom suboptimal response is anticipated (persons with HIV infection and those who have received vaccine in the buttock). When indicated, such testing should be done within 1-6 months after completing vaccination. Postvac- cination testing should also be considered for health-care workers at risk of needlestick exposures. If such testing demonstrates an antibody level <10 mIU/mL, revaccination with one or more doses should be considered. Vaccine indications. Vaccination is recommended for adults at increased risk of occupational, social, family, environmental, or illness- related exposure to HBV. These include homosexual males, injecting drug users, heterosexual persons with multiple partners or other sexually transmitted diseases, household and sexual contacts of HBV carriers, workers in health-related and public-safety occupations requiring frequent exposure to blood, residents and staff of institutions for the develop- mentally disabled, hemodialysis patients, recipients of factor VIII or IX concentrates, and morticians and their assistants. Inmates in some long- term correctional facilities may also be candidates for vaccination. Vaccination should also be considered for persons who plan to reside for >6 months in areas with high levels of endemic HBV and who will have close contact with the local population and for travelers intending a short stay who are likely to have contact with blood from or sexual contact with residents of areas with high levels of endemic disease (particularly areas of eastern Asia and sub-Saharan Africa). Such persons should allow 6 months before travel to complete the HB vaccine primary series. The alternative four-dose schedule may offer better protection if three doses can be given before travel. HB vaccine is intended primarily for preexposure prophylaxis; however, it has been recommended for postexposure use in certain situations, particularly for nonimmune persons who belong to a high-risk group for whom preexposure administration of vaccine is recommended (21). HB vaccine, in combination with HBIG, provides sustained protective levels of antibody and obviates the need for a second dose of HBIG in such exposures. Therefore, a normal series of HB vaccine, combined with a single dose (0.06 mL/kg or 5 mL for adults) of HBIG given at a different site, is recommended for postexposure prophylaxis of nonimmune (and previously unvaccinated) health workers after accidental percutaneous or mucous-membrane exposure to blood containing HBsAg, and after all sexual exposure to HBsAg-positive persons if the first dose of vaccine can be administered within 14 days of sexual exposure or if sexual contact with the infected person will continue. Vaccine side effects and adverse reactions. The most common side effect observed after vaccination with each of the available vaccines has been soreness at the injection site. Postvaccination surveillance for 3 years after licensure of the plasma-derived vaccine showed an association of borderline significance between Guillain-Barre syndrome (GBS) and receipt of the first vaccine dose (22). The rate of this occurrence was very low (0.5/100,000 vaccinees), and, even if a true side effect, was more than compensated for by disease prevented by the vaccine. Such postvac- cination surveillance information is not available for the recombinant HB vaccines. Early concerns about safety of plasma-derived vaccine, particularly the concern that infectious agents such as HIV present in the donor plasma pools might contaminate the final product, have proved to be unfounded. Vaccine precautions and contraindications. Pregnancy should not be considered a contraindication to vaccinating women who are otherwise candidates for receiving HB vaccine. Although data are not available on the safety of the vaccine for the developing fetus, HB vaccine contains only noninfectious HBsAg particles and should pose no risk to the fetus. In contrast, HBV infection in a pregnant woman may result in a severe disease for the mother and chronic infection for the newborn. Influenza Influenza viruses have continually demonstrated the ability to cause major epidemics of respiratory disease. High attack rates of acute illness and the frequent occurrence of lower respiratory tract complications usually result in dramatic rises in visits to physicians' offices and hospital emergency rooms. Furthermore, influenza frequently infects individuals who, because of their age or underlying health status, are poorly able to cope with the disease and often require medical attention, including hospitalization. Such persons are considered, medically, to be at "high risk" in epidemics. In one recent study, for example, rates of hospitalization for adults with high-risk medical conditions increased during major epidemics by approximately twofold to fivefold in different age groups, reaching a maximum rate of about 800/100,000 population. Influenza epidemics cause excess mortality that is attributable not only to influenza pneumonia but also to cardiopulmonary disease. Nineteen times in the period 1957-1986 epidemics have been associated with greater than or equal to 10,000 excess deaths. Approximately 80%-90% of the excess deaths attributed to pneumonia and influenza were among persons greater than or equal to 65 years of age during major epidemics. Influenza has its greatest impact when new strains appear against which most of the population lacks immunity. In these circumstances (e.g., 1957 and 1968), pandemics occur. During pandemics, one-fourth or more of the U.S. population has been affected over a period of 2-3 months. Because the proportion of elderly persons in the United States is increasing and because age and its associated chronic diseases are risk factors for severe influenza illness, the toll of influenza may also increase unless control measures are used more vigorously than in the past. Influenza vaccine. Influenza A viruses are classified into subtypes on the basis of two antigens: hemagglutinin (H) and neuraminidase (N). Three subtypes of hemagglutinin (H1, H2, H3) and two subtypes of neuraminidases (N1, N2) are recognized among influenza A viruses that have caused widespread human disease. Immunity to these antigens, especially hemagglutinin, reduces the likelihood of infection and the severity of disease if a person does become infected. However, sufficient antigenic variation (antigenic drift) within the same subtype over time may exist, so that infection or vaccination with one strain may not induce immunity to distantly related strains of the same subtype. Although influenza B viruses have shown much more antigenic stability than influenza A viruses, antigenic variation does occur. As a consequence, the antigenic characteristics of current strains provide the basis for selecting virus strains to be included in the vaccine for a given year. The potency of present vaccines is such that nearly all vaccinated young adults develop hemagglutination-inhibition antibody titers that usually protect them against infection by strains like those in the vaccine, and often by related variants that emerge. The elderly, the very young, and patients with certain chronic diseases may develop lower antibody titers after vaccination than do young adults. Under these circumstances, influenza vaccine may be more effective in preventing lower- respiratory-tract involvement or other complications of influenza than in preventing upper-respiratory-tract involvement. Influenza vaccine will not prevent primary illnesses caused by other respiratory pathogens. Vaccine indications. Use of inactivated influenza vaccine is the single most important measure in preventing and attenuating influenza infection. Since 1963, annual vaccination against influenza has been recommended for individuals at high risk of lower-respiratory-tract complications and death after influenza infection (i.e., the elderly and persons with chronic disorders of the cardiovascular, pulmonary, and/or renal systems; metabolic diseases; severe anemia; and/or compromised immune function, including HIV infection). These groups have been identified primarily by review of death certificate data, supported by hospital-based or population-based studies. Within each broadly defined high-risk category, however, some persons are more likely than others to suffer severe complications from influenza infection. Among nursing-home residents, chronic diseases and other debilitating conditions are common, and influenza can often be spread explosively, with attack rates as high as 60% and case-fatality ratios greater than or equal to 30%. Medical personnel, while working, may transmit influenza infections to their high-risk patients while they themselves are incubating an infection, undergoing a subclinical infection, or having mild symptoms. Nosocomial outbreaks of influenza have been reported. The potential for introducing influenza to a high-risk group, such as patients with severely compromised cardiopulmonary or immune systems or infants in neonatal intensive care units, should be reduced by targeted vaccination programs of medical personnel. On the basis of these observations, the previous, broadly defined high- risk adult groups have been assigned further priority for receiving vaccine so that special efforts can be directed at providing vaccine to those who may derive the greatest benefit. Groups at increased risk for influenza-related complications. To maximize protection of high-risk persons, both the persons at risk and their close contacts should be targeted for organized vaccination programs. These include the following:
persons. Care-givers of or household members attending high-risk persons can transmit influenza infections to them while they themselves are undergoing subclinical or symptomatic infection. Some high-risk persons (e.g., the elderly, transplant recipients, or persons with acquired immunodeficiency syndrome {AIDS}) can have relatively low antibody responses to influenza vaccine. Efforts to protect them against influenza may be improved by reducing the chances that their care providers may expose them to influenza. Therefore, the following groups should be vaccinated:
essential community service, to any adult who wishes to reduce the likelihood of an influenza infection, to the elderly, or to those with high-risk conditions who travel to areas with active influenza disease. Vaccination of other groups. Pregnant women who have other medical conditions that increase their risks for complications from influenza should be vaccinated, as the vaccine is considered safe for pregnant women. Administering the vaccine after the first trimester is a reasonable precaution to minimize any concern over the theoretical risk of terato- genicity. However, delaying vaccination of pregnant women who have high- risk conditions and who will still be in the first trimester of pregnancy when the influenza season begins is undesirable. Little information exists on the frequency and severity of influenza illness among HIV-infected persons, but recent reports suggest that symptoms may be prolonged and the risk of complications increased for this high-risk group. Therefore, vaccination is a prudent precaution and will result in protective antibody levels among many recipients. However, the antibody response to vaccine may be low in persons with advanced HIV- related illnesses. A booster dose of vaccine has not improved the immune response for these individuals. Strategies for implementing influenza vaccine recommendations. Effective programs for giving influenza vaccine are needed in nursing homes and other chronic-care facilities, in physicians' offices, and in hospital settings. Residents of nursing homes and chronic-care facilities should receive routine annual vaccinations. Other adult high-priority groups should receive influenza vaccine at the time of regular medical follow-ups in the autumn or should be notified to come in specifically to receive the vaccine. Patients with high-risk conditions who are hospitalized during the autumn should be considered for influenza vaccine before being discharged from the hospital. The target groups for receiving influenza and pneumococcal polysaccharide vaccine overlap considerably. These vaccines can be given at the same time at different sites without an increase in side effects or compromise in immunogenicity; however, influenza vaccine is given annually, whereas pneumococcal polysaccharide vaccine is not given more often than every 6 years to adults. Amantadine hydrochloride, an antiviral drug, can prevent influenza A or be used therapeutically to reduce symptoms of influenza A infections. It is not a substitute for vaccine. Specific circumstances in which amantadine prophylaxis is recommended are described in the ACIP recommendations on prevention and control of influenza. (See Appendix 1.) Vaccine side effects and adverse reactions. Vaccines used in recent years have been associated with infrequent reactions. Local redness or induration for 1 or 2 days at the site of injection has reportedly developed among fewer than one-third of vaccinees. Systemic reactions have been of two types. First, malaise, myalgia, and other systemic symptoms of toxicity, although infrequent, most often affect those who have had no experience with the influenza virus antigens contained in the vaccine. These reactions, which begin 6-12 hours after vaccination and persist 1-2 days, are usually attributed to the influenza antigens (even though the virus is inactivated) and constitute most of the systemic side effects of influenza vaccination. Second, immediate, presumably allergic responses, such as flare and wheal or various respiratory tract symptoms of hypersensitivity, occur extremely rarely after influenza vaccination. These symptoms probably result from sensitivity to some vaccine component -- most likely residual egg protein. Although current influenza vaccines contain only a small quantity of egg protein, vaccine can induce hypersensitivity reactions on rare occasions. Unlike the 1976 swine influenza vaccine, vaccines used subsequently have not been clearly associated with an increased frequency of GBS. Vaccine precautions and contraindications. Persons with a history of any signs or symptoms of an anaphylactic reaction (e.g., hives, swelling of the mouth and throat, difficulty breathing, hypotension, or shock) after eating eggs should not be given inactivated influenza vaccine. Persons with acute febrile illnesses normally should not be vaccinated until their symptoms have abated. Rabies Although rabies rarely affects humans in the United States, approxi- mately 18,000 persons receive rabies vaccine every year for postexposure prophylaxis, and an additional 10,000 persons receive preexposure prophylaxis. The likelihood of human exposure to rabies from domestic animals has decreased greatly in recent years. In every year since 1976, >85% of all reported cases of animal rabies have been among wild animals, the most important source of possible infection for humans in the United States. However, for persons traveling overseas to developing countries with endemic rabies, the dog remains the animal most likely to transmit the disease. Rabies vaccine. Two inactivated rabies vaccines are currently licensed for preexposure and postexposure prophylaxis in the United States. HDCV is supplied in two forms: a) for IM administration (single-dose vials containing lyophilized vaccine that is reconstituted in the vial with the accompanying diluent to a final volume of 1.0 mL just before adminis- tration), and b) for ID administration (single-dose syringes containing lyophilized vaccine that is reconstituted in the syringe to a volume of 0.1 mL just before administration). Rabies vaccine adsorbed (RVA), prepared from the Kissling strain of rabies virus adapted to fetal rhesus lung diploid cell culture, was licensed in 1988. Developed and distributed by the Biologics Products Program, Michigan Department of Public Health, RVA is currently available only to residents of the state of Michigan. Rabies vaccine derived from human diploid cell developed in the United States (Wyeth-Ayerst Laboratories, WYVAC) was recalled from the market in 1985 and is no longer available. Preexposure prophylaxis, consisting of three 1.0-mL injections of HDCV or RVA, should be given IM (deltoid), one each on days O, 7, and 28. Alternatively, using the specially designed syringe, three 0.1-mL injections of HDCV (but not RVA) may be given ID in the deltoid on days 0, 7, and 21 or 28 (23). The proper postexposure rabies prophylaxis regimen depends on whether the person has had previous preexposure or postexposure prophylaxis. Persons who a) have previously received postexposure prophylaxis with HDCV or RVA, b) have received a three-dose IM preexposure regimen of HDCV or RVA, c) have received a three-dose ID preexposure regimen of HDCV in the United States, or d) have a previously documented adequate rabies titer should receive two 1-mL IM doses of HDCV -- one dose each on days 0 and 3. Human rabies immune globulin (HRIG) is not recommended in these circumstances. Persons not meeting the above criteria should be treated with a single 20-IU/kg dose of HRIG and five 1-mL doses IM of HDCV -- one each on days 0, 3, 7, 14, and 28. HRIG should be administered at the beginning of HDCV postexposure prophylaxis but can be given up to the eighth day after the first dose of HDCV was given. The HRIG dose should be divided. Up to half should infiltrate the area of the wound, if possible, and the rest should be administered IM, but never in the same site or in the same syringe as HDCV. Only IM administration of HDCV is indicated for postexposure prophylaxis. Among adults, only the deltoid area is acceptable for vaccine administration. Vaccine indications. Preexposure immunization should be considered for high-risk groups: animal handlers, certain laboratory workers and field personnel, and persons planning to spend more than 1 month in areas of countries where rabies is a constant threat. Persons whose vocations or avocations bring them into contact with potentially rabid animals, including skunks, raccoons, and bats, should also be considered for preexposure vaccination. Persons with continuing risk of exposure should receive a booster dose every 2 years, or they should have their serum tested for rabies antibody every 2 years and, if the titer is inadequate, receive a booster dose. If substantial risk of exposure to rabies exists, preexposure rabies prophylaxis may be indicated during pregnancy. The decision to provide postexposure antirabies treatment should include the following considerations:
