 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
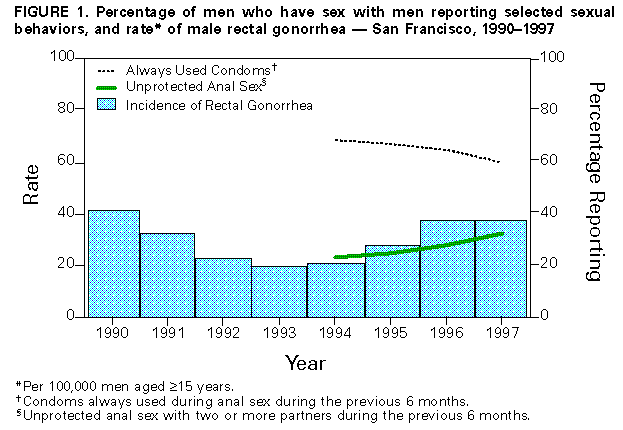
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Increases in Unsafe Sex and Rectal Gonorrhea Among Men Who Have Sex With Men -- San Francisco, California, 1994-1997Reductions in AIDS cases among men who have sex with men (MSM) have been attributed in part to widespread declines in unprotected anal sex since the mid-1980s (1) and use of increasingly effective antiretroviral therapy (ART) since the mid-1990s (2). Because data about HIV infection incidence are limited, other indicators of transmission risk have been used. In San Francisco, data from annual behavioral surveys among MSM (1994-1997) and from the sexually transmitted disease (STD) surveillance program (1990-1997) were analyzed to characterize changes in HIV risk behaviors of MSM and changes in incidence of male rectal gonorrhea. This report describes the findings of these analyses, which indicate increases in unsafe sexual behavior and increases in rates of rectal gonorrhea among MSM. From 1994 through 1997, volunteers in The Stop AIDS Project, a San Francisco community-based organization, conducted standardized annual surveys in which MSM were approached in various settings (e.g., neighborhoods, clubs, bars, and outdoor events) and asked to respond to a peer-administered, one-page questionnaire. Persons were excluded if they had participated previously during the same year. Methods were identical across years. First-time interviews were completed among 21,857 MSM; 6223, 5989, 5472, and 4173 interviews were completed each respective year. Demographic and sexual behavior information was collected annually; in 1997, subjects were asked whether they knew the HIV serostatus of their sex partners. In the survey, unprotected anal intercourse (UAI) was defined as insertive or receptive anal sex during the previous 6 months without always using condoms. Multiple partners was defined as more than one sex partner during the previous 6 months. Male rectal gonorrhea data reported to the San Francisco Department of Public Health, Sexually Transmitted Disease Control Section, were reviewed. The annual incidence from 1994 through 1997 was calculated as cases per 100,000 adult men aged greater than or equal to 15 years (1990 U.S. census data were used for the denominator). Changes in sexual behaviors and rectal gonorrhea incidence over time were assessed using the chi-square test for trend. The proportion of surveyed MSM who reported having had anal sex increased from 57.6% (95% confidence interval {CI}=56.4%-58.9%) in 1994 to 61.2% (95% CI=60.1%-63.1%) in 1997 (pless than 0.01). Among MSM who had had anal sex, the proportion reporting "always" using condoms declined from 69.6% (95% CI=68.1%-71.1%) in 1994 to 60.8% (95% CI=58.9%-62.7%) in 1997 (pless than 0.01) (Figure_1). The most pronounced decline in consistent condom use occurred among men aged 26-29 years (from 68.2% {95% CI=64.8%-71.5%} in 1994 to 58.0% {95% CI=53.7%-62.1%} in 1997). The proportion of men who reported having had multiple sex partners and UAI increased from 23.6% (95% CI=21.9%-25.4%) in 1994 to 33.3% (95% CI=31.1%-35.6%) in 1997 (pless than 0.01). The largest increase in this risk behavior was among respondents aged less than or equal to 25 years (from 22.0% {95% CI=18.4%-25.9%} in 1994 to 32.1% {95% CI=27.7%-36.7%} in 1997; pless than 0.01). Decreasing consistent condom use and increasing proportions of MSM reporting UAI with multiple partners occurred in all racial/ethnic groups. In 1997, 45% (95% CI=41.4%-48.8%) of 865 MSM who had had UAI during the previous 6 months also reported not knowing the HIV serostatus of all their sex partners. Among 525 MSM who had had UAI and multiple partners during the previous 6 months, 68.0% (95% CI=63.9%-72.7%) reported not knowing the HIV serostatus of all their sex partners. Male rectal gonorrhea incidence declined from 1990 through 1993 (42, 33, 23, and 20 per 100,000 adult men, respectively). From 1994 through 1997, the incidence increased from 21 to 38 per 100,000 adult men (pless than 0.01) (Figure_1). This increase in incidence was observed in all racial/ethnic and age groups but was highest among men aged 25-34 years (from 41 to 83 cases per 100,000 men aged 25-34 years, pless than 0.01). Reported by: KA Page-Shafer, PhD, W McFarland, MD, R Kohn, J Klausner, MD, MH Katz, MD, San Francisco Dept of Public Health, San Francisco; D Wohlfeiler, MPH, S Gibson, MSW, The Stop AIDS Project, San