
Two Fire Fighters Die and Eight Fire Fighters are Injured from a Silo Explosion at a Lumber Company - Ohio
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2003-32 Date Released: December 27, 2004
SUMMARY
On October 1, 2003, a 44-year-old male volunteer fire fighter and a 42-year-old male volunteer fire fighter were fatally injured by a silo explosion at a lumber company. The victims responded to a mutual aid call from a neighboring volunteer fire department already on the scene at the silo fire. Prior to the explosion, fire fighters had opened some exterior hatches at the base of an oxygen-limiting silo and were flowing water through the hatch openings with a piercing nozzle. Fire fighters were also flowing water into the top of the silo via an aerial apparatus. At the time of the explosion, one victim was standing on top of the silo and the other victim was in the aerial basket positioned beside the top of the silo. Eight other fire fighters were injured during the explosion, two requiring hospitalization. The fatally injured victims were transported to regional hospitals via ambulance where they were later pronounced dead.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
- Train officers and fire fighters on the hazards associated with different types of silos and the appropriate fire fighting tactics
- Develop and implement standard operating guidelines (SOGs) for fighting oxygen-limiting silo fires
- Ensure that pre-emergency planning is completed for silos within their jurisdictions
Additionally,
- Facilities with oxygen-limiting silos should ensure the proper operation and maintenance of their silos
- Municipalities should consider requiring an exterior placard with specific silo information for use during fire fighting efforts
- Silo manufacturers and research organizations should consider researching the causes and mechanisms of silo fires involving wood products and developing engineering approaches to reduce the risks to fire fighters
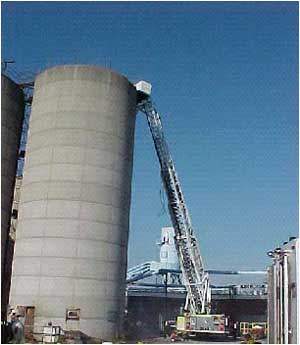
Silo involved in the incident
INTRODUCTION
On October 1, 2003, a 44-year-old male volunteer fire fighter (Victim #1) and a 42-year-old male volunteer fire fighter (Victim #2) were fatally injured by a silo explosion at a lumber company. The victims responded to a mutual aid call for their aerial apparatus from a neighboring volunteer department already on the scene of the silo fire. At the time of the explosion, Victim #1 was standing on top of the silo and Victim #2 was in the aerial basket positioned beside the top of the silo. A third fire fighter (Fire Fighter #1), who was severely injured and hospitalized, was also standing on top of the silo. Seven other fire fighters were injured during the explosion, one requiring hospitalization. On October 1, 2003, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On October 6-7, 2003, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program conducted a site visit at the lumber company and met with representatives of the lumber company and the State Fire Marshal’s Office. The victims’ aerial apparatus damaged in the explosion was also inspected. On December 1-4, 2003, two safety and occupational health specialists conducted further investigation into this incident. The NIOSH team met with the Chiefs of both volunteer departments, interviewed officers and fire fighters on the scene, examined photographs of the fire ground, and reviewed witness statements and other pertinent documents including the State Fire Marshal’s report.
Departments
Two volunteer fire departments were involved in this incident. The incident command department has 23 personnel that serve a population of approximately 2,300 to 2,500 within a rural area of about 45 square miles. The department serves the community from a single station and receives the majority of its funding through the township.
The mutual aid volunteer department has 30 personnel that serve a population of approximately 3,500 within a residential and industrial area of about 17 square miles. The department also serves the community from a single station and receives its funding through the city and township. Both victims were members of this department.
Training and Experience
Victim #1 had 14 years of experience as a volunteer fire fighter. He was certified in the State of Ohio as a Volunteer Fire Fighter Level 1-A. Fire Fighter Level 1-A is a 48-hour course developed for volunteer fire fighters that contains a portion of the requirements for NFPA Fire Fighter Level I. Additional training included confined space rescue, training in propane emergencies, and terrorism awareness.
Victim #2 had 10 years of experience as a volunteer fire fighter. He was also certified in the State of Ohio as a Volunteer Fire Fighter Level 1-A. Additional training included confined space rescue, terrorism awareness, fire fighter safety, farm emergencies, public information officer, and electrical emergencies.
