
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Norovirus Outbreaks on Three College Campuses --- California, Michigan, and Wisconsin, 2008
Noroviruses are the most common cause of outbreaks of acute gastroenteritis worldwide (1). Norovirus outbreaks affect persons of all ages and occur in a wide variety of settings (e.g., nursing homes, hospitals, restaurants, communities, schools, day care centers, military barracks, and cruise ships) (2). During fall 2008, three norovirus outbreaks occurring on college campuses in California, Michigan, and Wisconsin were reported to CDC. Public health investigations led by the respective state and local health departments were conducted to characterize the extent of the outbreaks and implement appropriate control measures. This report summarizes the investigations of these outbreaks, which resulted in a total of approximately 1,000 cases of reported illness, including at least 10 hospitalizations, and prompted closure of one of the three campuses. Median duration of the three outbreaks was 19 days (range: 16--20 days), and the attack rates ranged from 1.5% to 12.9%. Because of the potential for widespread infection and rapid transmission on college campuses, efforts to prevent and control norovirus outbreaks in these settings should focus on promoting hand hygiene, environmental disinfection, and exclusion of ill food workers.
California
On October 3, 2008, the Los Angeles County Department of Public Health (LACDPH) was notified by a local university (enrollment: approximately 32,000) of at least 30 students visiting the student health center or local emergency departments with symptoms of acute gastroenteritis consistent with norovirus infection. LACDPH arranged collection of stool specimens for diagnoses, performed on-site interviews with ill students, and monitored daily reports of gastrointestinal illness from the student health center, local hospitals, and residence hall advisors. LACDPH made multiple site visits to inspect dining halls and dormitories and to monitor stadium food preparation and janitorial services during football games held on October 4 and 11. Alcohol-based hand sanitizers were installed in numerous cafeterias, classrooms, and sports venues. All students were asked via a single e-mail message from the campus administration to complete a web-based survey, which was used for case ascertainment and risk factor analysis. Persons with suspected acute gastroenteritis reported to LACDPH also were interviewed either in person or by telephone.
A case of acute gastroenteritis was defined as either 1) vomiting and diarrhea or 2) vomiting or diarrhea with at least two of the following symptoms: stomach cramps, nausea, fever, body aches, headache, and fatigue. A total of 5,227 students (16% of all students) completed the web-based survey, of whom 440 (8.4%) met the case definition. Illness onsets occurred during September 24--October 13 (Figure 1). Of 43 students interviewed directly by LACDPH, 38 additional cases were identified, resulting in a total case count of 478 and an overall campus attack rate of 1.5%. Among the patients, symptoms included nausea (87%), fatigue (83%), vomiting (78%), stomach cramps (73%), diarrhea (70%), headache (61%), body aches (55%), and subjective fever (47%). Mean duration of symptoms was 2.4 days. Mean age of patients was 20.4 years; 64% were female.
A total of 185 patients (39%) sought medical attention at the student health center, 35 (7.3%) visited an emergency department, and 10 (2.1%) were hospitalized for dehydration. Of 10 patients for whom stool specimens were submitted, six were positive for norovirus by real-time reverse transcription--polymerase chain reaction (rRT-PCR). All six had matching genetic sequences classified as GII.6 Seacroft, a strain that had not been found previously in California. A cohort study was conducted using data collected through the web-based survey to assess potential exposures that might have produced a spike in cases with illness onset October 3. However, no single event, residence hall, or eating venue was implicated as a significant risk factor, and no ill food handler was identified in the investigation.
Michigan
On November 6, 2008, the Ottawa County Health Department (OCHD) was notified by the medical clinic at a college (enrollment: approximately 3,000) of a sudden increase in the number of students reporting acute diarrhea and vomiting, from a baseline daily average of two to five cases to 60 cases on 1 day, November 6. OCHD reported this increased activity to the Michigan Department of Community Health (MDCH), which initiated an investigation. On November 6, MDCH sent a Health Alert notification to neighboring jurisdictions and a mass fax describing the surge in gastroenteritis along with disinfection guidelines* to community schools, health-care providers, and local medical facilities.
A case of acute gastroenteritis was defined as illness onset during November 1--21 in a student, faculty member, or staff member with diarrhea or vomiting and one or more of the following symptoms: nausea, body ache, headache, or self-reported fever. On November 7, the cumulative number of reported cases increased sharply to 130, suggesting a possible common-source exposure. Because the campus has only one primary dining facility and parent's day activities were beginning the following day, OCHD investigators were concerned that further spread could occur. To facilitate environmental disinfection and prevent opportunities for further outbreak amplification via either foodborne or person-to-person transmission in large gatherings, OCHD decided, in consultation with MDCH and administrators from the college, to close the campus until November 12, except for dormitories and the medical clinic.
