
Study Syllabus for Classification of Radiographs of Pneumoconioses
Pathology Overview
Pathology Basis of Occupational Lung Disease
Coal Workers’ Pneumoconiosis
Complicated CWP
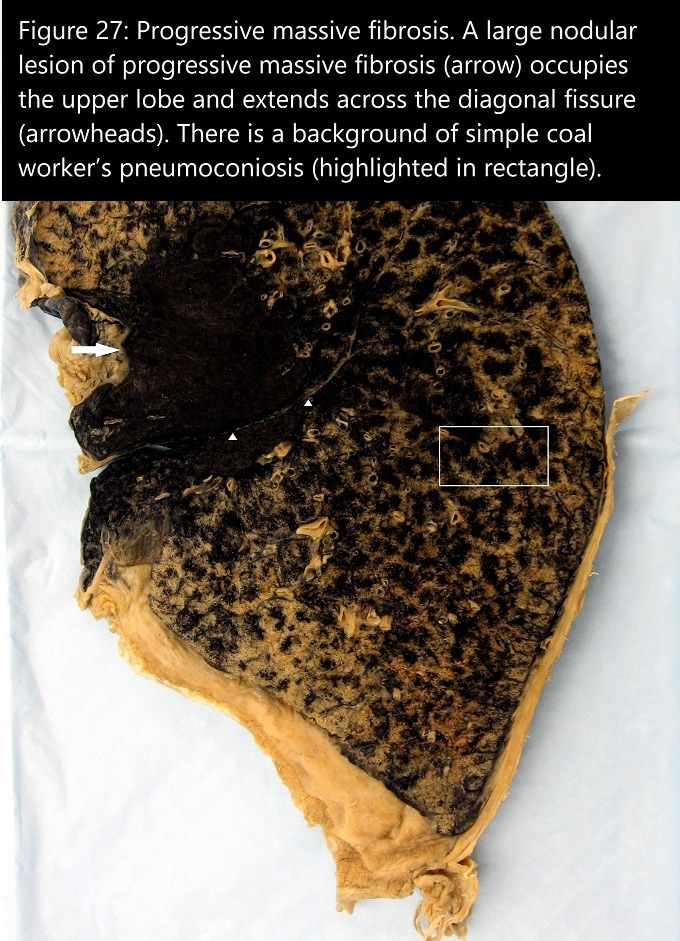
Complicated CWP (PMF) bears similarities to complicated silicosis because of the presence of fibrotic nodules appearing as large opacities of at least 1 cm in diameter in the postero-anterior chest radiograph. The minimum standard for the diagnosis of PMF in lung tissue varies among reports as either 1 or 2 cm in maximal dimension, with the majority of reports advocating a 1-cm tissue standard [“Pathology standards,” 1979; Green and Vallyathan 1998].
Complicated CWP usually occurs in a background of simple CWP, both of which are accentuated in bilateral upper lobes. Macroscopically, lesions of PMF are heavily pigmented, destructive fibrous nodules that may transgress interlobar fissures (Fig. 27). Compared with complicated silicosis, the nodular lesions of PMF tend to have more abundant black pigment, fewer birefringent crystals, and irregular borders. However, with heavy silica exposure, nodules may be more rounded because of coalescence of silicotic-type fibrohyaline nodules. Paracicatricial emphysema with or without bullae commonly surrounds large PMF lesions. Both PMF and complicated silicosis may exhibit central ischemic necrosis and cavitation. Microscopically, PMF lesions are composed of coarse collagen bundles arranged in a haphazard manner, interspersed with black pigment (Fig. 28).
{kind=link}
There has been recent documentation of a severe variant of CWP characterized by accelerated decline in lung function and rapid radiographic CWP progression among US coal miners [Petsonk et al. 2013]. Pathologic findings in a subset of miners with rapidly progressive pneumoconiosis showed PMF in the majority with features of silicosis and mixed-dust lesions, associated with large amounts of birefringent mineral dust particles consistent with silica and silicates. A minority of cases have been characterized pathologically as diffuse interstitial fibrosis [Cohen et al. 2016].
Rheumatoid Pneumoconiosis (Caplan Syndrome)
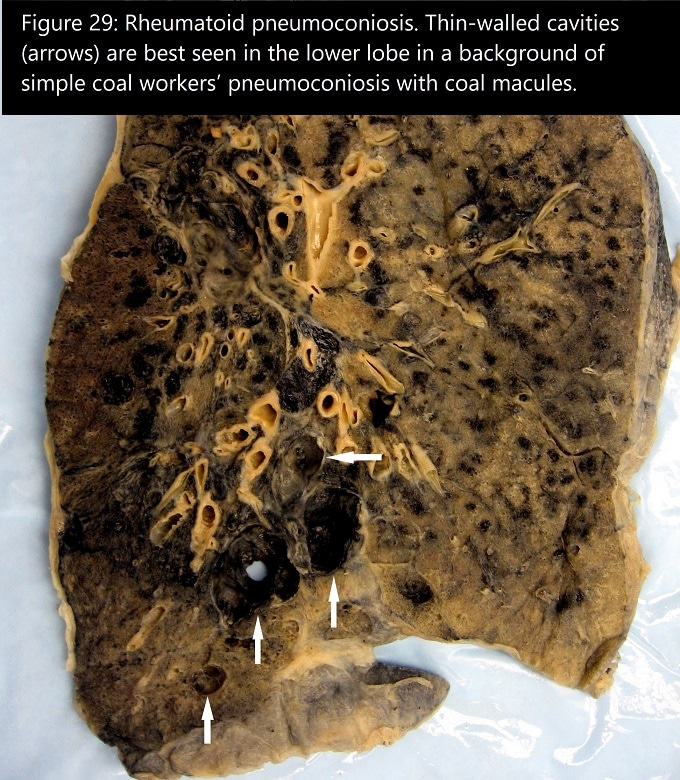
Rheumatoid pneumoconiosis represents a form of pneumoconiosis affecting coal miners (and other mineral dust-exposed individuals) who also have rheumatoid arthritis or serological evidence of rheumatoid factor [Green and Vallyathan 1998]. Rapidly developing nodules of variable size appear macroscopically like giant silicotic nodules, but have a softer texture and often a laminated appearance. Thin-walled cavities like the necrobiotic nodules seen with rheumatoid arthritis may also occur (Fig. 29). Background simple CWP is frequently of a mild degree [Gough et al. 1955]. The histological features of Caplan nodules include laminated black pigment with central necrosis, cavitation, eosinophilic degeneration of collagen, and palisaded histiocytes and/or chronic inflammation around the necrotic zone (Fig. 30). Caplan nodules must be distinguished from mycobacterial lesions. Evaluation for mycobacteria and other infectious organisms is required for any necrotic and/or cavitated lesion of CWP, even when granulomatous inflammation is absent.
{kind=link}