pain, erythema, and swelling or itching at the injection site, are reported by up to 74% of recipients. Mild systemic reactions, such as headache, nausea, abdominal pain, muscle aches, and dizziness, are reported by between 5% and 40% of recipients. After primary vaccination, systemic allergic reactions ranging from hives to anaphylaxis occur among an estimated 11 of 10,000 vaccinees. After booster doses, mild immune-complex- like hypersensitivity reactions consisting of hives, itching, and angioedema occur 2-21 days later among approximately 6% of recipients and are the most frequently reported allergic reactions (24). Fewer than 1% of persons develop such reactions after primary administration of HDCV. Two cases of neurologic illness resembling GBS that resolved without sequelae in 12 weeks have been reported -- as well as a number of different subacute central and peripheral nervous system disorders temporally associated with HDCV vaccine, but a causal relationship has not been established (25). Vaccine precautions and contraindications. Corticosteroids and other immunosuppressive agents can interfere with the development of active immunity and should not be administered during preexposure therapy. When rabies postexposure prophylaxis is administered to persons known or suspected of being immunosuppressed or to those who are receiving steroids or immunosuppressive therapy, the serum should be tested to ensure an adequate rabies antibody response. Chloroquine phosphate administered for malaria chemoprophylaxis and unidentified factors among persons living in developing countries may interfere with the antibody response to HDCV among persons traveling to developing countries (26). Among persons receiving preexposure prophylaxis and chloroquine in preparation for travel to an area in which rabies is enzootic, the administration of the 0.1-mL dose ID should be initiated at least 1 month before travel to allow the three-dose series to be completed before antimalarial prophylaxis begins. If this is not possible, the 1.0-mL dose should be administered IM. If person experiences a possible anaphylactic reaction (e.g., hives, swelling of the mouth and throat, difficulty breathing, hypotension, or shock) after receiving HDCV, no further preexposure doses of HDCV should be given. In contrast, if a person needing postexposure therapy has had a previous anaphylactic reaction to HDCV or has such a reaction during the postexposure course, public health officials should be contacted to determine if HDCV therapy should continue. The person should receive the subsequent doses in an appropriate medical setting. Inactivated-Bacteria Vaccines Cholera Cholera continues to be a health risk in Africa, Asia, and Latin America. Persons who follow the usual tourist itinerary and who use tourist accommodations in countries affected by cholera are at virtually no risk of infection. The traveler's best protection against cholera is avoiding food and water that might be contaminated. Cholera vaccine. The vaccine may be administered as a 0.5-mL dose SC or IM or as a 0.2-mL dose ID. Although a single dose of vaccine is sufficient for entry into most countries, some countries may require evidence of a complete primary series of two doses given 1 week to greater than or equal to 1 month apart, or a booster dose within 6 months before arrival. The currently available cholera vaccine has been shown in field trials to be only approximately 50% effective in preventing clinical illness for a period of 3-6 months. The vaccine does not prevent transmission of infection. The risk of cholera to most U.S. travelers is so low that the vaccination is of dubious benefit. WHO no longer recommends cholera vaccination for travel to or from cholera-infected areas. However, some countries affected or threatened by cholera may require evidence of cholera vaccination as a condition of entry. Current information on cholera- vaccination requirements of individual countries is published annually in "Health Information for International Travel" (see page 11). All state health departments and many county and city health departments receive this publication. Travelers to countries with cholera-vaccination requirements should have an International Certificate of Vaccination completed, dated, signed, and validated, showing receipt of the vaccine 6 days-6 months before entry into the country. Most city, county, and state health departments can validate certificates. Failure to secure validation may cause travelers to be revaccinated or quarantined. Vaccine indications. Cholera vaccine is indicated for travelers to countries requiring evidence of cholera vaccination for entry. In addition, the complete primary series is suggested only for special high-risk groups that live in areas in which cholera is highly endemic under insanitary conditions. Boosters may be given every 6 months if required by a country. Vaccine side effects and adverse reactions. Vaccination often results in 1-2 days of pain, erythema, and induration at the site of injection. The local reaction may be accompanied by fever, malaise, and headache. Serious reactions, including neurologic reactions, after cholera vaccination are extremely rare. Vaccine precautions and contraindications. No specific information is available on the safety of cholera vaccine during pregnancy. Because cholera disease during pregnancy is a serious illness, whether to use cholera vaccine should be determined in individual circumstances based on the actual risk of disease and the probable benefits of the vaccine. The only contraindication to cholera vaccine is a history of a severe reaction after a previous dose. Most governments will permit unvaccinated travelers to enter the country if they carry a physician's statement of medical contraindication. However, some countries may quarantine such unvaccinated persons or place them under surveillance if they come from areas with cholera. Some data have indicated that persons given yellow fever and cholera vaccines simultaneously or 1-3 weeks apart had lower than normal antibody responses to both vaccines. Unless there are time constraints, cholera and yellow fever vaccines should be administered at a minimal interval of 3 weeks. If the vaccines cannot be administered at least 3 weeks apart, they can be given simultaneously or anytime within the 3-week interval. Haemophilus influenzae type b Healthy adults are not at increased risk of invasive Hib disease. Over 85% of invasive H. influenzae cases occur among children <5 years of age (27). Among adults, invasive H. influenzae disease occurs primarily among persons with chronic pulmonary disease and underlying conditions that predispose to infections with encapsulated bacteria. Hib bacteria cause less than half the cases of invasive H. influenzae disease among adults. Nontypeable H. influenzae bacteria are a more common cause of invasive disease, such as pneumonia in adults, as well as of mucosal infections, such as otitis media and bronchitis. Haemophilus influenzae type b vaccine. The Hib vaccines available include three polysaccharide protein conjugate vaccines licensed during the period 1987-1989. The conjugate vaccines are known to be more immunogenic among children <2 years of age and among immunocompromised persons than the polysaccharide polyribosyl-ribitol-phosphate (PRP) vaccine, licensed in 1985. For this reason, this PRP vaccine is no longer being produced in the United States. Vaccine indications. No data documenting the efficacy of any Hib vaccine among children >5 years of age or adults exist. This includes those persons with underlying conditions (e.g., splenectomy, sickle cell disease, Hodgkin disease and other hematologic neoplasms, and immunosuppression) that predispose to infections with encapsulated bacteria. Studies suggest, however, good immunogenicity among patients with sickle cell disease (28) or leukemia (29) and among adults who have had splenectomies (30) or HIV infection (31,32). Because of the theoretical risk to such patients, physicians may wish to consider use of HbCV among individuals with functional or anatomic asplenia or with HIV infection. Administering Hib vaccine to such patients is not contraindicated. One study reported 12 (100%) of 12 healthy adults and 20 (87%) of 23 patients who had undergone splenectomies responded with protective levels of antibody to conjugate vaccine, although the antibody levels were significantly lower among the splenectomized patients (30). Because healthy adults are not at risk for invasive Hib disease, routinely vaccinating health-care and day care workers who may come into close contact with children with invasive Hib disease is unnecessary. Rifampin prophylaxis is recommended for all household and day care contacts of cases of invasive Hib disease, including children and adults, when there are any children <4 years of age (households) or <2 years of age (day care classrooms) in the exposed group. Although not at risk themselves, adults who have been exposed to a child with invasive Hib disease in a household or day care setting may be asymptomatic carriers of the organism and can transmit it to other susceptible children. Pregnant women should not receive rifampin, because its effect on the fetus has not been established and it is teratogenic among laboratory animals. Vaccine side effects and adverse reactions. In one study of children 15-24 months of age, local reactions were noted for 12.5% of children receiving conjugate vaccine; moderate fever (temperature >39.0 C {>102.2 F}) occurred among 0.7% of children (33). In a study of 35 children >9 years of age and of adults who received conjugate vaccine (30) (23 of whom had had Hodgkin disease and had had surgical splenectomy), 3 (8.5%) of the 35 complained of systemic side effects: weakness, nausea and vertigo (1), myalgias (2), and fever (1). Vaccine precautions and contraindications. The safety of HbCV for pregnant women has not been established. On theoretical grounds, avoiding vaccination of pregnant women unless there is a substantial risk of infection (e.g., anatomic or functional asplenia or HIV infection) is prudent. Meningococcal Disease Meningococcal disease is endemic throughout the world but may also occur in epidemics. Among U.S. civilians, meningococcal disease occurs primarily as single, isolated cases, or, infrequently, in small, localized clusters. One-third of all cases of meningococcal disease occur among patients greater than or equal to 20 years old. Serogroup B and C strains cause the majority of U.S. cases, with serogroups Y and W135 accounting for most of the rest. Meningococcal polysaccharide vaccine. One meningococcal polysaccharide vaccine, a quadrivalent A, C, Y, and W135 vaccine, is available for use in the United States. The vaccine is given as a single dose and induces serogroup-specific immunity of unknown duration. Vaccine indications. Vaccine may be of benefit for travelers to areas with epidemic meningococcal disease. Vaccine may also be used in aborting and controlling outbreaks caused by serogroups represented in the vaccine. In addition, the ACIP recommends the vaccine for individuals with terminal complement component deficiencies and those with anatomic or functional asplenia. The need for booster doses has not been established. Routine vaccination of U.S. civilians with meningococcal polysaccharide vaccine is not recommended because of the lack of availability of a group B vaccine and the low risk of infection in the United States. Vaccine side effects and adverse reactions. Adverse reactions to meningococcal polysaccharide vaccine are infrequent and mild, consisting principally of localized erythema lasting 1-2 days. Vaccine precautions and contraindications. The safety of meningococcal polysaccharide vaccine for pregnant women has not been established. On theoretical grounds, avoiding it unless there is a substantial risk of infection is prudent. Plague Plague is a natural infection of rodents and their fleas. In the United States, an average of 19 cases has been reported yearly between 1979 and 1988 among humans exposed in the western United States to infected animals (primarily rodents) and their fleas. Other countries currently reporting plague infections are noted in the biweekly publication "Summary of Health Information for International Travel" (see page 11). All state health departments and many county and city health departments receive this publication. A number of countries in Africa, Asia, and South America continue to report sporadic, epidemic, and epizootic infection. In most of these countries, the risk of exposure exists primarily in rural or semirural areas. Plague vaccine. A primary series of plague vaccine consists of three IM doses. The first dose, 1 mL, is followed in 4 weeks by a second dose of 0.2 mL. The third dose, also 0.2 mL, is administered 5 months after the second. The effectiveness of a primary series of plague vaccine has never been measured precisely. Field experience indicates that vaccination with plague vaccine reduces the incidence and severity of disease resulting from the bite of infected fleas. The degree of protection offered against primary pneumonic infection is unknown. Because plague vaccination may only ameliorate illness, prophylactic antibiotics may be indicated whenever a person, vaccinated or not, has a definite exposure. Vaccine indications. Vaccination is indicated for certain vocational groups. These include all laboratory and field personnel working with Y. pestis organisms that may be resistant to antimicrobials, persons engaged in aerosol experiments with Y. pestis, and field personnel engaged in operations in areas with enzootic or epidemic plague in which preventing exposure to rodents and fleas is impossible. Vaccine may also be considered for travelers to areas known to have endemic plague, particularly if travel will not be limited to urban areas with tourist-hotel accommodations. For persons with continuing exposure, two booster doses, each 0.1-0.2 mL, should be given approximately 6 months apart. Thereafter, booster doses at 1- to 2-year intervals should provide good protection. Vaccine side effects and adverse reactions. For approximately 10% of recipients, primary vaccination may result in general malaise, headache, fever, mild lymphadenopathy, and/or erythema and induration at the injection site. These reactions occur more commonly with repeated injections. Sterile abscesses occur rarely. Sensitivity reactions, manifested by urticarial and asthmatic phenomena, have occasionally been reported. Vaccine precautions and contraindications. Neither the safety nor the efficacy of vaccination with plague vaccine during pregnancy has been determined; therefore, it should not be used unless there is a substantial risk of infection. Plague vaccine should not be administered to anyone with a known hyper- sensitivity to any of its constituents (beef protein, soy, casein, and phenol). Patients who have had severe local or systemic reactions to plague vaccine should not be revaccinated. Pneumococcal Disease Precise data on the occurrence of serious pneumococcal disease in the United States are not available; however, the annual incidence rate of pneumococcal bacteremia is estimated to be 15-19 cases/100,000 population for all persons, and 50 cases/100,000 for persons greater than or equal to 65 years old. The incidence of pneumococcal pneumonia, which causes a substantial number of deaths annually, can be three to five times that of the detected rates of bacteremia. Mortality from all pneumococcal disease, estimated at 40,000 deaths annually in the United States, is highest among patients who have bacteremia or meningitis, patients with underlying medical conditions, and older persons. Patients with certain chronic conditions are at increased risk of pneumococcal infection and severe pneumococcal illness. Patients with chronic cardiovascular diseases, chronic pulmonary disease, diabetes mellitus, alcoholism, and cirrhosis have increased risk. Other patients at elevated risk include those with functional or anatomic asplenia (e.g., sickle cell disease or splenectomy), Hodgkin disease, lymphoma, multiple myeloma, chronic renal failure, nephrotic syndrome, and organ transplantation. Patients with AIDS are also at increased risk of pneumococcal disease, with an annual attack rate of pneumococcal bacteremia as high as 9.4/1,000/year (34). Recurrent pneumococcal meningitis may occur among patients with cerebrospinal fluid leakage that is complicating skull fractures or neurologic procedures. Pneumococcal polysaccharide vaccine. The pneumococcal polysaccharide vaccine currently available contains purified capsular materials of the 23 types of S. pneumoniae responsible for 88% of recent bacteremic pneumo- coccal disease in the United States. Most healthy adults show a two-fold rise in type-specific antibody 2-3 weeks after administration of a single dose of vaccine. The titer of antibody that is protective against each serotype has not been determined. The duration of vaccine-induced immunity is unknown. Studies of persistence of vaccine-induced antibody show elevated titers 5 years after vaccination among healthy adults. Estimates of pneumococcal vaccine efficacy have varied widely in several studies. Studies based on CDC's pneumococcal surveillance system suggest an efficacy of 60%-64% for vaccine-type strains among patients with bacteremic disease. For all persons greater than or equal to 65 years of age, vaccine efficacy was 44%-61%. Three case-control studies that have emphasized complete assessment of vaccination status suggest a range of efficacy against pneumococcal bacteremia from 61% to 81%. Despite findings of varying efficacy, the data continue to support the use of the pneumococcal vaccine for certain well-defined groups at risk. Patients who have received the earlier pneumococcal polysaccharide vaccine containing capsular material from only 14 types of Streptococcus pneumoniae should not be routinely revaccinated with the 23-valent pneumococcal polysaccharide vaccine, as the increased coverage is modest. However, revaccination should be strongly considered greater than or equal to 6 years after the first dose for those at highest risk of rapid decline in antibody levels (i.e., those with chronic renal failure, nephrotic syndrome, or transplanted organs) or of fatal pneumococcal infection (i.e., asplenic patients). Vaccine indications. Available data regarding vaccine efficacy support the broader use of pneumococcal polysaccharide vaccine in the United States. Vaccination is particularly recommended for the following groups:
to be developed further. Specifically, more effective programs are needed for giving vaccine in physicians' offices, hospitals, nursing homes, and other chronic-care facilities. Two-thirds of persons with serious pneumococcal disease have been hospitalized within a 5-year period before the pneumococcal illness (35). Therefore, vaccine should be given to hospitalized patients in the high- risk groups before discharge in order to prevent future admissions for pneumococcal disease. Also, persons with chronic conditions who visit physicians frequently are probably at higher risk of pneumococcal infection than those who require infrequent visits. Office-based programs to identify and vaccinate patients requiring frequent medical care should help prevent pneumococcal illness. Furthermore, pneumococcal polysaccharide vaccine and influenza vaccine can be given at different sites at the same time without an increase in side effects (36). Medicare has partially reimbursed the cost of pneumococcal polysac- charide vaccination since 1981. Hospitals may be reimbursed for pneumo- coccal vaccination of Medicare recipients independent of reimbursement based on systems of prospective payments. Vaccine side effects and adverse reactions. About half the persons given pneumococcal polysaccharide vaccine experience mild side effects such as erythema and pain at the site of injection. Fever, myalgias, and severe local reactions have been reported by <1% of those given pneumococcal polysaccharide vaccine (37). Severe adverse effects such as anaphylactic reactions have rarely been reported approximately five cases per million doses administered. A similar incidence of adverse events after primary vaccination and revaccination has been noted among adults when revac- cination occurs>4 years after primary vaccination (Merck Sharp & Dohme, unpublished data). When the interval between first and second doses was less than or equal to 13 months, local reactions were more severe (38); these reactions are thought to result from localized antigen-antibody reactions involving antibody induced by a previous vaccination. Until more information is available, revaccination should be given only to adults at highest risk of pneumococcal illness, as noted above in the "Vaccine Indications" section. Vaccine precautions and contraindications. The safety of pneumococcal polysaccharide vaccine among pregnant women has not been evaluated. Women at high risk of pneumococcal disease ideally should be vaccinated before pregnancy. Both Inactivated-Bacteria and Live-Bacteria Vaccines Typhoid The occurrence of typhoid fever remained constant in the period 1975-1989, with an average of 447 cases reported annually. During the period 1975-1989, 59% of cases for which the patient's age was known occurred among patients greater than or equal to 20 years of age. Approximately 69% of typhoid cases reported in the United States in 1984 were acquired by travelers to other countries. Typhoid vaccine. A primary series of two 0.5-mL doses of phenol- inactivated typhoid vaccine (given SC) 4 weeks apart has been shown to protect 51%-76% of recipients. A live, attenuated oral typhoid vaccine was licensed in 1989. Its efficacy is approximately 67%, when taken as recommended (four doses on alternate days). An acetone-killed and -dried typhoid vaccine is available only to the U.S. Armed Forces. Vaccine indications. Vaccination is indicated for travelers to areas where a recognized risk of exposure to typhoid exists, although no country requires typhoid immunization for entry. Vaccination is particularly recommended for travelers who will have prolonged exposure to potentially contaminated food and water in smaller villages or rural areas off the usual tourist routes. Further information to guide travelers about typhoid immunization is contained in the publication "Health Information for International Travel" (see page 11). Even after typhoid vaccination, food and water should be selected carefully in these areas. Two other groups for whom selective vaccination is indicated are persons with intimate exposure (i.e., continued household contact) to a documented typhoid carrier and workers in microbiology laboratories who frequently work with Salmonella typhi. Typhoid vaccination is not recommended in the United States for use in areas of natural disaster. Booster doses of the inactivated vaccine should be given at least every 3 years to persons with continued or repeated exposure; these may be administered SC (0.5 mL) or ID (0.1 mL). The optimal booster schedule for live, attenuated Ty21a oral vaccine has not been determined, although efficacy has been shown to persist for 5 years with a four-dose regimen. The manufacturer of Ty21a recommends revaccination with the entire four-dose series every 5 years. No experience with using live, attenuated oral vaccine as a booster among persons who were previously vaccinated with parenteral vaccine exists. The acetone- killed and -dried vaccine, available only to the U.S. Armed Forces, should not be given ID. Vaccine side effects and adverse reactions. Inactivated typhoid vaccine given SC often results in 1-2 days of discomfort at the site of injection. The local reaction may be accompanied by fever, malaise, and headache. Adverse reactions from the oral typhoid vaccine reported to the manufacturer occurred at a rate of <1/100,000 doses administered. Reactions reported consisted of nausea, abdominal cramps, vomiting, and skin rash or urticaria. Vaccine precautions and contraindications. The only contraindication to inactivated typhoid vaccine is a history of a severe local or systemic reaction after a previous dose. Oral typhoid vaccine is not recommended for children <6 years of age or immunocompromised persons, including those with asymptomatic HIV infection. Live-Bacteria Vaccines Tuberculosis The number of tuberculosis cases in the United States has markedly declined since nationwide reporting began in 1953. Between 1972 and 1984, the annual incidence of tuberculosis declined from 15.8 cases/100,000 population to 9.4/100,000, a decrease of 41%. Since 1984, however, the number of cases reported and the case rate have increased. This increase is probably attributable to the occurrence of tuberculosis among persons with HIV infection. In 1989, approximately 92.2% of 23,485 reported cases with patient ages known occurred among persons greater than or equal to 20 years of age. The risk of infection with Mycobacterium tuberculosis is greatest for those who have repeated exposure to persons with unrecognized or untreated sputum-positive pulmonary tuberculosis. In the United States, efforts to control tuberculosis are directed toward early identification and treatment of cases, preventive therapy with isoniazid for infected persons at high risk of disease, and prevention of transmission to others. Bacille Calmette-Guerin vaccine. Although BCG is widely used in many areas of the world, results of a recent large-scale field trial in India have raised questions about its efficacy (39). BCG vaccines currently available in the United States differ from the products used in the published field trials, and their efficacy has not been demonstrated directly. In the United States, vaccines for ID and for percutaneous administration are licensed. (For percutaneous administration, one drop of vaccine is placed on the skin and introduced through the skin by multiple punctures with a bifurcated or other type of needle.) Vaccination should be only by the route indicated on the package labeling. Vaccine indications. In the United States, BCG vaccination is no longer recommended for health-care workers or other adults at high risk for acquiring TB infection. The only situations in which BCG might be considered are for children with negative tuberculin skin tests who fall into the following categories: a) those who cannot be placed on isoniazid preventive therapy but who have continuous exposure to persons with active disease, b) those with continuous exposure to patients with organisms resistant to isoniazid and rifampin, or c) those belonging to groups with exceptionally high annual rates of new infection (i.e., >1% per year). Vaccine side effects and adverse reactions. BCG has been associated with severe or prolonged ulceration at the vaccination site, regional adenitis, disseminated BCG infection, and osteitis. Severe ulceration and adenitis occur among approximately 1%-10% of vaccinees, although disseminated infections and osteitis are quite rare (1-10 per million doses). Vaccine precautions and contraindications. Although no harmful effects of BCG on the fetus have been observed, avoiding vaccination during pregnancy unless there is immediate excessive risk of exposure to infective tuberculosis is prudent. Because BCG is a live-bacteria vaccine, it should not be given to persons immunocompromised as a result of immune deficiency diseases (including HIV infection), leukemia, lymphoma, and generalized malignancy, or to persons immunosuppressed as a result of therapy with corticosteroids, alkylating drugs, antimetabolites, or radiation. (See "Conditions that Compromise the Immune System.") Other Licensed Vaccines Adenovirus and Adenovirus Vaccine Adenovirus types 4 and 7 have frequently been the cause of outbreaks of acute, febrile respiratory tract disease among young adults during military training. Live, oral adenovirus vaccines for types 4 and 7 are available for vaccination of military populations. Use of the vaccines in other populations is not recommended. Anthrax and Anthrax Vaccine Anthrax is infrequently encountered. Anthrax vaccine is recommended only for individuals who come in contact in the workplace with imported animal hides, furs, bonemeal, wool, animal hair (especially goat hair), and bristles and for persons undertaking investigations involving Bacillus anthracis. Primary vaccination consists of six SC 0.5-mL injections, the first three at 2-week intervals and the other three at 6-month intervals. Booster doses of 0.5-mL SC are recommended at 1-year intervals. The vaccine is only available from the Biologic Products Program, Michigan Department of Public Health. Details on reactions and vaccine contraindications are found in the package insert. Immune Globulins IG and specific immune globulins (i.e., HBIG, TIG, HRIG, and varicella- zoster immune globulin {VZIG}) are indicated to prevent or modify certain diseases in specific circumstances. Cytomegalovirus Immune Globulin This is a hyperimmune intravenous preparation that is effective in both prophylaxis (alone) and treatment (with ganciclovir) of cytomegalovirus (CMV) infections in bone marrow and kidney transplant recipients. When used as a prophylactic agent, CMV immune globulin has been used over a period of several months and does not diminish the frequency of CMV infections, but it does limit disease and reduce death rates. Hepatitis B Immune Globulin HBIG, alone or in combination with HB vaccine, is used for postexposure prophylaxis of HBV infection among persons who have not previously received HB vaccine or who are known not to have responded to the vaccine series. For percutaneous or mucous-membrane exposure to blood known to be HBsAg positive or from a bite by an HBV carrier, a single dose of HBIG (0.06 mL/kg or 5 mL for adults) should be administered as soon as possible and a series of three doses of HB vaccine begun within 1 week after exposure. Vaccine and HBIG may be administered simultaneously, but at different sites. For those who choose not to take HB vaccine, a second, identical dose of HBIG should be administered 1 month later. After any percutaneous exposure to blood, serologic confirmation of the HBsAg status of the source patient should be obtained as soon as possible. If the source patient is HBsAg positive, the exposed person should immediately receive HBIG and HB vaccine according to the schedule above. The value of HBIG given beyond 7 days after exposure is unclear. For management of HBsAg-positive percutaneous exposure among persons who have previously received HB vaccine, the ACIP's Recommendations for "Protection of Viral Hepatitis" should be consulted (21) (Table_9). All susceptible persons whose sex partners have acute HBV infection or whose sex partners are discovered to be HBsAg carriers should receive a single dose of HBIG (0.06 mL/kg) and should begin the HB vaccine series if prophylaxis can be started within 14 days of the last sexual contact or if ongoing sexual contact will occur. Administering the vaccine with HBIG may improve the efficacy of postexposure treatment; in addition, the vaccine has the advantage of conferring long-lasting protection. These recommen- dations, along with those for newborn infants exposed to HBsAg-carrier mothers, are listed in Table_10. An alternative treatment for persons who are not from a high-risk group for whom vaccine is routinely recommended and whose regular sex partners have acute HBV infection is to give one dose of HBIG within 14 days of exposure (without vaccine) and retest the sex partner for HBsAg 3 months later. No further treatment is necessary if the sex partner becomes HBsAg negative. If the sex partner remains HBsAg positive, a second dose of HBIG should be administered and the HBV vaccine series started. Human Rabies Immune Globulin Postexposure prophylaxis for rabies should always include HRIG with one exception: persons who have been previously vaccinated with the recommended preexposure or postexposure regimens of HDCV or have been vaccinated with other types of rabies vaccines and have a history of documented adequate rabies antibody titer should not receive HRIG (Table_7). The recommended dose of HRIG is 20 IU/kg body weight. If anatomically feasible, thoroughly infiltrate the area around the wound with up to half the dose of HRIG; the rest of the HRIG should be administered IM. Immune Globulin for Intramuscular Use IG is given IM for preexposure prophylaxis against hepatitis A to travelers in areas where contact with potentially contaminated food and water is anticipated. For travelers at risk for 2-3 months, a single IM dose of 0.02 mL/kg is recommended. For more prolonged travel, 0.06 mL/kg should be administered every 5 months. For persons whose travel repeatedly places them at risk for hepatitis A, testing for antibodies to hepatitis A is useful to identify those who are immune and to eliminate unnecessary doses of IG. IG is also indicated for postexposure prophylaxis for close household and sexual contacts of persons with hepatitis A, staff and attendees of day care centers, household contacts of diapered children in day care centers in which hepatitis A transmission is occurring, selected staff and clients of custodial institutions in which an outbreak is occurring, and co-workers of food handlers with hepatitis A. For such contacts, a single dose of 0.02 mL/kg of IG is recommended as soon as possible after exposure. IG is not effective unless given within 2 weeks after exposure. IG can be used to prevent or modify measles disease in susceptible contacts of persons with measles, especially those for whom measles vaccine is contraindicated, if given within 6 days after exposure. The recommended dose is 0.25 mL/kg, or 0.5 mL/kg for immunocompromised persons (maximum dose = 15 mL in both situations). IG should not be used to control measles outbreaks. Immune Globulin for Intravenous Use IG modified for intravenous (IV) use may be administered to prevent acute