Francisco, California. Prevention Svcs Research Br, Program Evaluation Research Br, International Activities Br, Div of HIV/AIDS Prevention, and Epidemiology and Surveillance Br, Div of Sexually Transmitted Diseases Prevention, National Center for HIV, STD, and TB Prevention, CDC. Editorial NoteEditorial Note: The data described in this report suggest that increases in unsafe sexual behavior have occurred among MSM in San Francisco, resulting in increased risk for HIV infection and transmission. These data provide additional insight to a previous report of increasing gonorrhea among MSM in selected STD clinics (3) and document significant increases during 1994-1997 in rectal gonorrhea (a direct measure of UAI) and self-reported UAI among MSM. The increases in reported risk behaviors and the increases in STDs in San Francisco coincide with the expanded availability of effective ART in San Francisco and the United States. Although ART can result in decreased viral load and decreased risk for HIV transmission, advances in HIV treatment and the resulting declines in AIDS deaths in San Francisco and nationally might lead to increased risk behavior by MSM who perceive that HIV infection can be managed effectively (4). Because the prevalence of HIV infection among MSM in San Francisco is high, small increases in unsafe behaviors in this population may result in increases in HIV infection incidence. Recent data do not show changes in HIV infection incidence among young MSM (aged 18-29 years) in San Francisco (5). However, HIV transmission may lag behind the transmission of other STDs, including gonorrhea, for several reasons (e.g., differences in infectivity and treatment) (6). That increases in UAI may represent sex between mutually monogamous persons with concordant HIV serostatus (i.e., "negotiated safety") seems unlikely. One third of MSM reported UAI with multiple partners during the previous 6 months. Substantial numbers of men interviewed in 1997 reported not knowing the HIV infection status of all their partners. In addition, increases in rectal gonorrhea are inconsistent with increases in negotiated safe sex behaviors between MSM. The findings in this study are subject to at least four limitations. First, the sample of MSM in The Stop AIDS Project surveys may not be representative of the general MSM community in San Francisco. Second, the questionnaire did not distinguish insertive versus receptive anal sex, and it did not inquire specifically about condom use with persons whose HIV serostatus was unknown. Third, survey respondents who reported UAI may not be similar to persons who acquired rectal gonorrhea. Fourth, the survey was not designed to assess the association between decreases in AIDS prevalence, AIDS deaths, or other factors and the described risk behaviors. However, the population surveyed was large, and increases in reported risk behaviors were consistent across all age and racial/ethnic groups. Other studies have described high and increasing rates of sexual risk behavior among MSM in San Francisco (7), elsewhere in the United States (8), and in Canada (9). Male rectal gonorrhea is increasing among MSM amidst an overall decline in nationwide gonorrhea rates (10). During 1993-1997, national gonorrhea surveillance demonstrated an annual increase in the proportion of cases in males compared with cases in females in western states (CDC, unpublished data) consistent with an increase in gonorrhea infection among MSM. The data presented in this report suggest that the substantial reduction in sexual risk behaviors among MSM and the decreases in rectal gonorrhea during the 1980s and early 1990s cannot be assumed to be maintained indefinitely. The availability of ART and the possible perception of lower risk for infection from persons receiving ART may lead to misunderstandings and complacency toward safe-sex messages. MSM of all ages and races/ethnicities in San Francisco continue to engage in behaviors that put them at high risk for HIV infection, and HIV prevalence is highest among the MSM populations compared with heterosexual populations. As the epidemic continues, it remains important to maintain resources for prevention activities targeted toward MSM across all racial/ethnic and age groups. Public health prevention and community-based outreach efforts to reduce risk behaviors and STDs remain crucial to reach these populations. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 01/28/99 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}