 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Trends in Tuberculosis --- United States, 2004During 2004, a total of 14,511 confirmed tuberculosis (TB) cases (4.9 cases per 100,000 population) were reported in the United States, representing a 3.3% decline in the rate from 2003. Slightly more than half (53.7%) of U.S. cases were in foreign-born persons. This report summarizes data from the national TB surveillance system for 2004 and describes trends since 1993. Findings indicate that although the 2004 TB rate was the lowest recorded in the United States since national reporting began in 1953, the declines in rates for 2003 (2.3%) and 2004 (3.3%) were the smallest since 1993. In addition, TB rates greater than the U.S. average continue to be reported in certain racial/ethnic populations*; in 2004, Hispanics, blacks, and Asians had TB rates 7.5, 8.3, and 20.0 times higher than whites, respectively. Essential elements for controlling TB in the United States include sufficient local resources, interventions targeted to populations with the highest TB rates, and continued collaborative efforts with other nations to reduce TB globally. The 50 states and the District of Columbia (DC) report cases to the national TB surveillance system at CDC by using a standard case definition and report form (1). Provisional reports, updated as of February 16, 2005, were used for this analysis. U.S. census population estimates were used to calculate national and state TB rates (2) and rates for racial/ethnic populations (3) and for foreign-born and U.S.-born† persons (5). During 2004, a total of 30 (58.8%) states§ reported a decline in cases from 2003. Seventeen states¶ and DC reported an increase in cases, and three states** reported the same number of cases as in 2003. Seven states reported more than 400 cases each in 2004; collectively these states accounted for 8,689 cases, or 59.9% of the national case total. Of these seven states, two reported increases for 2004 (Texas, 4.0% and Florida, 1.0%); the other five states reported decreases (California, 8.4%; Georgia, 2.5%; Illinois, 10.9%; New Jersey, 3.3%; and New York, 7.3%). States with the largest numbers of TB cases also had the highest TB rates, with certain exceptions. Illinois and New Jersey each had more than 400 cases but were not among the top 20% of rates (i.e., >5.6 per 100,000 population) (Figure 1). The number of cases reported by Alaska (43 cases), DC (81), and Hawaii (116) were less than the median of 127, but each area reported rates of >5.6. Many of the states reporting the lowest TB rates were in the Rocky Mountains area, the upper Midwest, or the Northeast. In 2004, among U.S.-born persons, 6,637 cases were reported, a decrease of 3.7% compared with 2003 and 61.9% compared with 1993 (Figure 2). The 2004 TB rate for U.S.-born persons was 2.6 per 100,000 population, a decrease of 4.3% from 2003 and 64.6% from 1993. In 2004, among foreign-born persons, 7,701 cases were reported. In contrast to the substantial decline in cases among U.S.-born persons since 1993, the number of cases reported among foreign-born persons has not changed substantially. From 1996 to 2000, the TB rate for foreign-born persons decreased 22.4%, from 32.6 to 25.3; from 2000 to 2004, the rate decreased 11.2%, from 25.3 to 22.5. During these periods, the growth of the foreign-born population in the United States ranged from a 26.6% increase during 1996--2000 to a 14.2% increase during 2000--2004. In 2004, for the first time, TB was reported more frequently among Hispanics than among any other racial/ethnic population (Table). The number of cases in Hispanics increased 1.2%, from 4,109 in 2003 to 4,160 in 2004. However, the TB rate for Hispanics decreased, from 10.3 in 2003 to 10.1 in 2004. The increase in case counts, but decrease in rates, reflects a 3.6% increase in the 2004 U.S. population of Hispanics compared with 2003. For blacks, whites, and Asians, the case numbers and rates both decreased. Of 3,221 Asians with TB and known origin of birth, 3,074 (95.4%) were foreign born; of 4,105 Hispanics with TB, 3,037 (74.0%) were foreign born; and, of 3,981 blacks with TB, 1,055 (26.5%) were foreign born. The recommended length of drug therapy for most types of TB is 6--9 months. In 2001, the latest year for which completion-of-therapy data are available, the percentage of patients who completed therapy within 1 year†† was 81.4% for U.S.