infections among patients with defective antibody synthesis or, in unusual situations, as prophylaxis against hepatitis A or measles for patients for whom the IM preparation is contraindicated because of thrombo- cytopenia or disorders that can cause IM hemorrhage. However, no data are available about the efficacy of IG when administered IV in preventing either hepatitis A or measles. Because IG modified for IV use is made from a relatively small pool of donors, it may not contain antibodies to hepatitis A. ONLY IG MODIFIED FOR IV USE CAN BE GIVEN INTRAVENOUSLY. The IV dose is 100 mg/kg, administered slowly. The IV preparation is supplied in 50-mL vials containing 2.5 g of IG. Tetanus Immune Globulin TIG is indicated in tetanus prophylaxis as part of the management of wounds other than clean, minor wounds in persons a) whose previous T toxoid vaccination status is unknown or uncertain or b) who have received fewer than three previous T toxoid doses. The currently recommended prophylactic dose for wounds of average severity is 250 units (U) IM. Td should be administered at the same time but at a separate site. A summary of the indications for active and passive immunization in the management of wounds is provided in Table_8. Vaccinia Immune Globulin Vaccinia immune globulin (VIG) is available only from CDC's Drug Service (404-639-3670) for the treatment of eczema vaccinatum, vaccinia necrosum, and ocular vaccinia developed as a result of smallpox vaccination. VIG is of no benefit in the treatment of postvaccination encephalitis. The recommended dose is 0.6 mL/kg IM to be administered as soon as possible after onset of symptoms. Because therapeutic doses of VIG can be quite large (e.g., 42 mL for a 70-kg person), the doses should be divided over a 24- to 36-hour period. Doses may be repeated at the discretion of the attending physician, usually every 2-3 days, until no new lesions appear. Varicella-Zoster Immune Globulin Most persons with a clearly positive history of previous varicella are probably immune. Most adults (85%-95%) with negative or unknown histories of varicella disease (chickenpox) are likely to be immune. (Susceptibility rates for adults raised in some tropical areas, particularly remote areas, may be somewhat higher.) When available, serologic screening may be used to define susceptibility more precisely. Rates of complications and death for immunocompromised adults who contract varicella are likely to be substantially greater than for normal adults. After being carefully and individually evaluated, an immunocompromised patient who is believed to be susceptible and who has had significant exposure to varicella should receive VZIG to prevent complications. Significant exposure to a person with varicella includes household contact, close contact indoors of >1 hour, sharing the same two- to four- bed hospital room, or prolonged, direct, face-to-face contact such as occurs with nurses or doctors who care for the patient. Chickenpox can be more severe among adults than among normal children. The decision to administer VZIG to a normal adult should be made on an individual basis. The objective of VZIG use for normal adults is to modify rather than prevent illness in the hope of inducing lifelong immunity. When deciding whether to administer VZIG, the clinician should consider the patient's health status, the type of exposure, and the likelihood of previous infection. Adults who were older siblings in large families or whose children have had varicella are probably immune. If, after being carefully evaluated, a normal adult with substantial exposure to varicella is believed to be susceptible, VZIG may be administered. Pregnant women and potentially susceptible hospital personnel should be evaluated in the same way as other adults. Supplies of VZIG are limited, and indiscriminate administration of VZIG to normal adults would quickly exhaust supplies and prevent prophylaxis for known high-risk individuals. The cost of a five- vial adult dose is approximately $400. VZIG, available through some American Red Cross distribution centers (Appendix 6), is supplied in vials containing 125 U. Although 125 U/10 kg of body weight up to a maximum of 625 U is considered likely to prevent or modify varicella among normal adults, higher doses may be necessary for the immunocompromised adult. However, the appropriate dose for immunocom- promised adults has not been determined. VZIG should be administered IM as directed by the manufacturer. Although the duration of protection is unknown, the protection should probably last for at least one half-life of the IG, that is, approximately 3 weeks. Immune Globulin Side Effects and Adverse Reactions Serious adverse effects from immune globulins administered as recommended have been rare. Immune Globulin Precautions and Contraindications IG, if needed, is not contraindicated for pregnant women, Except for its IV preparation, IG is prepared for IM use and should not be given IV. The various preparations intended for IM use should not be given to patients with severe thrombocytopenia or other coagulation disorders that would ordinarily contraindicate IM injections, unless the expected benefits outweigh the risks. Parenterally administered live-virus vaccines (e.g., MMR or other combinations) should be given at least 14 days before, or at least 6 weeks and preferably 3 months after, the administration of IG preparations. If an IG must be administered within 14 days after the administration of most live-virus vaccines, the vaccine should be administered again 3 months after the IG. If the interval between receipt of the vaccine and receipt of the IG is longer, the vaccine need not be readministered. Preliminary data indicate that IG preparations do not interfere with the immune response to either OPV or yellow fever vaccine. No evidence suggests that HBV, HIV, or other viruses have ever been transmitted by the IG or HBIG that is commercially available in the United States (40). Since April 1985, all plasma units for preparation of all IG have been screened for antibody to HIV, and reactive units are discarded. No instance of HIV transmission or clinical illness consistent with HIV infection attributable to receiving IG or HBIG, including lots prepared before April 1985, has been observed. Laboratory studies have shown that the margin of safety based on the removal of HIV infectivity by the fractionation process is extremely high (41). Some HBIG lots prepared before April 1985 have detectable HIV antibody; low levels of passively acquired HIV antibody can occasionally be detected among recipients shortly after administration, but this reactivity does not persist (42).
References
Appendix 1 Table_A1 Appendix 2 Table_A2 Appendix 3 Table_A3 Appendix 4 Table_A4 Appendix 5 Table_A5 Appendix 6
Table_A6
TABLE 1. On the basis of The National Childhood Vaccine Injury Act of 1986 (NCVIA), the vaccines and toxoids, adverse
events, and intervals from vaccination to onset of adverse event required for reporting or compensation, United States
======================================================================================================================================================
Interval from vaccination to onset of event
-----------------------------------------------------------------
Vaccine/toxoid * Adverse event For reporting + For compensation &
--------------------------------------------------------------------------------------------------------------------------------
DTP, P, A. Anaphylaxis or 24 hours 24 hours
DTP/Poliovrrus anaphylactic shock
combined B. Encephalopathy (or 7 days 3 days
encephalitis) @
C. Shock-collapse or 7 days 3 days
hypotonic-hyporesponsive
collapse **
D. Residual seizure disorder ++ ++ 3 days
E. Any acute complication or No limit Not applicable
sequela (including death)
of above events
F. Events described as (See package insert) &&
contraindications to additional
doses of vaccine (see manufacturer's
package insert) &&
Measles, A. Anaphylaxis or 24 hours 24 hours
Mumps, and anaphylactic shock
Rubella; B. Encephalopathy (or 15 days (for measles, mumps, 15 days for measles,
DT, Td, T encephalitis) @ and rubella vaccines); mumps, and rubella vaccine;
7 days (for DT, Td, and T) 3 days (for DT, Td, and T)
C. Residual seizure disorder ++ ++ 15 days (for measles,
mumps, or rubella vaccine);
3 days for DT, Td, or T)
D. Any acute complication or No limit
sequela (including death)
of above events
E. Events described as contraindications (See package insert) &&
to additional doses of vaccine
(see manufacturer's package insert) &&
OPV A. Paralytic poliomyelitis
in a nonimmunodeficient 30 days 30 days
recipient
in an immunodeficient 6 months 6 months
recipient
in a vaccine-associated No limit Not applicable
community case
B. Any acute complication or No limit Not applicable
sequela (including death)
of above events
C. Events described as contrain- (See package insert) &&
dications to additional doses
of vaccine (see manufacturer's
package insert) &&
Inactivated A. Anaphylaxis or 24 hours 24 hours
Polio anaphylactic shock
Vaccine B. Any acute complication or No limit Not applicable
sequela (including death)
of above events
C. Events described as contrain- (See package insert) &&
dications to additional doses
of vaccine (see manufacturer's
package insert) &&
--------------------------------------------------------------------------------------------------------------------------------
* The vaccine/toxoid abbreviations are defined, in alphabetical order, as follows: DT = Diphtheria and tetanus toxoids, adsorbed; DTP =
Diphtheria and tetanus toxoids and pertussis vaccine, adsorbed (pediatric); OPV = Oral poliovirus vaccine, live, trivalent; P = Pertussis
vaccine; T = Tetanus toxoid, adsorbed; and Td = Tetanus and diphtheria toxoids, adsorbed (for adult use).
+ Adverse events that are required by NCVIA to be reported to Vaccine Adverse Events Reporting System (VAERS) if their onset is within the
indicated interval after vaccination.
& Adverse events that may be compensable under NCVIA if the onset is within this interval after vaccination.
@ Encephalopathy means any significant acquired abnormality of, injury to, or impairment of function of the brain. Among the frequent
manifestations of encephalopathy are focal and diffuse neurologic signs, increased intracranial pressure, or changes lasting at least 6 hours
in level of consciousness, with or without convulsions. The neurologic signs and symptoms of encephalopathy may be temporary with
complete recovery or may result in various degrees of permanent impairment. Signs and symptoms such as high-pitched and unusual
screaming, persistent inconsolable crying, and bulging fontanel are compatible with an encephalopathy, but in and of themselves are not
conclusive evidence of encephalopathy. Encephalopathy usually can be documented by slow wave activity on an electroencephalogram.
** Shock-collapse or hypotonic-hyporesponsive collapse may include signs or symptoms such as decrease or loss of muscle tone, paralysis
(partial or complete), hemiplegia, hemiparesis, loss of color or turning pale white or blue, unresponsiveness to environmental stimuli,
depression of or loss of consciousness, prolonged sleeping with difficulty being aroused, or cardiovascular or respiratory arrest.
++ Residual seizure disorder may have occurred if no other seizure or convulsion unaccompanied by fever or accompanied by a fever of < 102
F occurred before the first seizure or convulsion after the administration of the vaccine involved, and if, in the case of measles-, mumps-, or
rubella-containing vaccines, the first seizure or convulsion occurred within 15 days after vaccination, or, in the case of any other vaccine, the
first seizure or convulsion occurred within 3 days after vaccination, and, if two or more seizures or convulsions unaccompanied by fever or
accompanied by a fever of <102 F occurred within 1 year after vaccination. The terms seizure and convulsion include grand mal, petit mal,
absence, myoclonic, tonic-clonic, and focal motor seizures and signs.
&& Refer to the CONTRAINDICATION section of the manufacturer's package insert for each vaccine/toxoid.
======================================================================================================================================================
Return to top. Table_2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 2. Vaccines and toxoids * recommended for adults, by age groups, United
States
======================================================================================================
Vaccine/toxoid
------------------------------------------------------------------
Age group Pneumococcal
(years) Td + Measles Mumps Rubella Influenza Polysaccharide
--------------------------------------------------------------------------------
18-24 X X X X
25-64 X X & X & X
>=65 X X X
--------------------------------------------------------------------------------
* Refer also to sections in text on specific vaccines or toxoids for indications, contraindications,
precautions, dosages, side effects, adverse reactions, and special considerations.
+ Td = Tetanus and diphtheria toxoids, adsorbed (for adult use), which is a combined
preparation containing <2 flocculation units of diphtheria toxoid.
& Indicated for persons born after 1956.
======================================================================================================
Return to top. Table_3 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 3. Recommended schedule of vaccinations for all children
==============================================================================================
4-6 years
(before begin-
2 months 4 months 6 months 12 months 15 months ing school)
---------------------------------------------------------------------------------
DTP DTP DTP DTP * DTP
Polio Polio Polio * Polio
MMR + MMR &
HbCV:
Option 1 @ HbCV HbCV HbCV
Option 2 @ HbCV HbCV
---------------------------------------------------------------------------------
At birth (before
hospital discharge) 1-2 months 4 months 6-18 months
---------------------------------------------------------------------------------
HBv:
Option 1 HBv HBv ** HBv **
Option 2 HBv ** HBv ** HBv **
---------------------------------------------------------------------------------
DTP: Diphtheria, Tetanus, and Pertussis Vaccine
Polio: LIve Oral Polio Vaccine drops (OPV) or Killed (Inactivated) Polio Vaccine shots (IPV)
MMR: Measles, Mumps, and Rubella Vaccine
HbCV: Haemophilus infuenzae type b Conjugate Vaccine
HBv: Hepatitis B vaccine
* Many experts recommend these vaccines at 18 months.
+ In some areas this dose of MMR vaccine may be administered at 12 months.
& Many experts recommend this dose of MMR vaccine be administered at entry into middle
school or junior high school.
@ HbCV vaccine is administered in either a 4-dose schedule (1) or a 3-dose schedule (2),
depending on the type of vaccine used.
** HBv can be administered at the same time as DTP and/or HbCV.
==============================================================================================
Return to top. Table_4 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 4. Immunobiologics * recommended for special occupations, life-styles, envi-
ronmental circumstances, travel, foreign students, immigrants, and refugees, United
States
==========================================================================================================
Indication Immunobiologic
-----------------------------------------------------------------------------
Occupation
Hospital, laboratory, and other Hepatitis B
health-care personnel Influenza
Measles
Rubella
Mumps
Polio
Public-safety personnel Hepatitis B
Influenza
Staff of institutions for the Hepatitis B
developmentally disabled
Veterinarians and animal handlers Rabies
Plague
Selected field workers Plague
(those who come into contact with Rabies
possibly infected animals)
Selected occupations Anthrax
(those who work with imported
animal hides, furs, wool, animal
hair, and bristles)
Life-styles
Homosexual males Hepatitis B
Injecting drug users Hepatitis B
Heterosexual persons with Hepatitis B
multiple sexual partners or
recently acquired sexually
transmitted disease
Environmental situation
Inmates of long-term correctional Hepatitis B
facilities
Residents of institutions for the Hepatitis B
developmentally disabled
Household contacts of HBV carriers Hepatitis B
Homeless persons Tetanus/diphtheria
Measles
Mumps
Rubella
Influenza
Pneumococcal polysaccharide
Travel + Measles
Mumps
Rubella
Polio
Influenza
Hepatitis B
Rabies
Meningococcal polysaccharide
Tetanus/diphtheria &
Yellow fever
Typhoid
Cholera
Plague @
Immune globulin **
Foreign students, Measles
immigrants, and refugees Rubella
Diphtheria
Tetanus
Mumps
Hepatitis B
-----------------------------------------------------------------------------
* Refer also to sections in text on specific immunobiologics for use by specific risk groups, details
on indications, contraindications, precautions, dosages, side effects, and adverse reactions, and
special considerations. Unless specifically contraindicated, the vaccines or toxoids recom-
mended for adults are also indicated. Table 2 shows vaccines and toxoids appropriate for most
adults by age.
+ Vaccines needed for travelers will vary depending on individual itineraries; travelers should
refer to Health Information for International Travelers for more detailed information (see page 11 ).
& If not received within 10 years.
@ In or during travel to areas with enzootic or epidemic plague in which exposure to rodents
cannot be prevented.