During the campus closure, e-mail and text messages were sent to students, instructing them to stay in their residence unless illness required medical attention. Faculty and staff members were advised to stay home if ill until at least 72 hours after symptoms had ceased and to exercise proper hand washing techniques. Those experiencing illness were asked to reply electronically to a brief questionnaire requesting symptom history and residence. Parents of students and the news media were sent e-mail messages with ongoing updates on the outbreak, and relevant announcements were posted on the college website. Only take-out or delivery food services were available through dining facilities. Recommendations to students included promptly disinfecting dormitory room and bathroom surfaces and objects with dilute bleach solution, washing soiled linens and clothing, and frequent hand washing.
On the basis of electronic responses (n = 205) and direct reporting (n = 213) to the medical clinic, 418 (12.9%) of 3,238 students and 33 (5.2%) of 630 faculty and staff members met the outbreak case definition for gastroenteritis (Figure 2). Stool specimens from five patients were submitted for testing; all five were positive for norovirus by rRT-PCR and classified as genotype GI.4. Environmental health investigation of the three dining facilities revealed no violations; however, interviews with dining services staff indicated that three ill food service workers had worked briefly while symptomatic with vomiting and diarrhea at the main campus dining facility on November 4 before being sent home.
Wisconsin
On November 6, 2008, two students living in the same residence hall (hall A; population: 1,150) of a large university (enrollment: approximately 42,000) visited campus health services with symptoms of acute gastroenteritis characterized by vomiting, diarrhea, and abdominal pain. The two patients reported that an unspecified number of other students in hall A were ill with similar symptoms. In collaboration with the local and state health departments, campus health services initiated an investigation. Hall A staff members provided daily reports of the number of ill residents. A case of acute gastroenteritis was defined as vomiting or diarrhea (three or more loose stools in 24 hours).
Students were educated regarding hand washing, and cleaning of dormitories, public restrooms, and communal areas was implemented with cleaning agents approved for norovirus by the Environmental Protection Agency.† Additional cases continued to be reported during the week of November 10, including cases among students living in neighboring residence halls and a sorority house. To enhance surveillance, campus health services sent an e-mail message on November 14 to all 3,480 residents living in eight neighboring residence halls and to all 2,700 students who were members of a fraternity or sorority. Students who had experienced illness during the preceding 2 weeks were asked to complete an online questionnaire used for case ascertainment and descriptive analyses.
Approximately 200 students completed questionnaires, and 138 persons met the case definition for acute gastroenteritis. An additional 18 cases were identified among students visiting the campus health center, for a total of 156 cases. Among the 138 patients, 93 (67%) lived in hall A, 29 (21%) lived in five of the eight neighboring residence halls, nine (6.5%) lived in a sorority house, and 25 (18%) lived off campus (Figure 3). The overall attack rate was 2.2%. The attack rate was 8.1% among hall A residents and 3.5% among residents of the eight neighboring residence halls. Self-reported signs and symptoms of illness among students included diarrhea (92%), vomiting (88%), abdominal cramps (88%), chills (80%), body aches (81%), and subjective fever (65%). The median duration of illness was 2 days. None of the patients was hospitalized, although 36 (23%) consulted a health-care provider. Stool specimens were obtained from five patients, and two were positive by rRT-PCR for norovirus genogroup II.
Reported by: CM Roberts, MS, Univ of Wisconsin-Madison, J Archer, MS, Wisconsin Div of Public Health. T Renner, Office of Public Relations, Hope College; PA Heidel, MD, DL VandeBunte, Ottawa County Health Dept; BM Brennan, MSPH, Michigan Dept of Community Health. C Croker, MPH, R Reporter, MD, S Nakagawa-Ota, Los Angeles County Dept of Public Health, California. AJ Hall, DVM, Div of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC.
Editorial Note:
This report highlights the effect of norovirus outbreaks on these three college campuses and the demand for campus medical services. College campuses are at particularly high risk for norovirus outbreaks because of the extensive opportunities for transmission created by numerous shared exposures and living areas (3--5). Notably, the Wisconsin school had experienced a previous norovirus outbreak in 1999 attributed to direct person-to-person and fomite transmission in the shared living and bathroom areas of a dormitory (6). The ready access to health-care services that is typically present on college campuses also likely encourages increased reporting of illness relative to the general public, which can facilitate outbreak reporting.
