 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Exposure to Patients With Meningococcal Disease on Aircrafts ---United States, 1999--2001Neisseria meningitidis is a leading cause of bacterial meningitis and sepsis in children and young adults in the United States and is spread through direct contact with respiratory secretions (1). Persons in close contact with patients who have meningococcal disease are at increased risk for contracting the disease (1). Commercial aircraft are suitable environments for the spread of airborne pathogens, including N. meningitidis (2). A case of air-travel--associated meningococcal disease is defined as a patient who meets the case definition of meningococcal disease (3) within 14 days of travel on a flight of at least 8 hours duration. Because of concerns about disease transmission aboard aircraft, CDC has developed recommendations to ensure a standard approach to management of airline contacts. This report presents a case of air-travel--associated meningococcal disease and presents guidelines for the management of persons potentially exposed to meningococcus during air travel. Case ReportOn May 24, 2001, the New York Department of Health (NYDH) reported a 62-year-old man with meningococcal meningitis to the CDC quarantine station at John F. Kennedy (JFK) International Airport. On May 20, the passenger arrived from Sydney, Australia, after changing planes at Los Angeles International Airport. He began to feel ill during his flight and was assisted from the plane in a wheelchair. No public health officer at JFK airport was contacted to report an ill passenger on board the aircraft. On May 23, the man was hospitalized, and microscopic examination of cerebrospinal fluid (CSF) showed gram-negative diplococci. On May 25, the patient's CSF grew N. meningitidis, serogroup B, and he was diagnosed with meningococcal meningitis. NYDH requested assistance in identifying any airline passengers who required chemoprophylaxis. A New York quarantine inspector contacted the airline station manager to request the flight manifest and passenger contact information. The manifest was not available locally and could be obtained only from the airline's corporate headquarters in Australia. Because contact information from the airline was not complete, quarantine inspectors in New York and Los Angeles manually extracted passenger names and addresses from the customs declaration forms that each international traveler completes on entry to the United States. Within 2 days, they were able to identify the two passengers sitting on either side of the patient. This information was relayed to the two passengers' respective state health departments. One exposed contact could not be located at the address provided on the customs form. The other contact was asymptomatic and the state health department recommended that he take appropriate chemoprophylaxis. Surveillance MeasuresCDC employs a passive surveillance system by which local health departments report suspected cases of air-travel--associated meningococcal disease. From February 1999 through May 2001, CDC received 21 reports, an average of one report every 6 weeks (Figure 1). Approximately half of these cases were reported to a CDC airport quarantine station, and the rest were reported to CDC headquarters. The mean time between the completion of the flight and the onset of illness was 1.9 days (range: 0--10 days). Five case-patients had onset of illness before arrival. Reported by: M Layton, MD, New York City Dept of Health. M Cartter, MD, Connecticut State Dept of Public Health. E Bresnitz, MD, State Epidemiologist, New Jersey Dept of Health and Senior Svcs. S Wiersma, MD, Florida Dept of Health. L Mascola, MD, Los Angeles County Dept of Health Svcs. Meningitis and Special Pathogens Br, Div of Bacterial and Mycotic Diseases; Surveillance and Epidemiology Br, Div of Global Migration and Quarantine, National Center for Infectious Diseases; and an EIS Officer, CDC. Editorial Note:Chemoprophylaxis of persons in close contact with an index case-patient is the primary means for prevention of secondary cases of meningococcal disease. Close contacts at high risk for secondary disease include household members, day care center contacts, and anyone directly exposed to a patient's oral secretions (e.g., through kissing and endotracheal tube management) (1). The attack rate among household contacts of patients with meningococcal disease is an estimated 500--800 times greater than the general population (4). Because the risk for illness is highest during the first few days after infection, chemoprophylaxis should be administered as soon as possible (ideally within 24 hours) after contact with an index case-patient. Chemoprophylaxis administered >14 days is probably of limited or no value. Systemic antibiotics that effectively eliminate nasopharyngeal carriage of N. meningitidis include rifampin, ciprofloxacin, and ceftriaxone (Table 1) (1). No cases of secondary disease among air travel contacts of persons with meningococcal disease have been reported; however, passengers who are seated next to a person with meningococcal disease for a prolonged flight may be at higher risk for developing meningococcal disease. Seven investigations of Mycobacterium tuberculosis transmission on airplanes suggest that in-flight transmission of bacterial respiratory pathogens do occur (5). One of these investigations