|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
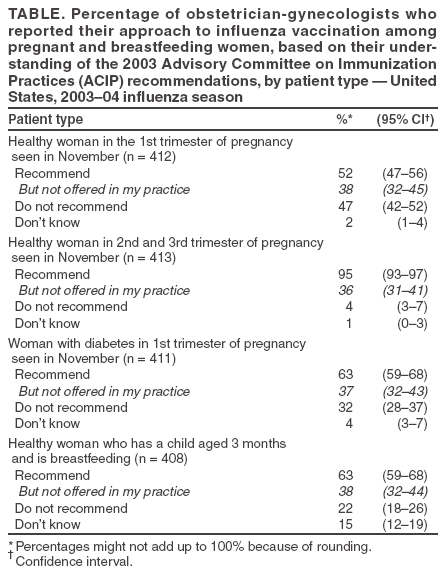
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Influenza Vaccination in Pregnancy: Practices Among Obstetrician-Gynecologists --- United States, 2003--04 Influenza SeasonWomen infected with influenza virus during pregnancy are at increased risk for serious complications and hospitalization (1). During 1997--2003, the Advisory Committee on Immunization Practices (ACIP) included healthy pregnant women who would be in their second or third trimester of pregnancy during the influenza season among those persons at high risk for whom influenza vaccination was indicated (2). Also included were women at any stage of pregnancy with certain chronic medical conditions, such as asthma, diabetes mellitus, or heart disease (2). ACIP emphasized that the influenza vaccine was safe for breastfeeding mothers and their infants and that household contacts of children aged <2 years also should be vaccinated (2). However, despite these recommendations, only 13% of pregnant women received influenza vaccination in 2003 (3). To assess understanding of the ACIP recommendations among obstetrician-gynecologists (OB/GYNs), the American College of Obstetricians and Gynecologists (ACOG), with support from CDC, surveyed a national sample of OB/GYNs in May 2004. This report describes the results of that survey, which indicated that 52% of OB/GYNs surveyed would recommend influenza vaccination for a healthy woman in the first trimester of pregnancy, 95% would recommend the vaccine for a healthy pregnant woman beyond the first trimester, and 63% would recommend vaccination for a woman with a medical condition in the first trimester. However, of the physicians who would recommend vaccination, 36%--38% reported that influenza vaccination was not offered in their practices. Increased efforts are needed to improve vaccine availability and to educate OB/GYNs regarding the updated ACIP recommendations on the use of influenza vaccine in the first trimester for both healthy pregnant women and pregnant women at high risk. In May 2004, ACOG mailed surveys to a random sample of 1,000 OB/GYNs who had current membership in ACOG. A second mailing was sent approximately 1 month after the first to physicians who had failed to respond. Physicians were asked about their approaches toward recommending and providing influenza vaccination for pregnant and postpartum women during the 2003--04 influenza season, a season with no shortage in vaccine supply. Physicians were asked to indicate their approach to influenza vaccination for four patient scenarios involving women in their practices (Table). In addition, physicians were asked whether they had seen pregnant patients whom they suspected had influenza and how often they tested these patients for influenza during the 2003--04 influenza season. Respondent demographic and practice-setting data also were collected. Exact binomial confidence intervals (CIs) were calculated. Completed surveys were received from 515 OB/GYNs (response rate: 52%). Respondents who had not seen obstetric patients during the 2003--04 influenza season were excluded (n = 102). A total of 413 OB/GYNs constituted the final sample. Median age of respondents included in the analysis was 45.8 years (range: 30--72 years); 56% of respondents were male. However, not all 413 physicians responded to each question. Among the OB/GYNs included in the analysis, 212 (52%) reported that they would recommend influenza vaccination to a healthy pregnant woman in the first trimester seen during the influenza season; of these, 81 (38%) reported that the vaccine was not offered by their practice. A total of 391 (95%) reported that they would recommend vaccination for a healthy pregnant woman in the second or third trimester, but 140 (36%) of these did not offer influenza vaccination in their practices. For a woman with diabetes who was in the first trimester of pregnancy, 260 (63%) reported that they would recommend influenza vaccination; of these, 97 (37%) indicated that the vaccine was not offered by their practices. Whereas 259 (63%) respondents reported that they would recommend influenza vaccination to a healthy postpartum woman who is breastfeeding, 98 (38%) indicated that the vaccine was not offered by their practice. Of the OB/GYNs who completed the survey, 243 (59%) reported seeing pregnant women in their practice whom they suspected of having influenza during the 2003--04 influenza season. However, of these, 203 (84%) reported that they rarely or never tested pregnant women for influenza. Reported by: B Bettes, PhD, D Hawks, MPH, J Schulkin, PhD, American College of Obstetricians and Gynecologists, Washington, DC. L Riley, MD, Harvard Medical School, Boston, MA. S Rasmussen, MD, J Mulinare, MD, Div of Birth Defects and Developmental Disabilities, H Atrash, MD, National Center on Birth Defects and Developmental Disabilities; C Bridges, MD, Epidemiology and Surveillance Div, N Allred, PhD, Immunization Svcs Div, National Immunization Program; CB Borkowf, PhD, Div of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention; KG Raleigh, PhD, EIS Officer, CDC. Editorial Note:The results of this study indicated that 52% of OB/GYNs supported the use of influenza vaccination