** For Hepatitis A prophylaxis.
==========================================================================================================
Return to top. Table_5 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 5. Vaccines and toxoids * indicated or specifically contraindicated for situa-
tions involving special health status, United States
====================================================================================================
Vaccine/toxoid
-------------------------------------------------------------
Health situation Indicated Contraindicated
------------------------------------------------------------------------------------------
Pregnancy Tetanus/diphtheria Live-virus vaccines
Immunocompromised + Influenza Live-virus vaccines
Pneumococcal polysaccharide Bacille Calmette-Guerin
Haemophilus influenzae type b & Oral typhoid
Splenic dysfunction or Pneumococcal polysaccharide
anatomic asplenia Influenza
Meningococcal polysaccharide
Haemophilus influenzae type b &
Hemodialysis or Hepatitis B @
transplant recipients Influenza
Pneumococcal polysaccharide
Deficiencies of Hepatitis B
factors VIII or IX
Chronic alcoholism Pneumococcal polysaccharide
Diabetes and other Influenza
high-risk diseases Pneumococcal polysaccharide
------------------------------------------------------------------------------------------
* Refer also to sections in text on specific vaccines or toxoids for details on indications,
contraindications, precautions, dosages, side effects and adverse reactions, and special consid-
erations. Unless specifically contraindicated, the vaccines and toxoids recommended for adults
are also indicated. See Table 2 for vaccines and toxoids appropriate for most adults, by age.
+ Recommendations specific to persons infected with human immunodeficiency virus are listed
in Table 6.
& May be considered.
@ These patients will need a higher dose or an increased number of doses; see "Hemodialysis
and Transplantation" section in text.
====================================================================================================
Return to top. Table_6 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 6. Recommendations for routine vaccination of HIV-infected persons *, United
States
====================================================================================================
HIV infection
-------------------------------------------
Vaccine/toxoid + Known asymptomatic Symptomatic
------------------------------------------------------------------------
DTP/Td yes yes
OPV no no
eIPV & yes yes
MMR yes yes @
HbCV ** yes yes
Pneumococcal yes yes
Influenza yes @ yes
------------------------------------------------------------------------
* Appropriate for human immunodeficiency virus (HIV)-infected children and adults.
+ The vaccine/toxoid abbreviations are defined as follows: DTP = Diphtheria and tetanus toxoids
and pertussis vaccine, adsorbed (pediatric); Td = Tetanus and diphtheria toxoids, adsorbed (for
adult use); OPV = Oral poliovirus vaccine; eIPV = Enhanced-potency inactivated poliovirus
vaccine; MMR = Measles, mumps, and rubella vaccine; HbCV = Haemophilus influenzae type
b conjugate vaccine; and Pneumococcal = Pneumococcal polysaccharide vaccine.
& For adults >=18 years of age, use only if indicated. (See text.)
@ Should be considered.
** May be considered for HIV-infected adults (see "Special Health Status: Conditions that
Compromise the Immune System" in text).
====================================================================================================
Return to top. Table_7 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 7. Immunobiologics * and schedules for adults (>=18 years of age) *+, United States
=====================================================================================================================================================
Immunobiologic Primary schedule Major precautions and
generic name and booster(s) Indications contraindications & Special considerations
---------------------------------------------------------------------------------------------------------------------------------------------------
TOXOIDS
Tetanus/diphtheria Two doses intramuscularly All adults. Except in the first trimester, Tetanus prophylaxis in wound
toxoid, adsorbed (IM) 4 weeks apart; third pregnancy is not a contra- management. (See text and
(for adult use) (Td) dose 6-12 months after indication. History of a Table 8.)
second dose. Booster neurologic reaction or
every 10 years. immediate hypersensitivity
reaction following a pre-
vious dose. History
of severe local (Arthus-
type) reaction following
previous dose. Such
individuals should not be
given further routine or
emergency doses of Td
for 10 years.
LIVE-VIRUS VACCINES
Measles vaccine, One dose subcutaneously All adults born after Pregnancy; immunocom- MMR is the vaccine of choice
live (SC); second dose at 1956 without documen- promised persons @; if recipients are likely to be
least 1 month later, tation of live vaccine history of anaphylactic susceptible to rubella and/or
at entry into college on or after first birthday, reactions following mumps as well as to measles.
or post-high school physician-diagnosed egg ingestion or receipt Persons vaccinated between
education, beginning measles, or laboratory of neomycin. (See text.) 1963 and 1967 with a killed
medical facility evidence of immunity; measles vaccine alone, killed
employment, or before persons born before 1957 vaccine followed by live
traveling. Susceptible are generally considered vaccine, or with a vaccine of
travelers should receive immune. unknown type should be revac-
one dose. cinated with live measles virus
vaccine.
Mumps vaccine, One dose SC; no booster. All adults believed to Pregnancy; immunocom- MMR is the vaccine of choice
live be susceptible can be promised persons @; history if recipients are likely to be
vaccinated. Adults born of anaphylactic reaction susceptible to measles and
before 1957 can be following egg ingestion. rubella as well as to mumps.
considered immune. (See text.)
Rubella vaccine, One dose SC; Indicated for adults, Pregnancy; immunocom- Women pregnant when vacci-
live no booster. both male and female, promised persons @; history nated or who become preg-
lacking documentation of of anaphylactic reaction nant within 3 months of vacci-
live vaccine on or after following receipt of nation should be counseled
first birthday or neomycin. on the theoretical risks to the
laboratory evidence of fetus. The risk of rubella
immunity, particularly vaccine-associated malfor-
young adults who work mations in these women is so
or congregate in places small as to be negligible.
such as hospitals, MMR is the vaccine of choice
colleges, and military, if recipients are likely to be
as well as susceptible susceptible to measles or
travelers. mumps as well as to rubella.
Smallpox vaccine THERE ARE NO INDICATIONS FOR THE USE OF SMALLPOX VACCINE IN THE Laboratory workers working
(vaccinia virus) GENERAL CIVILIAN POPULATION. with orthopox viruses or
health-care workers involved
in clinical trials of vaccinia-
recombinant vaccines.
Yellow fever One dose SC 10 days Selected persons travel- Although specific infor- Some countries require a valid
attenuated virus, to 10 years before ing or living in areas mation is not available International Certificate of
live (17D strain) travel; booster every where yellow fever concerning adverse effects Vaccination showing receipt of
10 years. infection exists. on the developing fetus, it vaccine. If the only reason
is prudent on theoretical to vaccinate a pregnant
grounds to avoid vaccinat- woman is an international
ing a pregnant woman requirement, efforts should be
unless she must travel made to obtain a waiver letter
where the risk of yellow (see text).
fever is high.
Immunocompromised
persons @; history of
hypersensitivity to egg
ingestion.
LIVE-VIRUS AND INACTIVATED-VIRUS VACCINES
Polio vaccines: eIPV preferred for Persons traveling to Although there is no con- Although a protective immune
Enhanced potency primary vaccination; areas where wild vincing evidence docu- response to eIPV in the
inactivated polio- two doses SC 4 weeks poliovirus is epidemic menting adverse effects immunocompromised person
virus vaccine apart; a third dose or endemic. Certain of either OPV or eIPV cannot be assured, the
(eIPV) 6-12 months after health-care personnel. on the pregnant woman vaccine is safe, and some
Oral poliovirus second; for adults with (See text for or developing fetus, it protection may result from
vaccine, live a completed primary recommendations for is prudent on theoretical its administration.
(OPV) series and for whom a incompletely vaccinated grounds to avoid vacci-
booster is indicated, adults and adults nating pregnant women.
either OPV or eIPV in households of However, if immediate
can be administered. children to be protection against polio-
If immediate immunized.) myelitis is needed, OPV
protection is needed, is recommended. OPV
OPV is recommended. should not be given to
immunocompromised indi-
viduals or to persons
with known or possibly
immunocompromised
family members. @ eIPV is
recommended in such
situations.
INACTIVATED-VIRUS VACCINES
Hepatitis B (HB) Two doses IM 4 weeks Adults at increased Data are not available on The vaccine produces neither
inactivated-virus apart; third dose 5 risk of occupational, the safety of the vaccine therapeutic nor adverse effects
vaccine months after second; environmental, social, for the developing fetus. on HBV-infected persons.
booster doses not or family exposure. Because the vaccine Prevaccination serologic
necessary within 7 contains only noninfectious screening for susceptibility
years of primary series. HBsAg particles, the risk before vaccination may or
Alternate schedule should be negligible. may not be cost effective
for one vaccine: three Pregnancy should not depending on costs of
doses IM 4 weeks apart; be considered a vaccine vaccination and testing and
fourth dose 10 months contraindication if the on the prevalence of immune
after the third. woman is otherwise persons in the group.
eligible.
Influenza vaccine Annual vaccination with Adults with high-risk History of anaphylactic No evidence exists of maternal
(inactivated current vaccine. Either conditions, residents of hypersensitivity to egg or fetal risk when vaccine is
whole-virus and whole- or split-virus nursing homes or other ingestion. administered in pregnancy
split-virus) vaccine may be used. chronic-care facilities, because of an underlying
vaccine medical-care personnel, high-risk condition in a preg-
or healthy persons nant woman. However, it is
>=65 years. reasonable to wait until the
second or third trimester, if
possible, before vaccination.
Human diploid Preexposure prophylaxis: Veterinarians, animal If there is substantial Complete preexposure
cell rabies two doses 1 week apart; handlers, certain risk of exposure to rabies, prophylaxis does not eliminate
vaccine (HDCV) third dose 3 weeks laboratory workers, preexposure vaccination the need for additional
inactivated, after second. If and persons living in may be indicated during therapy with rabies vaccine
whole-virion); exposure continues, or visiting countries pregnancy. Corticosteroids after a rabies exposure.
rabies vaccine, booster doses every 2 for >1 month where and immunosuppressive
adsorbed (RVA) years, or an antibody rabies is a constant agents can interfere with The decision for postexposure
titer determined and a threat. the development of active use of HDCV depends on the
booster dose administered immunity; history of species of biting animal, the
if titer is inadequate (<5). anaphylactic or Type III circumstances of biting
hypersensitivity reaction incident, and the type of expo-
Postexposure prophylaxis: to previous dose of HDCV. sure (e.g., bite, saliva contami-
All postexposure treat- (See text.) nation of wound). The type of
ment should begin and schedule for postexposure
with soap and water. prophylaxis depends upon
the person's previous rabies
1) Persons who have vaccination status, or the
a) previously received result of a previous or
postexposure prophylaxis current serologic test for
with HDCV, b) received rabies antibody. For
recommended IM pre- postexposure prophylaxis,
exposure series of HDCV, HDCV should always be
c) received recommended administered IM, not ID.
ID preexposure series of
HDCV in the United States,
or d) have a previously
documented rabies anti-
body titer considered
adequate: two doses of
HDCV, 1.0 mL IM, one
each on days 0 and 3.
2) Persons not previously
immunized as above:
HRIG 20 IU/kg body
weight, half infiltrated at
bite site if possible;
remainder IM; and five
doses of HDCV, 1.0 mL IM
one each on days 0, 3,
7, 14, 28.
INACTIVATED
BACTERIA
VACCINES
Cholera vaccine Two 0.5-mL doses SC or Travelers to countries No specific information on One dose generally satisfies
IM or two 0.2-mL doses requiring evidence of vaccine safety during International Health Regula-
ID 1 week to 1 month cholera vaccination for pregnancy. Use in preg- tions. Some countries may
apart; booster doses entry. nancy should reflect actual require evidence of a complete
(0.5 mL IM or 0.2 mL ID) increased risk. Persons primary series or a booster
every 6 months. who have had severe local dose given within 6 months
or systemic reactions to a before arrival. Vaccination
previous dose. should not be considered an
alternative to continued care-
ful selection of foods and
water.
Haemophilus Dosage for adults has May be considered for No specific information on No efficacy data available
influenzae type b not been determined. adults at highest theo- vaccine safety during for adults; not indicated for
conjugate vaccine retical risk (e.g., those pregnancy. adult contacts of children
(HbCV) with anatomic or func- with invasive disease.
tional asplenia or HIV
infection).
Meningococcal One dose in volume and Travelers visiting Pregnancy unless there is
polysaccharide by route specified areas of a country substantial risk of
vaccine by manufacturer; need that are recognized of infection.
(tetravalent for boosters unknown. as having epidemic
A, C, W135, meningococcal disease.
and Y)
Plague vaccine Three IM doses; first Selected travelers to Pregnancy, unless there is Prophylactic antibiotics may
dose 1.0 mL; second countries reporting substantial and unavoid- be recommended for definite
dose 0.2 mL 1 month cases, or in which able risk of exposure; per- exposure whether or not the
later; third dose avoidance of rodents sons with known hyper- exposed person has been
0.2 mL 5 months after and fleas is impossible; sensitivity to any of the vaccinated.
second; booster doses all laboratory and field vaccine constituents (see
(0.2 mL) at 1- to 2- personnel working with manufacturer's label);
year intervals if Yersinia pestis organ- patients who have had
exposure continues. isms possibly resistant severe local or systemic
to antimicrobials; those reactions to a previous
engaged in Y. pestis dose.
aerosol experiments or
in field operations in
areas with enzootic
plague where regular
exposure to potentially
infected wild rodents,
rabbits, or their fleas
cannot be prevented.
Pneumococcal One dose; revaccination Adults who are at The safety of vaccine for
polysaccharide recommended for those increased risk of pregnant women has not
vaccine (23 at highest risk >=6 years pneumococcal disease been evaluated; it should
valent). after the first dose. and its complications not be given during
because of underlying pregnancy unless the risk
health conditions; older of infection is high.
adults, especially those Previous recipients of
>=65 years of age who any type of pneumococcal
are healthy. polysaccharide vaccine
who are at highest risk of
fatal infection or antibody
loss may be revaccinated
>=6 years after the first
dose. (See text.)
INACTIVATED
BACTERIA AND
LIVE-BACTERIA
VACCINES
Typhoid vaccine, Two 0.5-mL doses SC Travelers to areas Severe local or systemic Vaccination should not be
SC and oral 4 or more weeks apart, where there is a reaction to a previous considered an alternative
booster 0.5 mL SC or recognized risk of dose. Acetone-killed and to continued careful selection
0.1 mL ID every 3 years exposure to typhoid. -dried vaccines should not of foods and water.
if exposure continues. be administered ID.
Four oral doses on
alternate days.
The manufacturer
recommends
revaccination with the
entire four-dose series
every 5 years.