The identification of a source of infection and targets for intervention is complicated by the multiple potential routes by which norovirus can be transmitted (1). The California university outbreak exhibited a sharp increase in cases suggestive of a point source, although no single facility or campus event was implicated. During the Michigan college outbreak, foodborne transmission was suggested by reports of ill food workers immediately before the spike in reported norovirus cases; however, no analytic investigation was conducted to support this hypothesis. In contrast, the propagation of cases, association with a specific residence hall, and the shape of the epidemic curve during the Wisconsin university outbreak are suggestive of primarily person-to-person transmission.
Control measures implemented in response to the Michigan outbreak included cancellation of all campus activities and closure of all buildings (excluding dormitories and the medical clinic) to enable extensive disinfection and promote social distancing. During norovirus outbreaks, particularly in institutional settings, temporary closure of public areas for the purpose of disinfection and cancellation of large gatherings often are indicated to help break or slow the cycle of transmission (7). In health-care settings, rapid closure of units experiencing norovirus outbreaks to new admissions has been associated with shorter outbreak duration (8). The number of cases declined after closure of the Michigan campus; however, the direct effect of campus closure on limiting further transmission is unclear.
The findings in this report are subject to at least four limitations. First, analytic studies were not performed during the outbreak investigations at the Michigan and Wisconsin schools, so specific exposures and risk factors could not be assessed. Second, because multiple control measures were implemented simultaneously in response to these three outbreaks, the efficacy of any single intervention could not be determined. Third, the majority of the data were self-reported through mostly passive electronic surveillance surveys that had relatively low response rates, likely resulting in underestimation of cases and attack rates. Finally, different case definitions were used in each of the three outbreaks because no standard case definition for norovirus infection exists. As such, outbreak-specific case definitions typically are developed during suspected norovirus outbreaks and tailored to the desired sensitivity and specificity of the investigation.
Norovirus exhibits many characteristics that can facilitate spread of infection and complicate interventions, including multiple potential modes of transmission, prolonged asymptomatic shedding, environmental stability of the virus, and lack of persistent cross-protective immunity (i.e., failure of prior infection to confer immunity to other norovirus strains) (1). Consistent with recommendations for general norovirus outbreak management (7), strategies to prevent and control norovirus on college campuses should focus on hand hygiene, environmental disinfection, and exclusion of ill food workers (Box). Additionally, the use of e-mail, text messaging, and the Internet all facilitated communication during these outbreaks, although the usefulness of these media for case ascertainment is unclear considering the relatively low response rates. Given the widespread access to these technological resources on college campuses, such methods might be helpful during future outbreaks for rapid health communications and to supplement traditional case ascertainment methods.
Acknowledgments
The findings in this report are based, in part, on contributions by the personnel of University of Southern California, Los Angeles; University of Wisconsin-Madison; and Hope College, Holland, Michigan.
References
- Patel MM, Hall AJ, Vinjé J, Parashar UD. Noroviruses: a comprehensive review. J Clin Virol 2009;44:1--8.
- Widdowson MA, Cramer EH, Hadley L, et al. Outbreaks of acute gastroenteritis on cruise ships and on land: identification of a predominant circulating strain of norovirus---United States, 2002. J Infect Dis 2004;190:27--36.
- Lieb S, Gunn RA, Medina R, et al. Norwalk virus gastroenteritis: an outbreak associated with a cafeteria at a college. Am J Epidemiol 1985;121:259--68.
- Alexander WJ, Holmes JR, Shaw JF, Riley WE, Roper WL. Norwalk virus outbreak at a college campus. South Med J 1986;79:33--6, 40.
- Moe CL, Christmas WA, Echols LJ, Miller SE. Outbreaks of acute gastroenteritis associated wtih Norwalk-like viruses in campus settings. J Am Coll Health 2001;50:57--66.
- CDC. Outbreaks of Norwalk-like viral gastroenteritis---Alaska and Wisconsin, 1999. MMWR 2000;49:207--11.
- CDC. "Norwalk-like viruses": public health consequences and outbreak management. MMWR 2001;50(No. RR-9).
- Lopman BA, Reacher MH, Vipond IB, et al. Epidemiology and cost of nosocomial gastroenteritis, Avon, England, 2002--2003. Emerg Infect Dis 2004;10:1827--34.
* Information available at http://www.michigan.gov/documents/Guidelines_for_Environmental_Cleaning_125846_7.pdf.
† Information available at http://www.epa.gov/oppad001/list_g_norovirus.pdf.