documented transmission of M. tuberculosis from a symptomatic index case-patient to six passengers with no other risk factors who were sitting in the same section of a commercial aircraft during a long flight (>8 hours) (6). CDC, in collaboration with the Council of State and Territorial Epidemiologists, has developed procedures for the management of air-travel--associated exposure to meningococcus (7,8). These recommendations are intended to provide uniformity to the procedures followed by the various federal, state, and local health agencies involved in contact investigation and management for meningococcal cases occurring in airline passengers. Health departments from the jurisdiction where the patient resides and where the patient has been visiting should be contacted promptly to facilitate antimicrobial chemoprophylaxis of household members, day care center contacts, and other possible close contacts. Household members traveling with an index case-patient, persons traveling with an index case-patient who have had prolonged close contact (e.g., roommates), and anyone having direct contact with a patient's oral secretions should be identified and the need for antimicrobial chemoprophylaxis evaluated. The assessment of risk to passengers and flight crew members should be based on the flight duration and seating proximity to the index case-patient. For flights of >8 hours, including ground time, passengers who are seated immediately next to an index case-patient are more likely to be exposed directly to the patient's oral secretions and are probably at higher risk than those seated farther from the index case-patient. In the absence of data about increased risk to other passengers, antimicrobial chemoprophylaxis should be considered for those passengers seated in either seat next to an index case-patient. Because passengers disperse over a wide area after arrival, federal health authorities should work with the travel industry to identify passengers requiring chemoprophylaxis. On notification of an air passenger with potential meningococcal disease, the CDC quarantine station with jurisdiction over the port of entry will contact the airline to obtain a passenger manifest, which includes the name and seat assignment for all passengers on the flight. Once quarantine inspectors identify potentially exposed travelers, their names are cross-referenced with the airline's passenger history record that includes a telephone number and frequently an address for the patient. State or local health departments in the patient's area of residence should be responsible for contacting each exposed traveler. If the exposed passenger is a foreign national temporarily visiting the United States, the CDC quarantine station can assist in locating and contacting the person. In addition, the quarantine station will notify the national health authority of the passenger's home country. Most cases of meningococcal disease among air passengers are not detected until after the flight has landed and the passengers have dispersed. CDC and state health departments should enhance surveillance for secondary cases associated with air travel. To facilitate this process, state and local health departments and private physicians should ask all persons with meningococcal disease about recent travel, including flight information. Occasionally, a passenger's illness becomes evident during a flight. During the previous 2 years, five passengers with symptomatic meningococcal disease have flown on international flights to the United States. The airline crew reported only one of these cases before arrival, a critically ill passenger who later died. Federal law requires that an ill passenger on an international conveyance must be reported to the Public Health Service before arrival in the United States*. The pilot should contact the closest of eight CDC quarantine stations that are located at international airports to report an ill passenger. Quarantine station staff will assist the airline in management of the ill passenger and notification of fellow passengers and crew members. Many pilots are not familiar with the requirement to report arriving ill passengers aboard flights. Commercial pilot in-flight manuals should be updated to include procedures for managing an ill passenger and detailed information on how to contact the closest CDC quarantine station. Notification of meningococcal exposures on an aircraft is frequently hindered by difficulty in obtaining passenger contact information. Airlines typically maintain the passenger manifest and history records for 2--7 days, after which they are either archived or destroyed. Some airborne pathogens other than meningococcus have longer incubation periods, including tuberculosis and many bioterrorism agents. As a result, it may be necessary to contact passengers several weeks after a flight has disembarked. To facilitate timely identification and public health notification and management of at-risk passengers, commercial airlines should ensure that electronic passenger manifests and contact information are preserved and readily available for a period of at least 1 month following disembarkation. References
* 42 CFR 71.21(b). Table 1 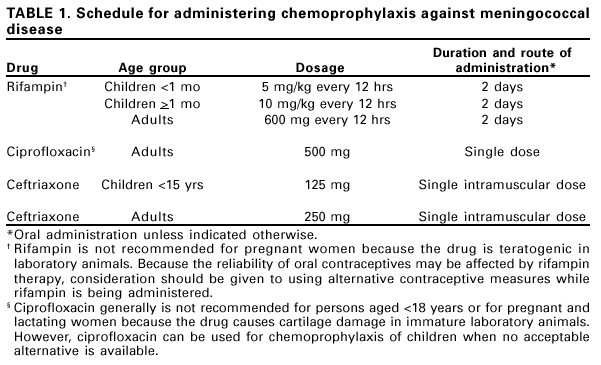 Return to top. Figure 1 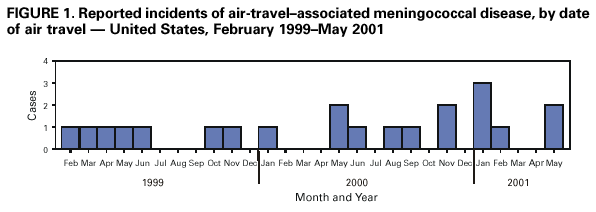 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 6/15/2001 |
|||||||||
This page last reviewed 6/15/2001
|