LIVE-BACTERIA
VACCINE
Bacille Calmette- One dose ID or For children only, who Pregnancy, unless there is In the United States,
Guerin vaccine percutaneously. have prolonged close unavoidable exposure to tuberculosis-control
(BCG) (See package label.) contact with untreated infective tuberculosis; efforts are directed
or ineffectively treated immunocompromised towards early identifi-
active tuberculosis patients. @ cation and treatment
patients; groups with of cases, and preventive
excessive rates of new therapy with isoniazid.
infection in which other
control measures have
not been successful.
IMMUNE GLOBULINS
Cytomegalovirus Bone marrow transplant As prophylaxis for Prophylaxis must be contin-
immune globulin recipients: 1.0 g/kg bone marrow and ued for 3-4 months to be
(intravenous) weekly; kidney kidney transplant effective.
transplant recipients: recipients.
150 mg/kg initially,
then 50-100 mg/kg
every 2 weeks.
Immune globulin Hepatitis A prophylaxis: Nonimmune persons For travelers, IG is not an
(IG) Preexposure: one IM dose traveling to developing alternative to continued
of 0.02 mL/kg for antici- countries. careful selection of foods
pated risk of 2-3 months; and water. Frequent
IM dose of 0.06 mL/kg travelers should be tested
for anticipated risk of for hepatitis A antibody.
5 months; repeat IG is not indicated for
appropriate dose at persons with antibody to
above intervals if hepatitis A.
exposure continues.
Postexposure: one IM Household and sexual
dose of 0.02 mL/kg contacts of persons with
administered within hepatitis A; staff, attend-
2 weeks of exposure. ees, and parents of
diapered attendees in
day care center
outbreaks.
Measles prophylaxis: Exposed susceptible IG should not be used IG administered within
0.25 mL/kg IM (maximum contacts of measles to control measles. 6 days after exposure
15 mL) administered cases. can prevent or modify
within 6 days after measles. Recipients
exposure. of IG for measles
prophylaxis should
receive live measles
vaccine 3 months later.
Hepatitis B 0.06 mL/kg IM as soon Following percutaneous
immune as possible after or mucous-membrane
globulin exposure (with HB exposure to blood known
(HBIG) vaccine started at a to be HBsAg positive
different site); a second (within 7 days); following
dose of HBIG should be sexual exposure to a
administered 1 month person with acute HBV
later (percutaneous/ or an HBV carrier
mucous-membrane (within 14 days).
exposure) or 3 months
later (sexual exposure)
if the HB vaccine
series has not been
started. (See text.)
Tetanus immune 250 U IM. Part of management of
globulin (TIG) nonclean, nonminor
wound in a person with
unknown tetanus toxoid
status, with less than
two previous doses
or with two previous
doses and a wound
more than 24 hours old.
Rabies immune 20 IU/kg, up to half Part of management of Although preferable to
globulin, human infiltrated around rabies exposure in administer with the
(HRIG) wound; remainder IM. persons lacking a history first dose of vaccine, can
of recommended pre- be administered up to
exposure or postexpo- the eighth day after the
sure prophylaxis with first dose of vaccine.
HDCV.
Vaccinia immune 0.6 mL/kg in divided Treatment of eczema Of no benefit for
globulin doses over 24-36 hours; vaccinatum, vaccinia postvaccination
may be repeated every necrosum, and ocular encephalitis.
2-3 days until no new vaccinia.
lesions appear.
Varicella-zoster Persons >50 kg: Immunocompromised
immune globulin 125 U/10 kg IM; patients known or likely
(VZIG) persons >50 kg: to be susceptible with
625 U **. close and prolonged
exposure to a household
contact case or to an
infectious hospital staff
member or hospital
roommate.
---------------------------------------------------------------------------------------------------------------------------------------------------
* Refer also to sections of text on specific vaccines or toxoids for further details on indications, contraindications, precautions, dosages, side
effects and adverse reactions, and special considerations. Refer also to individual ACIP statements (see list of published ACIP statements,
Appendix 2). Several other vaccines, toxoids, and immune globulins are licensed and available. These are noted in Appendix 3. In addition,
the following antitoxins are licensed and available: a) botulism antitoxin, trivalent equine (ABE) (distributed by CDC only), and b) tetanus
antitoxin (equine).
+ Several vaccines and toxoids are in "Investigational New Drug" (IND) status and available only through the U.S. Army Research Institute for
Infectious Diseases (telephone 301-663-2403). These are: a) eastern equine encephalitis vaccine (EEE), b) western equine encephalitis vaccine
(WEE), c) Venezuelan equine encephalitis vaccine (VEE), and d) tularemia vaccine. Pentavalent (ABCDE) botulinum toxoid is available only
through CDC's Drug Service.
& When any vaccine or toxoid is indicated during pregnancy, waiting until the second or the third trimester, when possible, is a reasonable
precaution that minimizes concern about teratogenicity.
@ Persons immunocompromised because of immune deficiency diseases, HIV infection (who should primarily not receive OPV and yellow
fever vaccines) (see text), leukemia, lymphoma, or generalized malignancy or immunosuppressed as a result of therapy with corticosteroids,
alkylating drugs, antimetabolites, or radiation.
** Some persons have recommended 125 U/10 kg regardless of total body weight.
=====================================================================================================================================================
Return to top. Table_8 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 8. Summary guide to tetanus prophylaxis * in routine wound management,
United States
========================================================================================================
Clean, minor wounds All other wounds +
------------------- ------------------
Td & TIG @ Td & TIG
------------------------------------------------------------------------
Uncertain or <3 Yes No Yes Yes
>3 ** No ++ No No && No
------------------------------------------------------------------------
* Refer also to text on specific vaccines or toxoids for contraindications, precautions, dosages,
side effects, adverse reactions, and special considerations. Important details are in the text and
in the ACIP recommendations on diphtheria, tetanus, and pertussis (DTP) (MMWR 1991:
40{RR-10)).
+ Such as, but not limited to: wounds contaminated with dirt, feces, and saliva; puncture
wounds; avulsions; and wounds resulting from missiles, crushing, burns, and frostbite.
& Td = Tetanus and diphtheria toxoids, adsorbed (for adult use). For children <7 years old, DTP
(DT, if pertussis vaccine is contraindicated) is preferred to tetanus toxoid alone. For persons >=7
years old, Td is preferred to tetanus toxoid alone.
@ TIG = Tetanus immune globulin.
** If only three doses of fluid toxoid have been received, a fourth dose of toxoid, preferably an
adsorbed toxoid, should be given.
++ Yes, >10 years since last dose.
&& Yes, >5 years since last dose. (More frequent boosters are not needed and can accentuate side
effects.)
========================================================================================================
Return to top. Table_9 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 9. Recommendations for postexposure prophylaxis for percutaneous or
permucosal exposure to hepatitis B, United States
=================================================================================================
Treatment when source is:
------------------------------------------------------------------------------
Source not tested
Exposed person HBsAg * positive HBsAg negative or unknown
-----------------------------------------------------------------------------------------------
Unvaccinated HBIG + x 1 & and Initiate HB Initiate HB vaccine **
initiate HB @ vaccine ** vaccine **
Previously Test exposed for No treatment No treatment
vaccinated anti-HBs ++
Known 1. If adequate, &&
responder no treatment
2. If inadequate,
HB vaccine
booster dose
Known HBIG x 2 or No treatment If known high-risk source,
nonresponder HBIG x 1 plus 1 may treat as if source were
HB vaccine HBsAg positive
Response Test exposed for No treatment Test exposed for anti-HBs
unknown anti-HBs 1. If inadequate, &&
1. If inadequate, && HB vaccine booster dose
HBIG x 1 plus HB 2. If adequate, no treatment
vaccine booster dose
2. If adequate, no treatment
-----------------------------------------------------------------------------------------------
* HBsAg = Hepatitis B surface antigen.
+ HBIG = Hepatitis B immune globulin.
& HBIG dose 0.06 mL/kg IM.
@ HB = Hepatitis B.
** For HB vaccine dose, see reference 21.
++ Antibody to hepatitis B surface antigen.
&& Adequate anti-HBs is 10 SRU by radioimmunoassay or positive by enzyme immunoassay.
=================================================================================================
Return to top. Table_10 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 10. Recommendations for postexposure prophylaxis for perinatal and sexual
exposure to hepatitis B, United States
==============================================================================================
HBIG * Vaccine
------------------------------------ -------------------------------
Recommended Recommended
Exposure Dose timing Dose timing
--------------------------------------------------------------------------------------
Perinatal 0.5 mL IM + Within 12 hours 0.5 mL IM +& Within 12 hours
of birth of birth @
Sexual 0.06 mL/kg IM + Single dose within 1.0 mL IM +& First dose at
14 days of last time of HBIG *
sexual contact treatment @
--------------------------------------------------------------------------------------
* HBIG = Hepatitis B immunoglobulin.
+ IM = intramuscularly
& For appropriate age-specific doses of each vaccine, see reference 21.
@ The first dose can be administered the same time as the HBIG dose but at a different site;
subsequent doses should be administered as recommended for specific vaccine.
==============================================================================================
Return to top. Figure_1 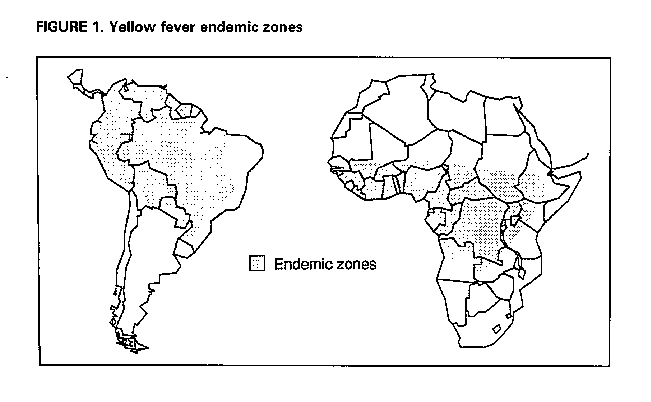 Return to top. Table_A1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
Appendix 1
Published ACIP Statements* Related to Specific Diseases and Immunobiologics
Recommendations, as of September 1, 1991
====================================================================================================
Subject MMWR Publication
---------------------------------------------------------------------------------
General recommendations 1989;38:205-14,
on immunizations 219-27
Erratum: 1989;38:311
Bacille Calmette-Guerin 1988;37:663-4
669-75
Cholera 1988;37:617-24
Diphtheria, tetanus, and pertussis 1991;40(No. RR-10):1-28
Haemophilus influenzae type b conjugate 1991;40(no. RR-1):1-7
Hepatitis, viral 1990;39(No. RR-2):1-26
Human T-lymphotropic virus type III/ 1986;35:595-8,
lymphadenopathy-associated virus, 603-6
immunization of children with
Human immunodeficiency virus, immunization of 1988;37:181-6
children with (supplementary statement)
Influenza+ 1991;40(No. RR-6):1-15
Measles 1989;38:(No. S-9):1-18
Meningococcal polysaccharide 1985;34:255-9
Mumps 1989;38:388-92,
397-400
Plague 1982;31:301-4
Pneumococcal polysaccharide 1989;38:64-8,73-6
Poliomyelitis 1982;31:22-6,31-4
Poliomyelitis, enhanced potency inactivated vaccine 1987;36:795-8
Rabies 1991;40(No. RR-3):1-19
Rubella 1990;39(No. RR-15):1-18
Smallpox (Vaccinia) 1985;34:341-2
Typhoid 1990;39(No. RR-10):1-5
Yellow fever 1990;39(No. RR-6):1-6
Varicella-zoster (chickenpox) immune globulin 1984;33:84-90,95-100
---------------------------------------------------------------------------------
* The Immunization Practices Advisory Committee (ACIP) periodically reviews recommendations
on vaccination and prophylaxis. When recommendations are revised, they are published
individually in the MMWR.
+ Each year influenza vaccine recommendations are reviewed and amended to reflect updated
information on influenza activity in the United States for the preceding influenza season and to
provide information on the vaccine available for the upcoming influenza season. These
recommendations are published in the MMWR annually, usually in May or June.
====================================================================================================
Return to top. Table_A2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
Appendix 2
National Coalition for Adult Immunization
Member Organizations
(as of March 1, 1991)
American Academy of Family Physicians Food and Drug Administration
American Academy of Otolaryngology- Gray Panthers
Head and Neck Surgery Harvard Community Health Plan
American Academy of Pediatrics Health Insurance Association of America
American Academy of Physician Assistants Infectious Diseases Society of America
American Association of Medical Colleges Lederle-Praxis Biologicals, A Cyanamid
American Association for World Health Business Unit
American Association of Retired Persons March of Dimes Birth Defects Foundation
American College of Obstetricians and Merck Sharp & Dohme
Gynecologists National AIDS Network
American College Health Association National Association of City and County
American College of Physicians Health Officials
American College of Preventive Medicine National Association of Hispanic Elderly
American Council of Life Insurance National Council of Community Hospitals
American Dental Association National Council for Education of Health
American Geriatrics Society Professionals-Health Promotion
American Group Practice Association National Council of Senior Citizens
American Hepatitis Association National Foundation for Infectious Diseases
American Hospital Association National Health Council
American Indian Health Care Association National Institute of Allergy and Infectious
American Liver Foundation Diseases, National Institutes of Health
American Lung Association National Leadership Coalition of AIDS
American Medical Association Parke-Davis Division of Warner-Lambert
American Managed Care and Review Company
Association Pharmaceutical Manufacturers Association
American Medical Student Association Phi Delta Chi Pharmacy Fraternity
American Nurses' Association Program for Appropriate Technology in Health
American Podiatric Medical Association Retirement Advisors
American Public Health Association Roche Laboratories, A Division of
American Social Health Association Hoffmann-La Roche, Inc.
American Society for Microbiology Sclavo, Inc.
American Society of Hospital Pharmacists Saint Louis Department of Health and
American Society of Internal Medicine Hospitals
American Thoracic Society Service Employees International Union,
Association of American Medical Colleges AFL-CIO, CLC
Association of Practitioners in Infection SmithKline Beecham Pharmaceuticals
Control Society of General Internal Medicine
Association of State and Territorial Health Society of Hospital Epidemiologists of
Officials America
Association of Teachers of Preventive E.R. Squibb and Sons, Inc.