Equipment
The incident command volunteer fire department initial dispatch response listed in order of arrival on the scene included:
- Engine 744 (Officer and four fire fighters)
- Equipment Truck 743 (five fire fighters)
- Engine 745 (two fire fighters)
- Tanker 742 (two fire fighters)
- Chief (Incident Commander) via personally owned vehicle (POV)
- Assistant Chief via POV
- Brush Truck 741 (Officer and fire fighter)
The mutual-aid volunteer fire department 2nd alarm response included:
- Aerial Truck 6642 (Officer, Victim #1, Victim #2, Fire Fighter #1 and two fire fighters)
- Equipment Truck 6643 (four fire fighters)
Additional personnel from both departments arrived on the scene in their POVs.
Structure
The incident silo (see Photo 1) was located at a lumber company that employs 60 full time employees. The facility produces various wood products including hardwood flooring for bowling lanes, architectural millwork, roof trusses and brooms.
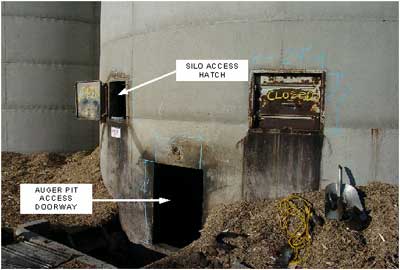
The silo was constructed in 1986 and was used to supply recycled plant material to an electrical boiler. The concrete silo was originally designed as an oxygen-limiting silo but was later modified. The silo was approximately 70 feet high and was 20 feet in diameter. The base of the silo had two doors (one on each side) to access the auger pit (see Photo 2). The auger was used to unload the silo. The silo was normally filled with wood chips and saw dust from the plant. The roof of the silo had two round openings each measuring about 2 feet in diameter. The silo was filled pneumatically as wood chips were blown through a tube into the top of the silo through the center opening. The other opening had a cover that was not in place. On the day of the incident, the silo was filled to a depth of 21 feet with wood chips.
According to the State Fire Marshal’s report, the origin and cause of the fire was heat generated from the friction of a belt on a pulley at the base of the silo’s auger, which ignited the combustible wood chips. The fire smoldered for several hours prior to the arrival of fire fighters. The Fire Marshal concluded that the explosion in this incident was a combination of events that included “at a minimum a backdraft with ignition of the fire gases and a dust explosion of some degree.”
The incident command fire department had conducted annual pre-planning for the facility and routinely made 1-2 calls per year to this facility. These calls included three fires in adjacent silos and small fires in the dust collection system. There were no previous fires in the incident silo.
INVESTIGATION
At 0650 hours, a lumber company supervisor directed a plant employee to check the silo because there was an odor of smoke in the vicinity. The employee went to the silo auger pit and quickly discovered the source of the odor when he opened the access door. The auger pit was filled with light smoke and there was a red glow seen within the silo through the auger port. He quickly exited the pit, shutting the access door on his way out, and reported to his supervisor that the silo was on fire.
At 0657 hours, the lumber company called 911 to report that one of the silos was on fire. At 0701 hours, Engine 744 was en route with an officer and four fire fighters. Engine 744 arrived at the lumber company at 0703 hours. Equipment Truck 743, Engine 745, and Tanker 742 also arrived within two minutes. (Note: The fire station is less than a mile from the lumber company). Upon arrival, fire fighters observed light white smoke coming from the top of the silo and moderate white/gray smoke through the bottom of the access doors. Engine 744 was positioned in the parking lot on the east side of the silo and the crew pulled a 1¾ inch handline to the northeast side of the silo. Engine 745 was put on standby to act as a backup.
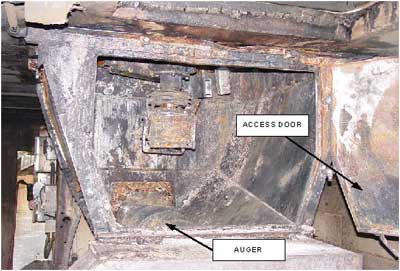
The crews from Engines 744 and 745 entered the silo auger pit from the east. Two fire fighters (with a 1¾ inch handline) inspected the auger pit and found some aerosol cans and a LP gas tank that they removed. Next they shut off the circuit breakers for the electric powered auger motor. The auger access door had warped opened due to heat and water was sprayed into the opening. Two other fire fighters stood on standby on the east side with a charged 1½ inch handline. Conditions within the auger pit were heavy smoke, little visibility and high heat. The metal auger access door (see Photo 3) was glowing red from intense heat and fire fighters were successful in cooling down the metal. Burning wood chips began to fall from the auger access door and pile up on the pit floor.
