 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Increase in African Immigrants and Refugees with Tuberculosis ---Seattle-King County, Washington, 1998--2001Please note: An erratum has been published for this article. To view the erratum, please click here. The proportion of tuberculosis (TB) cases among foreign-born persons in the United States has increased steadily, accounting for half of reported cases in 2001 for which country-of-origin information was available. During 1998--2001, the annual number of TB cases among African immigrants and refugees in Seattle and all of King County increased approximately threefold to that during 1993--1997. This report summarizes the investigation of cases during 1998--2001 and outlines the public health interventions implemented to prevent TB in this population. The findings indicate that in Seattle-King County, persons at risk for TB who have arrived recently in the United States were primarily from the African-Horn countries of Eritrea, Ethiopia, and Somalia. Primary health-care providers and civil surgeons (i.e., physicians appointed by the Immigration and Naturalization Service to screen for medical conditions as required for changes of immigration status) should be aware of the high TB rate among African immigrants, especially within the first 5 years after immigration, and be alert for severe extrapulmonary forms of TB. TB surveillance data are derived from case reports submitted to and verified by the Seattle-King County Public Health (SKCPH) TB Control Program. During 1993--1997, fewer than 10 cases of TB in African immigrants were reported each year (5%--10% of the annual total). The number of cases began increasing in 1998 (Figure). In 2001, of 139 TB cases reported in Seattle-King County, 28 (20%) were among African immigrants. During 1998--2001, of Seattle-King County's 486 TB cases, 79 (16%) were among African immigrants, 67 (85%) of whom were from Eritrea, Ethiopia, and Somalia. Two each were from Kenya, Uganda, and Zambia, and one each was from six other African countries (Gambia, Guinea, Liberia, Malawi, Rwanda, and Zaire). Of 281 other foreign-born patients with TB reported during the same period, 68 were from Vietnam, 59 were from the Philippines, 24 were from India, and the remainder were from 69 other countries. Characteristics of patients and of TB disease were similar for the 67 African-Horn immigrants and the 12 immigrants from other African countries; 40 (51%) cases were among men. Of 69 patients who were tested for human immunodeficiency virus infection, five (7%) tested positive. The median age of the 79 African immigrants with TB was 27 years (range: 2--70 years); five (6%) patients were aged <15 years, and 62 (78%) were aged <35 years, compared with 117 (40%) of 281 other foreign-born patients aged <35 years with TB reported during the same period (p<0.01). For African immigrants, TB occurred sooner after immigration than for other immigrants. Of 71 cases in African immigrants with known arrival dates, 32 (45%) occurred within 1 year after arrival, and 60 (65%) occurred within 5 years, compared with 38 (16%) and 98 (41%), respectively, of 239 TB cases among other immigrants (p<0.01). Among African immigrants with TB reported during 1998--2001, a total of 37 (47%) had pulmonary disease, 39 (49%) had extrapulmonary disease, and three (4%) had both, resulting in a total of 42 (53%) patients with extrapulmonary disease. This proportion was greater than the national average of 27% reported in 2000 (1) but similar to the 127 (45%) of 281 immigrants from other continents (p=0.21). Among the 42 African immigrants with extrapulmonary TB, eight (19%) had TB of the spine (i.e., Pott's disease), compared with nine (7%) of 127 extrapulmonary TB cases in the other foreign-born patients (p=0.04). Of the 72 initial isolates of Mycobacterium tuberculosis from African immigrants with TB, four (6%) were resistant to isoniazid but not to rifampin, and one was resistant to isoniazid, rifampin, ethambutol, pyrazinamide, and streptomycin. Of 258 initial isolates from other immigrants, 27 (10%) were resistant to isoniazid but not rifampin, and two were resistant to both isoniazid and rifampin. In the SKCPH Refugee Screening Program, the number of refugees arriving from Eritrea, Ethiopia, and Somalia into Seattle-King County increased from 59 in 1998 to 425 in 2001. An estimated 10,314 (range: 3,952--16,676) residents of Seattle-King County were born in Africa (2). On the basis of this denominator, the annual rate of TB for African immigrants was 262 per 100,000 population in 2001. For all of Seattle-King County, the 2001 TB rate was eight. Medical records for the 27 African immigrants reported with TB in 1998 and 1999 were reviewed for missed opportunities to prevent TB. Among 25 immigrants with complete records, 10 (40%) had received tuberculin skin testing before developing TB. Six of these patients had positive results and started isoniazid treatment for latent TB infection (LTBI); two reportedly completed treatment. Five (20%) other patients had not been tested for LTBI, although they had received primary health-care services before their diagnosis of TB. The remaining 10 (40%) were not known to have received medical care in the United States before their diagnosis of TB. Reported by: C Nolan, MD, S Goldberg, MD, J Wallace, MN, Public Health, Seattle-King County, Washington. Div of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention; P Dewan, MD, EIS Officer, CDC. Editorial Note:The findings in this report indicate that in Seattle-King County, the immigrant groups at risk for TB were primarily from the African-Horn countries of Eritrea, Ethiopia, and Somalia. The World Health Organization estimates that the TB rate is 260 per 100,000 population for Ethiopia and 229 for all of Africa (3), rates almost identical to those observed in Seattle-King County. Increases in African immigration and TB are occurring elsewhere; in the United States, the number of refugees from Africa increased from 6,662 in 1998 to an estimated 18,979 in 2001 (4,5). State and local health departments should monitor TB surveillance trends to focus case-finding and prevention activities. Seattle-King County implemented a flexible community-based approach that establishes partnerships with immigrant service systems, engages groups of immigrants in an exchange of TB information, and employs immigrants to serve as outreach workers in their communities (6). For example, the SKCPH TB Control Program and the International Medicine Clinic at Harborview Medical Center, Seattle, implemented a pilot program hiring and training recent refugees from three countries (Somalia, the former Soviet Union, and the former Yugoslavia) to work as outreach workers for TB-prevention services targeted to refugees. These workers visit patients who are undergoing treatment for LTBI or TB and serve as mediators between patients and their health-care providers. The workers also assist with other resettlement issues (e.g., social needs, education, and overall health care). Since the program was implemented in 1999, the rate of TB treatment acceptance among targeted refugees increased from 51% (46 of 90) in 1998 to 86% (224 of 260) in 2000, and the rate of treatment completion increased from 50% (23 of 46) to 87% (194 of 224) (6). Primary health-care providers and civil surgeons (7,8), should be aware of the high TB rate among African immigrants, especially within the first 5 years after immigration, and be alert for severe extrapulmonary forms of TB (e.g., Pott's disease). Immigrants, including refugees, from countries with high rates of TB (3) should be screened for active TB and tested for LTBI when they enter the health-care system. Candidates for treatment of LTBI should be selected and treated in accordance with guidelines from the American Thoracic Society and CDC (9). References
Acknowledgment This report is based on data contributed by K Janusz, Washington Dept of Health.
Figure 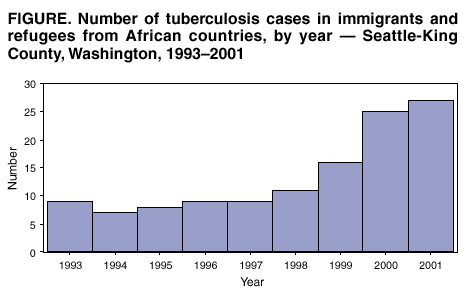 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/3/2002 |
|||||||||
This page last reviewed 10/3/2002
|