Medicine State of Washington Division of Health
Catholic Health Association The Surgeon General, U.S. Public Health
Centers for Disease Control Service
Conference of State and Territorial U.S. Conference of Local Health Officers
Epidemiologists U.S. Department of Defense
Connaught Laboratories, Inc., A United States Pharmacopeial Convention
Pasteur Merieux Company Veterans Administration Medical Center,
Du Pont Pharmaceuticals Minneapolis
Federation of American Health Systems Wyeth-Ayerst Laboratories
Return to top. Table_A3 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
Appendix 3
Suggested Immunization Record Form for Health-Care Provider
=================================================================================
Name ___________________________________ Sex ______ Birth Date ______________
Vaccine Date given Vaccine Doctor or Date next
Vaccine type Mo/Day/Yr lot # clinic dose due
-------------------------------------------------------------------------------
Polio __________ __________ __________ __________ __________
(OPV or eIPV)* __________ __________ __________ __________ __________
__________ __________ __________ __________ __________
Diphtheria __________ __________ __________ __________ __________
Tetanus __________ __________ __________ __________ __________
Pertussis __________ __________ __________ __________ __________
(DTP or DT, __________ __________ __________ __________ __________
Pediatrc or __________ __________ __________ __________ __________
Td {Adult})*
Measles __________ __________ __________ __________ __________
Mumps, __________ __________ __________ __________ __________
Rubella, or __________ __________ __________ __________ __________
Combinations* __________ __________ __________ __________ __________
Influenza __________ __________ __________ __________ __________
__________ __________ __________ __________ __________
__________ __________ __________ __________ __________
__________ __________ __________ __________ __________
Pneumococcal __________ __________ __________ __________ __________
Polysaccharide
Hepatitis B __________ __________ __________ __________ __________
__________ __________ __________ __________ __________
__________ __________ __________ __________ __________
Other vaccines __________ __________ __________ __________ __________
or Immune __________ __________ __________ __________ __________
Globulins* __________ __________ __________ __________ __________
Tuberculin __________ __________ __________ __________ __________
Test
Notes:
-------------------------------------------------------------------------------
* Specify type used.
=================================================================================
Return to top. Table_A4 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
Appendix 4
Immunobiologics Available, as of March 1, 1991,
by Product Name and Manufacturer, with
Manufacturers' Addresses and Telephone Numbers *
====================================================================================================
Immunobiologic Manufacturer Product name
------------------------------------------------------------------------------------
Adenovirus vaccine Wyeth-Ayerst Labs, Inc. Adenovirus, Live, Oral, Type 4 +
Adenovirus, Live, Oral, Type 7 +
Anthrax vaccine Michigan Department Anthrax Vaccine, Absorbed &
of Public Health
BCG vaccine Organon Teknika BCG Vaccine
Corporation
Cholera vaccine Wyeth-Ayerst Labs, Inc. Cholera Vaccine
Cytomegalovirus Massachusetts Public Cytomegalovirus Immune
immune gIobulin Health Biologic Labs Globulin, Intravenous
Diphtheria and Connaught Labs, Inc. Diphtheria and Tetanus Toxoids,
tetanus toxoids, Adsorbed (Pediatric)
adsorbed
Lederle Laboratories, Diphtheria and Tetanus Toxoids,
Division of American Adsorbed (Purogenated for
Cyanamid Co. Pediatric Use)
Massachusetts Public Diphtheria and Tetanus Toxoids,
Health Biologic Labs Adsorbed (Pediatric)
Michigan Department Diphtheria and Tetanus Toxoids,
of Public Health Adsorbed (Pediatric) &
Sclavo SpA @ Diphtheria and Tetanus Toxoids,
Adsorbed, USP (Pediatric)
Wyeth-Ayerst Labs, Inc. Diphtheria and Tetanus Toxoids,
Adsorbed (For Pediatric Use)
Diphtheria and Connaught Labs, Inc. Diphtheria and Tetanus Toxoids,
tetanus toxoids and and Pertussis Vaccine, Adsorbed
pertussis vaccine,
adsorbed
Lederle Laboratories, Diphtheria and Tetanus Toxoids
Division of American and Pertussis Vaccine, Adsorbed
Cyanamid Co. (Tri Immunol)
Massachusetts Public Diphtheria and Tetanus Toxoids
Health Biologic Labs and Pertussis Vaccine, Adsorbed
Michigan Department Diphtheria and Tetanus Toxoids
of Public Health and Pertussis Vaccine, Adsorbed &
Haemophilus Connaught Labs, Inc. ProHIBit
influenzae type b
vaccine
(polysaccharide-
conjugate)
Lederle-Praxis HibTITER
Biologicals
Merck Sharp & Dohme, Pedvax-Hib
Division of Merck
& Co., Inc.
Hepatitis B Immune Merck Sharp & Dohme, Hepatitis B Immune GIobulin
globulin Division of Merck (Human) (MSD,
& Co., Inc. HEP-B-GAMMAGEE)
Cutter Biological, Hepatitis B Immune Globulin
Division of Miles, Inc. (HYPER-HEP)
Abbott Laboratories Hepatitis B Immune Globulin
(Human) (H-BIG)
Hepatitis B vaccine Merck Sharp & Dohme, Recombivax HB
(recombinant) Division of Merck
& Co., Inc.
SmithKline Beecham Engerix B
Immune globulin Armour Pharmaceutical Immune Serum Globulin
Company (Human) (GAMMAR;
GAMMAR-IV)
Central Laboratory Immune Globulin Intravenous
Blood Transfusion (SANDOGLOBULIN)
Service, Swiss
Red Cross
Cutter Biological, Immune Globulin Intravenous
Division of Miles, Inc. {5% in 10% Maltose
(GAMIMUNE)}
Immune Globulin (Human), USP
(GAMASTAN)
Hyland Division Immune Globulin Intravenous
Baxter Healthcare Corp. (Human); (GAMMAGARD)
Massachusetts Public Immune Serum Globulin
Health Biologic Labs (Human)
Michigan Department Immune Serum Globulin
of Public Health (Human) &
New York Blood Ctr, Immune Serum Globulin
Inc. (Human)
Influenza vaccine Connaught Labs, Inc. Influenza Virus Vaccine
(Zonal Purified) Whole Virion
(FLUZONE)
Connaught Labs, Inc. Influenza Virus Vaccine
(Zonal Purified) Split Virion
(FLUZONE)
Lederle Laboratories, Influenza Virus Vaccine
Division of American (Split Virion {FLUIMUNE})
Cyanamid Co
Parke-Davis, Division Influenza Virus Vaccine
of Warner-Lambert Co. (Split Virion {FLUOGEN})
Wyeth-Ayerst Labs, Inc. Influenza Virus Vaccine,
Subvirion Type
Measles, mumps, and Merck Sharp & Dohme, Measles, Mumps, and Rubella
rubella vaccine Division of Merck Virus Vaccine, Live
Co., Inc. (MSD, MMR II)
Measles and rubella Merck Sharp & Dohme, Measles and Rubella Virus
vaccine Division of Merck Vaccine, Live
& Co., Inc. (MSD, M-R-VAX II)
Measles vaccine Merck Sharp & Dohme, Measles Virus Vaccine, Live
Division of Merck (Attenuated {MSD}
& Co., Inc. ATTENUVAX)
Meningococcal Connaught Labs, Inc. Meningococcal
polysaccharide Polysaccharide Vaccine
vaccine (MENOMUNE-A/C/Y/W-135)
A,C,Y, and W 135
Mumps vaccine Merck Sharp & Dohme, Mumps Virus Vaccine, Live
Division of Merck (MSD, MUMPSVAX)
& Co., Inc.
Pertussis vaccine, Michigan Department Pertussis Vaccine, Adsorbed
adsorbed of Public Health
Plague vaccine Cutter Biological, Plague Vaccine
Division of Miles, Inc.
Pneumococcal Lederle Laboratories, Pneumococcal Vaccine,
polysaccharide Division of American Polyvalent (PNU-IMUNE 23)
vaccine Cyanamid Co.
Merck Sharp & Dohme Pneumococcal Vaccine,
Division of Merck Polyvalent (MSD,
& Co., Inc. PNEUMOVAX 23)
Poliovirus vaccine Connaught Labs, Inc. Poliovax
inactivated
Poliovirus vaccine, Lederle Laboratories, Poliovirus Vaccine, Live, Oral
live, oral Division of American Trivalent (ORIMUNE)
Cyanamid Co.
Rabies immune Cutter Biological, Rabies Immune Globulin
globulin Division of Miles, Inc. (Human) (HYPERAB)
Institut Merieux ** Rabies Immune Globulin
(Human) (IMOGAMRABIES)
Rabies vaccine Institut Merieux ** Rabies Vaccine
(Human Diploid Cell
{IMOVAX-RABIES},
{IMOVAX-RABIES ID})
Rabies vaccine Michigan Department Rabies Vaccine, Adsorbed &
of Public Health
Rubella vaccine Merck Sharp & Dohme, Rubella Virus Vaccine, Live
Division of Merck (MSD, MERUVAX II)
& Co., Inc.
Rubella and mumps Merck Sharp & Dohme, Rubella and Mumps Virus
vaccine Division of Merck Vaccine, Live
& Co., Inc. (MSD, BIAVAX II)
Tetanus antitoxin Sclavo, SpA @ Tetanus Antitoxin
Purified, USP
Tetanus immune Cutter Biological, Tetanus Immune Globulin
globulin Division of Miles, Inc. (Human) (HYPER-TET)
Massachusetts Public Tetanus Immune Globulin
Health Biologic Labs (Human)
Tetanus and Connaught Labs, Inc. Tetanus and Diphtheria Toxoids,
diphtheria toxoids, Adsorbed (For Adult Use)
adsorbed
Lederle Laboratories, Tetanus and Diphtheria Toxoids,
Division of American Adsorbed (For Adult Use)
Cyanamid Co. (Purogenated Parenteral)
Massachusetts Public Tetanus and Diphtheria Toxoids,
Health Biologic Labs Adsorbed (For Adult Use)
Sclavo SpA @ Tetanus and Diphtheria Toxoids,
Adsorbed, USP (Adult)
Wyeth-Ayerst Labs, Inc. Tetanus and Diphtheria Toxoids,
Adsorbed (For Adult Use)
(Aluminum Phosphate,
Ultrafined)
Tetanus toxoid, Connaught Labs, Inc. Tetanus Toxoid, Adsorbed
adsorbed
Lederle Laboratories, Tetanus Toxoid, Adsorbed
Division of American (Purogenated {Aluminum
Cyanamid Co. Phosphate Adsorbed})
Massachusetts Public Tetanus Toxoid, Adsorbed
Health Biologic Labs
Michigan Department Tetanus Toxoid, Adsorbed &
of Public Health
Sclavo SpA @ Tetanus Toxoid, Adsorbed,
USP
Wyeth-Ayerst Labs, Inc. Tetanus Toxoid, Adsorbed
(Aluminum Phosphate
Adsorbed, Ultrafined)
Tetanus toxoid, Connaught Labs, Inc. Tetanus Toxoid (Fluid)
fluid
Lederle Laboratories, Tetanus Toxoid
Division of American (Purogenated, Tetanus
Cyanamid Co. Toxoid Fluid)
Sclavo SpA @ Tetanus Toxoid (Fluid)
Wyeth-Ayerst Labs, Inc. Tetanus Toxoid
(Fluid, Purified, Ultrafined)
Typhoid vaccine Wyeth-Ayerst Labs, Inc. Typhoid Vaccine, U.S.P.
Wyeth-Ayerst Labs, Inc. Typhoid Vaccine +
(Acetone-killed and -dried)
Typhoid vaccine, Swiss Serum and Vivotif Berna
live, oral/Ty21A and Vaccine Institute
Vaccinia immune None (CDC and Vaccinia Immune GIobulin
globulin Department of Defense (Human)
stockpiles only)
Vaccinia vaccine None (CDC stockpiles Smallpox Vaccine
only)
Varicella-zoster Massachusetts Public Varicella-Zoster Immune
immune globulin Health Biologic Labs Globulin (Human) ++
Yellow fever vaccine Connaught Labs, Inc. Yellow Fever Vaccine
(Live, 17D Virus, YF-VAX)
------------------------------------------------------------------------------------
* In the preparation of this appendix, every effort was made to assure its completeness and
accuracy. This appendix was compiled from information obtained from manufacturers, the
Division of Product Certification, Food and Drug Administration, and the Physicians' Desk
Reference, 44th Edition, 1991, and, to the best of our knowledge, is an accurate and complete
listing as of March 1, 1991. However, omissions and errors may have occurred inadvertently.
This appendix is intended to be a resource and does not replace the provider's obligation to
remain otherwise current on the availability of vaccines, toxoids, and immune globulins.
+ Available only to the U.S. Armed Forces.
& Outside Michigan, sold only to providers who will sign a "hold harmless" agreement.
@ Sclavo SpA products distributed in United States by Sclavo, Inc.
** Institut Merieux products distributed by Connaught Labs, Inc.
++ VariceIIa-zoster immune globulin is available from selected blood banks in various locations in
the United States. Consult Appendix 6 for a listing.
====================================================================================================
Immunobiologics
Manufacturers/Distributors
========================================================================
Manufacturer/Distributor Telephone
----------------------------------------------------------------------
1. Abbott Laboratories (708) 937-6100 or
Abbott Park, IL 60064 (800) 323-9100, x131
2. Armour Pharmaceutical Company (815) 932-6771 or
Kankakee, IL 60901 (800) 435-1852
3. Connaught Laboratories, Inc. (717) 839-7189 or
Swiftwater, PA 19370 (800) 822-2463
4. Cutter Biological (415) 420-5177
Division of Miles Laboratories, Inc. (800) 288-8371
Berkeley, CA 94701
5. Hyland Division (800) 423-2090
Baxter Healthcare Corporation
Glendale, CA 91202
6. Lederle Laboratories (914) 732-5000
Division of American Cyanamid Co. (201) 831-2000
Pearl River, NY 10965 (800) 533-3753
Wayne, NJ 07470
7. Lederle-Praxis Biologicals (800) 526-7870
30 Corporate Woods
Suite 300
Rochester, NY 14623
8. Massachusetts Public Health (617) 522-3700
Biologic Laboratories
Boston, MA 02130
9. Merck Sharp & Dohme (215) 661-5000
Division of Merck & Co., Inc.
West Point, PA 19486
10. Merieux Institute, Inc. (305) 593-9577 or
Miami, FL 33169 (800) 327-2842
11. Michigan Department of Public Health (517) 335-8119
Lansing, MI 48909
12. New York Blood Center (212) 570-3000
Blood Derivatives (800) 487-8751
New York, NY 10021
13. Organon Teknika Corporation (800) 323-6442
5516 Nicholson Lane
Kensington, MD 20895
14. Parke-Davis (201) 540-2000
Division of Warner-Lambert Co.