FIGURE 1. Number* of acute gastroenteritis cases† among students on a college campus, by date of illness onset --- California, September--October 2008
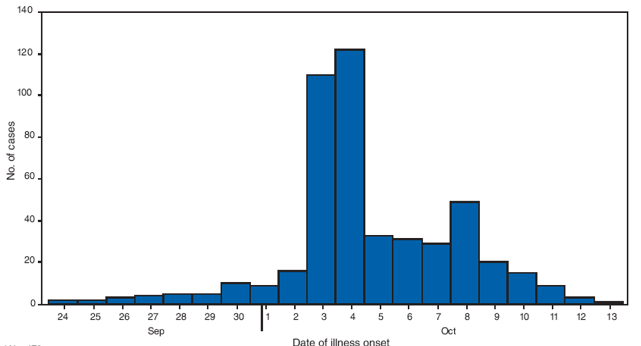
* N = 478.
† A case of acute gastroenteritis was defined as 1) vomiting and diarrhea or 2) vomiting or diarrhea with at least two of the following symptoms: stomach cramps, nausea, fever, body aches, headache, and fatigue.
Alternative Text: The figure above shows the number of acute gastroenteritis cases among students on a California college campus, by date of illness onset during September-October 2008. A case of acute gastroenteritis was defined as 1) vomiting and diarrhea or 2) vomiting or diarrhea with at least two of the following symptoms: stomach cramps, nausea, fever, body aches, headache, and fatigue. A total of 478 cases were identified. The majority of cases of illness onset occurred on October 3 and 4.
FIGURE 2. Number* of acute gastroenteritis cases† among students, faculty, and staff on a college campus, by date of illness onset --- Michigan, November 2008
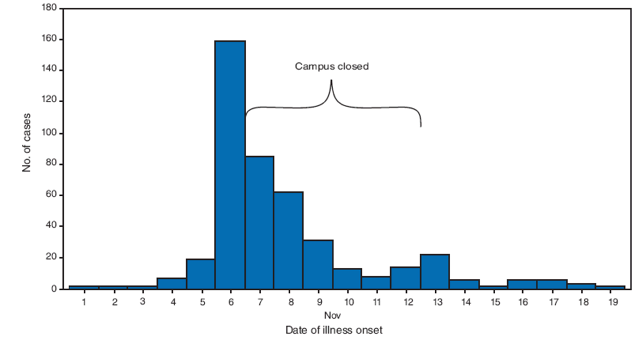
* N = 451.
† A case of acute gastroenteritis was defined as diarrhea or vomiting with one or more of the following symptoms: nausea, body ache, headache, or self-reported fever.
Alternative Text: The figure above shows the number of acute gastroenteritis cases among students, faculty, and staff on a Michigan college campus, by date of illness onset in November 2008. A case of acute gastroenteritis was defined as diarrhea or vomiting with one or more of the following symptoms: nausea, body ache, headache, or self-reported fever. A total of 451 students, faculty, and staff members met the outbreak case definition for acute gastroenteritis. The greatest number of cases of illness onset occurred on November 6. The campus was closed November 7-12.
FIGURE 3. Number* of acute gastroenteritis cases† among students on a college campus, by residence and date of illness onset --- Wisconsin, October--November 2008
* N = 156.
† A case of acute gastroenteritis was defined as vomiting or diarrhea (three or more loose stools in 24 hours).
Alternative Text: The figure above shows the number of acute gastroenteritis cases among students on a Wisconsin college campus, by residence and date of illness onset during October-November 2008. A case of acute gastroenteritis was defined as vomiting or diarrhea (three or more loose stools in 24 hours. A total of 156 students met the case definition for acute gastroenteritis.
BOX. CDC recommendations to prevent and control outbreaks of norovirus associated with college campuses
• Promote good hand hygiene, including frequent washing with soap and water and use of alcohol-based hand sanitizers (≥62% ethanol) as a complement to soap and water washing.
• Discourage sharing of eating utensils, toothbrushes, linens, or other personal items among students, especially when ill.
• Restrict ill students and staff from food preparation activities until at least 72 hours after symptoms have resolved.
• Encourage students to seek appropriate medical care when ill and limit social activities if symptoms are consistent with norovirus infection.
• Disinfect bathrooms and any areas possibly contaminated by ill persons, using a chlorine bleach solution with a concentration of 1,000--5,000 ppm (1:50--1:10 dilution of household bleach [5.25%]) or other approved disinfectant.*
• Consider closure of specific facilities and/or cancellation of events to help limit transmission during an outbreak.
• Disseminate prevention and control recommendations promptly during an outbreak, employing electronic communication resources (e.g., e-mail, Internet, and text messages) if available.
* Agents registered as effective against norovirus by the Environmental Protection Agency are listed at http://www.epa.gov/oppad001/list_g_norovirus.pdf. Evidence for efficacy against norovirus usually is based on studies using feline calicivirus (FCV) as a surrogate. However, FCV and norovirus exhibit different physiochemical properties, and whether inactivation of FCV reflects efficacy against norovirus is unclear.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/8/2009