during pregnancy in the first trimester for healthy women, 95% supported use in the second and third trimesters, and 63% reported that they would recommend vaccination to women with diabetes who were at any stage of pregnancy and to women who were breastfeeding. Nearly half of physicians reported that they would not recommend influenza vaccination for a healthy woman during the first trimester of pregnancy. This pattern is consistent with the 2003 ACIP recommendations, in place at the time of this survey, that acknowledged vaccination after 14 weeks' gestation and beyond as preferred by many providers for women without other underlying high-risk conditions, to avoid coincidental association with spontaneous abortions, which are common in the first trimester (2). In May 2004, after the survey was conducted, ACIP published simplified recommendations, which stated that vaccination is recommended in any trimester for healthy pregnant women and pregnant women with high-risk medical conditions (4). Whereas physicians frequently recommended influenza vaccination to pregnant women, vaccination often was not available in their practices. Although the reasons for not offering influenza vaccination in their practices were not explored, a study of OB/GYNs identified inadequate reimbursement, lack of vaccine information for patients, and liability concerns as main barriers to vaccination of pregnant women among physicians who did not offer influenza vaccination in their practices (5). These findings underscore the need to improve influenza vaccine availability and use for both healthy pregnant women and pregnant women at high risk. The majority of OB/GYNs who reported examining a pregnant woman whom they suspected had influenza did not confirm the diagnosis through laboratory testing. Reasons for not testing for influenza were not explored in this survey but might include cost, unfamiliarity with laboratory testing, lack of availability of the test in the office setting, concern about the estimated low sensitivity of rapid testing (6), lack of familiarity with antiviral medications (e.g., amantadine, rimantadine, and oseltamivir), or the paucity of data on effects of antiviral medications on the fetus. A laboratory diagnosis might improve the identification of influenza on a population level, making physicians aware of the presence of influenza virus in their area and helping them define treatment choices. However, because of the unknown effects of antiviral drugs on pregnant women and their fetuses, these agents are recommended for use during pregnancy only when the potential benefits outweigh the potential risks (2,7). The findings in this report are subject to at least three limitations. First, data were self-reported and are subject to social desirability bias. Second, the response rate was 52%, so results might not be representative of all practicing OB/GYNs. Third, the survey did not assess why physicians did not offer the vaccine in their practices. Finally, physicians were surveyed after the 2003--04 influenza season; therefore, results reflect practice at that time and do not reflect changes that might have occurred in physician practices after the ACIP updated interim influenza vaccination recommendations and during the limited availability of the vaccine for the 2004--05 influenza season. Evaluation efforts are needed to assess knowledge and practices of OB/GYNs since the updated 2004--05 ACIP recommendations, which added recommendations for pregnant women in the first trimester. Pregnant women infected with influenza virus are at risk for serious medical complications that are potentially preventable with influenza vaccination (8). In addition, postpartum vaccination of women is an important means of protecting young infants from influenza, particularly because children <6 months are at high risk for influenza-related complications but cannot be vaccinated themselves (9). CDC and ACOG will continue to monitor influenza vaccine use among pregnant women and the knowledge and practices of OB/GYNs regarding vaccine recommendations. Educational materials for both physicians and pregnant women, such as those that have been successful for other obstetric concerns (10), regarding the risk for influenza complications for pregnant women and children aged <6 months and the use of influenza vaccine for pregnant, postpartum, and breastfeeding women are needed to increase influenza vaccination coverage among these women. In November 2004, the ACOG Committee on Obstetrics Practice published and disseminated to its members a document encouraging use of the ACIP recommendations for vaccination of pregnant women at any stage of pregnancy (7). ACOG recently created a task force on immunizations that will address access to vaccinations in OB/GYN offices. Further research is needed to determine effective strategies for increasing influenza vaccine availability in the obstetrics-gynecology setting. OB/GYNs can play a pivotal role in helping to protect women and newborns from this vaccine-preventable disease. Achieving optimal compliance with current recommendations is important for reducing maternal and infant morbidity from influenza. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/19/2005
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|