Morris Plains, NJ 07950
15. Sclavo, Inc. (201) 696-8300 or
Wayne, NJ 07470 (800) 526-5260
16. Swiss Serum and Vaccine Institute (305) 443-2900
Berna Products
Coral Gables, FL
17. SmithKline Beecham (215) 751-4912
Philadelphia, PA 19101
18. Wyeth-Ayerst Laboratories, Inc. (215) 688-4400 or
Philadelphia, PA 19101 (800) 321-2304
---------------------------------------------------------------------
=======================================================================
Return to top. Table_A5 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
Appendix 5
Use of Immunobiologics in Pregnancy *
==============================================================================================================================================
Risk from Risk from Risk from Indications
disease to disease to Type of immunizing for immunization
Immunizing pregnant fetus of immunizing agent during Dose
agent female neonate agent to fetus pregnancy schedule Comments
--------------------------------------------------------------------------------------------------------------------------------------------
LIVE-VIRUS VACCINES
Measles Significant Significant Live, attenuated- None Contraindicated One or two doses, Vaccination of
morbidity, increase in virus vaccine confirmed (See immune depending on school/ susceptible
low mortality abortion rate; globulins) work status (see women should
(not altered may cause text) be part of post-
by pregnancy) malformation partum care
Mumps Low morbidity Probable Live, attenuated- None Contraindicated Single dose
and mortality increased rate virus vaccine confirmed
(not altered of abortion in
by pregnancy) first trimester.
Questionable
association of
fibroelastosis
in neonates
Rubella Low morbidity High rate of Live, attenuated- None Contraindicated Single dose Teratogenicity
and mortality abortion and virus vaccine confirmed of vaccine is
(not altered congenital theoretical, not
by pregnancy) rubella confirmed to
syndrome date; vaccination
of susceptible
women should be
part of post-
partum care
Yellow fever Significant Unknown Live, attenuated- Unknown Contraindicated Single dose Postponement of
morbidity and virus vaccine except if expo- travel preferable
mortality sure risk is high to vaccination, if
(not altered possible
by pregnancy,
TOXOIDS
Tetanus- Severe Neonatal Combined None Lack of primary Primary: two doses Updating of
Diphtheria morbidity; tetanus tetanus- confirmed series or no at 1- to 2-month immune status
tetanus mortality, diphtheria booster within interval with a should be part of
mortality, 60% toxoids past 10 years third dose 6-12 antepartum care;
60%; diph- preferred; months after the unvaccinated
theria mor- adult tetanus- second. Booster: women should be
tality, 10% diphtheria single dose every vaccinated,
(both of formulation 10 years after preferably after
which are completion of the first trimester
not altered primary series
by pregnancy)
INACTIVATED-VIRUS AND
LIVE-VIRUS VACCINES
Poliomyelitis No increased Anoxic fetal Live, attenuated- None Not routinely Primary: two doses OPV indicated
incidence in damage virus (OPV) and confirmed recommended of eIPV 4-8 weeks for susceptible
pregnancy but reported; inactivated virus for adults in apart and a third pregnant women
may be more 50% mortality (eIPV) vaccine United States, dose 6-12 months traveling in
severe if it in neonatal except persons after the second endemic areas
does occur disease at increased risk dose; two doses of or in other high-
of exposure. OPV with a 6- to risk situations.
8-week interval No data on safety
and a third dose of eIPV in
at least 6 weeks pregnancy.
later, customarily
8-12 months later
INACTIVATED VIRUS VACCINES
Hepatitis B Possible Possible Inactivated None Indications for 1.0 mL Infants born to
increased increase in HB vaccine reported prophylaxis not intramuscularly HBsAg-positive
severity abortion rate altered by at 0, 1, and mothers should
during third and prema- pregnancy 6 months receive 0.5 mL
trimester turity; peri- HBIG as soon as
natal trans- possible after
mission may birth, plus 0.5
occur if mL HB vaccine
mother is a within 1 week of
chronic birth. Vaccine
carrier or is should be
acutely repeated at
infected 1 and 6
months
Influenza Possible Possible Inactivated None Usually Consult with Criteria for
increase increased type A and confirmed recommended public health vaccination of
in mortality abortion type B virus only for patients authorities pregnant women
during rate; no vaccines with serious because same as for all
epidemic of malformation underlying recommendations adults
new antigenic confirmed diseases; public change each year
strain health authori-
ties to be con-
sulted for current
recommendation
Rabies Near 100% Determined Killed-virus Unknown Indications for Public health
fatality by maternal vaccine prophylaxis not authorities to be
(not altered disease altered by consulted for
by pregnancy) pregnancy; each indications and
case considered dosage
individually
INACTIVATED-BACTERIA VACCINES
Cholera Significant Increased risk Killed-bacteria Unknown Only to meet Two injections, Vaccine of low
morbidity and of fetal death vaccine international 4-8 weeks apart efficacy
mortality; during travel
more severe maternal requirements
during third illness
trimester occurring
during
third
trimester
Menin- No increased Unknown Killed-bacteria No data Indications not Public health
gococcus risk during vaccine available altered by authorities to be
pregnancy; on use pregnancy; consulted
no increase during vaccination
in severity pregnancy recommended
of disease only in unusual
outbreak
situations
Plague Significant Determined Killed-bacteria None Very selective Public health
morbidity and by maternal vaccine reported vaccination of authorities to be
mortality disease exposed persons consulted for
(not altered indications and
by pregnancy) dosage
Pneumo- No increased Unknown Polyvalent No data Indications In adults one dose
coccus risk during polysaccharide available not altered only, unless they
pregnancy; vaccine on use by pregnancy; are at highest risk
no increase during vaccine used of fatal infection
in severity pregnancy only for persons or antibody loss;
of disease at high risk such persons may
be revaccinated >6
years after the first
dose (see text)
Typhoid Significant Unknown Killed-bacteria None Not recom- Killed primary: two
morbidity and vaccine; live, confirmed mended injections, 4 weeks
mortality attenuated- routinely except apart; booster:
(not altered bacteria for close, con- single dose every 3
by pregnancy) vaccine tinued expo- years; oral primary:
sure or travel to four doses on
areas where alternate days;
disease is booster: four doses
endemic every 5 years
IMMUNE GLOBULINS
Hepatitis A Possible Possible Pooled immune None Postexposure 0.02 mL/kg in one IG should be
increased increase in globulin (IG) reported prophylaxis dose of IG given as soon
severity abortion rate as possible and
during third and prematu- within 2 weeks of
trimester rity; possible exposure; infants
transmission born to mothers
to neonate at who are incuba-
delivery if ting the virus or
mother is are acutely ill at
incubating delivery should
the virus or is receive one dose
acutely ill at of 0.5 mL as soon
that time as possible
after birth
Hepatitis B Possible Possible Hepatitis B None Postexposure 0.06 mL/kg or 5 mL Infants born to
increased increase in immune reported prophylaxis immediately, plus HBsAg-positive
severity abortion rate globulin HB vaccine series, mothers should
during third and prema- (HBIG) when indicated receive 0.5 mL
trimester turity; peri- HBIG as soon as
natal trans- possible after
mission may birth, plus 0.5 mL
occur if HB vaccine with-
mother is a in 1 week of
chronic birth. Vaccine
carrier or is should be
acutely repeated at 1
infected; and 6 months
newborns
are at risk of
fulminant
hepatitis or
chronic
carriage
Measles Significant Significant Pooled immune None Postexposure 0.25 mL/kg in Unclear if IG
morbidity, increase in globulin (IG) reported prophylaxis one dose of IG, prevents
low abortion rate; up to 15 mL abortion; must
mortality may cause be given within 6
(not altered malformations days of exposure
by pregnancy)
Rabies Near 100% Determined Human rabies None Postexposure 20 IU/kg in one Used with rabies
fatality by maternal immune reported prophylaxis dose of HRIG killed-virus
(not altered disease globulin vaccine
by pregnancy) (HRIG)
Tetanus Severe Neonatal Tetanus None Postexposure 250 U in one dose Used with
morbidity; tetanus immune reported prophylaxis of TIG tetanus toxoid
mortality, mortality, globulin
60% 60% (TIG)
Varicella Possible Can cause Varicella-zoster None Not routinely One vial per Primarily indicat-
increase neonatal immune reported indicated in kilogram in one ed for newborns
in severe varicella with globulin healthy pregnant dose of VZIG, up of mothers who
varicella increased (VZIG) women exposed to five vials had varicella
pneumonia mortality in to varicella within five days
neonatal before delivery or
period; very 48 hours after de-
rarely causes livery. Approxi-
congenital mately 90%-95%
defects of adults are
immune to
varicella
--------------------------------------------------------------------------------------------------------------------------------------------
* Modified from American College of Obstetricians and Gynecologists (ACOG). Immunization during pregnancy ACOG Technical Bulletin
#64. Washington DC: ACOG, 1982. This appendix describes methods and techniques of clinical practice that are currently acceptable and
used by recognized authorities. However it does not represent official policy or recommendations of the American College of Obstetricians
and Gynecologists. Its publication should not be construed as excluding other acceptable methods of handling similar problems.
==============================================================================================================================================
Return to top. Table_A6 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
Appendix 6
Varicella-Zoster Immune Globulin
Regional Distribution Centers and Service Areas
=======================================================================
Regional center
Service areas and 24-hour telephone
---------------------------------------------------------------------
United States and territories
Alabama American Red Cross
Blood Services
Alabama region
(205) 322-5661
Alaska (see Oregon)
Arizona American Red Cross
Blood Services
Southern Arizona region
(602) 623-0541
Arkansas (see Missouri)
California, northern American Red Cross
Blood Services
Central California region
(408) 292-1626
California, southern American Red Cross
Blood Services
L.A.-Orange County region
(213) 739-5200
Colorado (see New Mexico)
Connecticut American Red Cross
Blood Services
Connecticut region
(203) 678-2730
Delaware (see Pennsylvania)
Florida South Florida
Blood Service
(305) 326-8888
American Red Cross
Blood Services
Mid-Florida region
(904) 255-5444
Georgia American Red Cross
Blood Services
Atlanta region
(404) 881-9800
(404) 881-6752 (night)
Hawaii (see California, southern)
Idaho American Red Cross
Blood Services
Snake River region
(208) 342-4500
Illinois, northern American Red Cross
Blood Services
Mid-America region
(312) 440-2222
Illinois, southern (see Missouri)
Indiana American Red Cross
Blood Services
Fort Wayne region
(219) 482-3781
Iowa (see Wisconsin, S.E.)
Kansas (see Missouri)
Kentucky (see Missouri)
Louisiana (see Texas {Gulf coast})
Maine American Red Cross
Blood Services
Northeast-Portland
(207) 775-2367
Maryland American Red Cross
Blood Services
(301) 764-4639
(also see Washington, DC)
Massachusetts Massachusetts Public
Health
United States Biologics
Laboratories
(617) 522-3700
Michigan American Red Cross
Blood Services
Southeastern Michigan
region
(313) 494-2715
American Red Cross
Blood Services
Wolverine region
(313) 232-1176
American Red Cross
Blood Services
Great Lakes region
(517) 484-7461
Minnesota American Red Cross
Blood Services
St. Paul region
(612) 291-6789
(612) 291-6767 (night)
Mississippi (see Alabama)
Missouri American Red Cross
Blood Services
(314) 658-2000
(314) 658-2136 (night)
Montana (see Oregon)
Nebraska American Red Cross
Blood Services
Midwest region
(402) 341-2723
Nevada (see California, northern)
New Hampshire (see Vermont)
New Jersey, northern (see Greater New York
Blood Program)
New Jersey, southern (see Pennsylvania)
New Mexico United Blood Services
(505) 247-9831
New York The Greater New York
Blood Program
(212) 468-2106
(212) 570-3068 (night)
American Red Cross
Blood Services
Northeastern New York
region
(518) 449-5020
(518) 462-7461
(518) 462-6964 (night)
American Red Cross
Blood Services
Greater Buffalo Chapter
(716) 886-6866
American Red Cross
Blood Services
Rochester region
(716) 461-9800
American Red Cross
Blood Services
Syracuse region
(315) 425-1647
North Carolina American Red Cross
Blood Services
Carolinas region
(704) 376-1661
North Dakota (see Wisconsin, S.E.)
Ohio American Red Cross
Blood Services
Northern Ohio region
(216) 781-1800
American Red Cross
Central Ohio region
(614) 253-7981
Oklahoma (see Texas {Gulf Coast})
Oregon American Red Cross
Blood Services
Pacific Northwest region
(503) 243-5286
Pennsylvania American Red Cross
Blood Services
Penn-Jersey region
(215) 299-4126
Puerto Rico American Red Cross
Puerto Rico Blood
Services
(809) 759-7979
Rhode Island Rhode Island Blood Center
(401) 863-8368
South Carolina American Red Cross
Blood Services
South Carolina region
(803) 256-2301
South Dakota (see Wisconsin, S.E.)
Tennessee American Red Cross
Nashville region
(615) 327-1931, ext. 315
Texas Gulf Coast Regional
Blood Center
(713) 791-6250
American Red Cross
Blood Services
Central Texas region
(817) 776-8754
American Red Cross
Blood Services
Red River region
(817) 322-8686
Utah (see California, northern)
Vermont American Red Cross
Blood Services
Vermont-New Hampshire
region
(802) 658-6400, ext 217
Virginia (also see American Red Cross
Washington, DC) Blood Services
Tidewater region
(804) 446-7709
Richmond Metropolitan
Blood Service
(804) 359-5100
American Red Cross
Blood Services
Appalachian region
(703) 985-3595
Washington Puget Sound Blood Center
(206) 292-6525
Washington, DC American Red Cross
Blood Services
Washington region
(202) 728-6426
West Virginia (see Washington, DC)
Wisconsin The Blood Center of
S.E. Wisconsin
(414) 933-5000
American Red Cross
Blood Services
Badger region
(608) 255-0021
Wyoming (see California, northern)
Other countries
Canada Canadian Red Cross
Blood Transfusion Service
National Office
(416) 923-6692
Central and South Florida Community
South America Blood Center
(305) 326-8888
All other countries American Red Cross
Blood Services
Northeast region
(617) 449-0773
American Red Cross
Blood Services
(617) 731-2130
---------------------------------------------------------------------
=======================================================================
Return to top. Disclaimer All MMWR HTML documents published before January 1993 are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 08/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}