-born patients and 80.4% for foreign-born patients. In 2003, the most recent year for which drug-susceptibility data are available, 114 cases of multidrug-resistant (MDR) TB§§ were reported. These MDR TB cases represent 1.0% of the 11,040 cases for which drug-susceptibility test results were reported in 2003 and a 76.5% decline from the 486 MDR TB cases reported in 1993. In 2003, a total of 0.6% (28 cases) of U.S.-born and 1.4% (86 cases) of foreign-born persons had MDR TB, a 91.6% and 42.7% decline, respectively, in MDR TB cases from 1993. Reported by: Div of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:During 1993--2002, the United States reported steady declines in annual TB rates, with an average decline of 6.6% (4). However, annual declines in rates for 2003 and 2004 were the smallest since 1993, raising concerns that the progress toward eliminating TB might be slowing. Steep declines have occurred in TB rates among U.S.-born persons; since 1993, the TB rate among U.S.-born persons has declined 64.6%, to an all-time low of 2.6 per 100,000 population in 2004. Smaller declines have occurred among foreign-born persons; since 1993, the TB rate among those foreign born has declined 33.9%, to a rate of 22.5, approximately 8.7 times higher than the rate for those born in the United States. In 2001, the percentages of both U.S.-born (81.4%) and foreign-born (80.4%) patients who completed therapy within 1 year were similar but fell short of the 2010 national health target of 90% (objective no. 14.12) (6). A greater percentage of foreign-born than U.S.-born patients had MDR TB, reflecting likely exposure to TB in countries where rates of MDR TB are higher than in the United States. To address the high rate of TB among foreign-born persons, CDC is collaborating with other national and international public health organizations to 1) improve overseas screening of immigrants and refugees by systematically monitoring and evaluating the screening process, 2) strengthen the current notification system that alerts local health departments about the arrival of immigrants or refugees who have suspected TB, 3) improve coordination of TB-control activities between the United States and Mexico to ensure completion of treatment among TB patients who cross the border, 4) test recent arrivals from high-incidence countries for latent TB infection and treat them to completion, and 5) survey foreign-born TB patients in the United States to determine opportunities for improving prevention and control interventions. In addition, CDC continues to strengthen collaborations with international partners, including the Stop TB Partnership of the World Health Organization (http://www.stoptb.org), to improve TB control in high-incidence countries. A disproportionately large number of TB cases are reported among blacks, most of whom were born in the United States; in 2004, the TB rate for blacks was 8.3 times greater than that for whites. In southeastern states, blacks with TB are more likely than whites to have certain risk factors, such as human immunodeficiency virus infection, incarceration, or excess alcohol or drug use, which suggests that differences in socioeconomic status, health status, and opportunity for TB exposure, underlie increased risk for TB (7). However, the percentages of blacks receiving directly observed therapy (81.0%) and completing treatment on time (81.6%) were similar to the percentages among whites (74.7% and 82.2%, respectively). To address the high rate of TB in blacks in the United States, CDC has funded three U.S. demonstration projects (in Chicago, Illinois; Georgia; and South Carolina), in