Clinical Disease
There are four main clinical forms of smallpox, each with different characteristics. During the smallpox era, the case-fatality rate differed for the different clinical forms, but it was approximately 30% overall in unvaccinated individuals.
Ordinary Smallpox (Variola Major)
Ordinary smallpox was the most common form, accounting for over 85% of all cases during the smallpox era.
See Ordinary Smallpox image below.
Incubation Period
Infection with variola virus begins with an incubation period usually lasting between 10 to 14 days (range 7 to 19 days). During this time, the infected person does not have symptoms, is not contagious, and may feel fine.
Prodrome
The first symptoms of the prodrome begin after the incubation period and include:
- Fever as high as 101°F to 105°F (38.3°C to 40.5°C)
- Malaise
- Prostration
- Headache
- Backache
- Vomiting
- Severe abdominal pain
- Chills
- Anorexia
- Pharyngitis
This phase lasts about 4 days. In pale-skinned patients, an erythematous rash, or rarely, a petechial rash, may be visible.
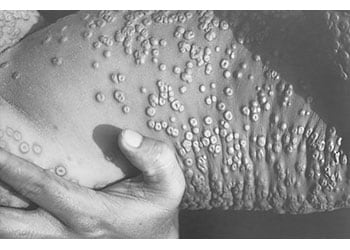
Eruptive Stage
As the fever subsides, rash lesions begin to develop. Lesions usually appear first on the oropharynx, followed by the face and extremities, and then spread to the trunk, palms, and soles in a centrifugal pattern of distribution.
Lesions develop uniformly throughout the disease and progress from macules to papules to vesicles over the course of 4 to 5 days. Within another 1 to 2 days, the vesicles often umbilicate and evolve to pustules that are round, tense, firm to the touch, and deep-seated within the dermis. Lesions typically exhibit the same stage of development in any one area of the body at any given time.
Crusting and scab formation typically begins by the ninth day of exanthema. The crusts slough off around 14 days after rash onset.
See Eruptive Stage image below.
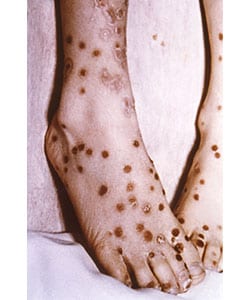
Sequelae
Pockmarks and scarring are the most common sequelae.They are a consequence of virus-mediated necrosis and destruction of sebaceous glands. Scarring may occur all over the body but is most profuse on the face, which has the highest concentration of sebaceous glands.
Other sequelae include:
- Blindness is a rare occurrence and results from corneal scarring following keratitis or corneal ulcerations. Generally, it occurs when malnutrition and/or an opportunistic infection are present.
- Encephalitis
- Osteomyelitis
- Stillbirths and spontaneous abortions
- Infertility (obstructive azoospermia) in males
Recovery from smallpox gives the patient prolonged immunity to re-infection with variola virus. The virus does not persist in the body after recovery.
See Sequelae image below.
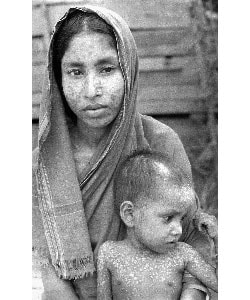
Modified-type Smallpox
Modified-type smallpox occurs in previously vaccinated individuals. In this type, the prodrome stage may still consist of severe headache, backache, and fever, and may last as long as in ordinary type. However, once the skin lesions appear, they generally evolve more quickly, and crusting completes within 10 days as opposed to 14 with ordinary smallpox. There may also be fewer, more superficial lesions than those seen in ordinary smallpox. Patients also do not tend to have a fever during the evolution of the rash.
See Modified-type Smallpox image below.
Flat-type (malignant) Smallpox
Flat-type—or malignant—smallpox is very rare, and is characterized by intense toxemia. It occurs more frequently in children. In contrast to ordinary smallpox, the skin lesions in this type develop slowly, merge together, and remain flat and soft (often described as “velvety” to the touch). They never progress to the pustular stage.
The appearance of the lesions suggests a deficient cellular immune response to variola virus, and the majority of flat-type smallpox cases are fatal. If the patient survives, the lesions gradually disappear without forming scabs. Prior vaccination appears to protect against flat-type smallpox.
See Flat-type (malignant) Smallpox image below.
Hemorrhagic Smallpox
Hemorrhagic-type smallpox occurs among all ages and in both sexes, but is more common in adults. Pregnant women appear to be more susceptible. The underlying biological reasons for this type are unclear. Prior vaccination is not protective. This type is differentiated from ordinary smallpox by:
- Shorter incubation period
- More severe prodromal symptoms with high fever, severe headache, and abdominal pain
- Development of a dusky erythema after illness onset, followed by petechiae and skin and mucosal hemorrhages
Death usually occurs by the 5th or 6th day of the rash, often before characteristic smallpox lesions develop. Death results from a profound toxemia, leading to multi-organ failure.