collaboration with state and local health departments, to identify innovative strategies for improving TB diagnosis, screening, and treatment adherence in communities with black persons at high risk. CDC is also conducting a formative research and intervention study in collaboration with the Research Triangle Institute. This study will 1) examine barriers to health-seeking behaviors and treatment adherence for blacks with or at risk for TB, 2) determine barriers to TB guideline adherence among providers who serve this population, 3) develop and test interventions to overcome identified barriers, and 4) improve partnerships and collaborations among TB programs and providers and organizations serving this population. Despite these targeted efforts to control TB, the recent deceleration of the decline in TB cases indicates the need for increased measures (e.g., improved case management and contact investigation, intensified testing of populations at high risk, better treatments and diagnostic tools, improved understanding of TB transmission, and continued collaborative efforts with other nations to reduce TB globally). These measures are required for complete implementation of the Institute of Medicine's recommendations for eliminating TB in the United States (8). Final data for 2004 will be published in fall 2005 in the CDC surveillance report, Reported Tuberculosis in the United States. Acknowledgments The findings in this report are based on surveillance data contributed by TB-control officials in state and local health departments. References
* For this report, persons identified as white, black, Asian, and of other/unknown races are all non-Hispanic. Persons identified as Hispanic might be of any race. † A U.S.-born person is defined as someone born in the United States or its associated jurisdictions or someone born in a foreign country but having at least one U.S.-born parent. All other persons not meeting this definition were classified as foreign-born (4). For 2004, patients with unknown origin of birth represented 1.2% (173) of total cases. § States reporting declines in cases in 2004 (cases, % decrease from 2003 to 2004): California (2,988, 8.4%), New York (1,364, 7.3%), Illinois (568, 10.9%), Georgia (528, 2.5%), New Jersey (482, 3.3%), Virginia (329, 2.7%), Pennsylvania (327, 3.0%), Tennessee (279, 3.4%), Arizona (272, 10.4%), Louisiana (249, 4.3%), Washington (244, 3.5%), South Carolina (234, 9.0%), Ohio (219, 4.5%), Alabama (211, 18.7%), Minnesota (199, 7.7%), Indiana (129, 10.3%), Kentucky (127, 8.6%), Missouri (127, 3.7%), Mississippi (119, 7.7%), Connecticut (101, 9.4%), Nevada (95, 13.9%), Kansas (62, 17.7%), Alaska (43, 25.4%), New Mexico (42, 15.4%), Utah (36, 9.1%), Maine (20, 17.2%), Idaho (11, 17.0%), South Dakota (11, 45.4%), Vermont (six, 33.6%), and North Dakota (four, 33.4%). ¶ States/areas reporting an increase in cases in 2004 (cases, % increase from 2003 to 2004): Texas (1,683, 4.0%), Florida (1,076, 1.0%), North Carolina (382, 0.7%), Maryland (314, 16.2%), Massachusetts (284, 8.9%), Michigan (273, 12.0%), Oklahoma (179, 9.3%), Arkansas (132, 2.2%), Colorado (127, 13.1%), Wisconsin (95, 43.0%), DC (81, 3.3%), Rhode Island (51, 10.4%), Iowa (47, 17.0%), Nebraska (39, 38.5%), New Hampshire (24, 58.7%), West Virginia (24, 14.0%), Montana (15, 112.3%), and Wyoming (five, 23.9%). ** States reporting the same number of cases in 2003 and 2004 include Hawaii (116), Oregon (106), and Delaware (32). †† Completion-of-therapy data exclude persons who died during therapy, persons with initial isolate resistant to rifampin, and pediatric patients (i.e., aged <15 years) with meningeal, bone or joint, or miliary disease. §§ Defined as resistant to at least isoniazid and rifampin.
Figure 1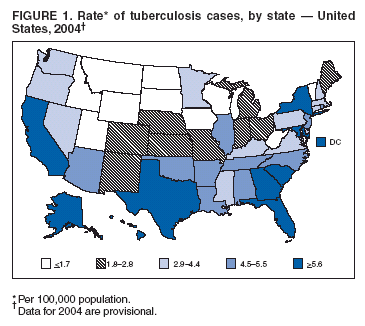 Return to top. Figure 2 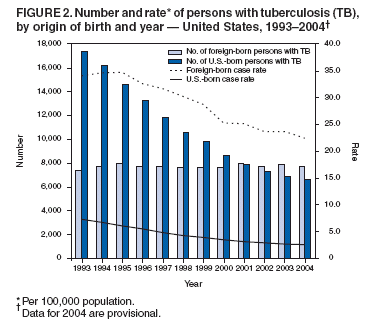 Return to top. Table 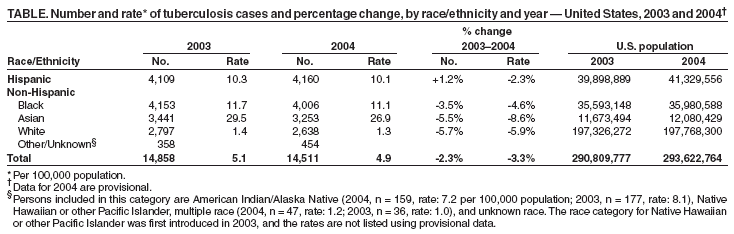 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 3/17/2005 |
|||||||||
This page last reviewed 3/17/2005
|