The IC was concerned that the fire would spread to other areas of the lumber company by burning embers and wanted to aggressively extinguish the fire. The IC wanted to inspect the fire conditions from the top of the silo. Since the silo did not have a cage on the external ladder, he determined that it would be unsafe for fire fighters to climb to the top. At 0725 hours, the IC requested an aerial apparatus (Aerial 6642) as mutual aid from a neighboring volunteer department.
At 0728 hours, Aerial 6642 was en route with an officer and five fire fighters. When the aerial unit arrived at 0736 hours, the crew observed minimal white/gray smoke coming from the top and moderate smoke from the bottom doors of the auger pit. The IC directed the aerial to position next to the silo on the north side. The IC and two mutual aid officers (Note: Another mutual aid officer had previously arrived on scene via POV at 0725 hours) had a brief discussion and decided to extend the aerial to determine the structure of the top of the silo and the conditions within the silo. Both victims from the mutual aid department and another fire fighter from the IC’s department went to the top of the silo in the aerial basket and examined the silo’s condition for several minutes. The basket was brought down and the fire fighters had a conference with the IC and reported that they could not see any flame or the surface of the woodchips within the silo due to the smoke.
At the same time the aerial was at the top of the silo, several fire fighters attempted to unload burning wood chips from the auger pit using shovels and small baskets. Two positive pressure ventilation (PPV) fans were placed on the west side auger pit doors to remove heavy smoke coming from underneath the silo. The fans were blowing smoke out so entry could be made from the east. The manual unloading and use of PPV fans was abandoned after several minutes due to the lack of progress. The auger and other equipment at the base of the silo could not be used to unload the silo since the drive belt had been damaged by fire and the metal was warped from the intense heat. (Note: The electrical supply to the silo’s auger had also previously been shut off).
At 0815 hours, the IC requested Equipment Truck 6643 as mutual aid from the same neighboring volunteer fire department since SCBA air bottles were beginning to run low. Truck 6643 had a cascade system for filling air bottles and arrived on scene at 0824 hours with four fire fighters. Upon arrival, the IC ordered Truck 6643 to park on the east side of the silo in the parking lot.
The IC used a thermal imaging camera (TIC) to locate hot spots on the exterior concrete surface of the silo. Hot spots were identified on the east and west sides about 15 feet from the ground and were beginning to grow in size. The IC decided to flow water into the top of the silo via the aerial. Engine 744 supplied water to the aerial with a 3-inch line and Victim #1, Victim #2 and Fire Fighter #1 went to the top of the silo in the aerial basket. Victim #1 and Fire Fighter #1 exited the basket onto the top of the silo. Victim #2 remained in the basket. Victim #1 made the hose connection to the platform water supply and ran a 50 foot section of 1½ inch hose with a 1½ inch distributing nozzle around the top of the silo. Fire Fighter # 1 lowered the hose into the access hole just as it was being charged. They sprayed water for about 5-10 minutes and it is estimated that less than 1,500 gallons were pumped into the silo.
At the base of the silo, fire fighters had opened a small exterior side hatch. They were pulling wood chips from the hatch and inserting a piercing nozzle supplied by a 1¾ inch handline from Engine 744. The hatch was located below a large hot spot observed with the TIC. A fire fighter was using a pike pole to make a path for the piercing nozzle and another fire fighter was inserting the 10 foot piercing nozzle into the hatch up through the wood chips. A third fire fighter was assisting with the hose. Fire fighters were alternating positions during this operation. Another fire fighter was behind them manning a charged 1¾ inch handline as a backup.
The IC instructed the aerial crew to change the nozzle to a straightbore and spray water in the southeast section of the silo based on the growing hot spots. Victim #2 shut the water off and Fire Fighter #1 started pulling the hose out of the silo. He recalls that the smoke was yellowish and remembers hearing a whooshing sound followed by a loud boom.
At the base of the silo, a sudden burst of wood chips and smoke came out the hatch. This was described by fire fighters as “like a jet engine taking off.” Other fire fighters on scene reported hearing a “sucking” sound or a strange “expanding-like” rush. Fire fighters on the ground closest to the silo felt a concussion and the ground shake. Several fire fighters at the base of the silo near the hatch were thrown to the ground from the force of the blast.
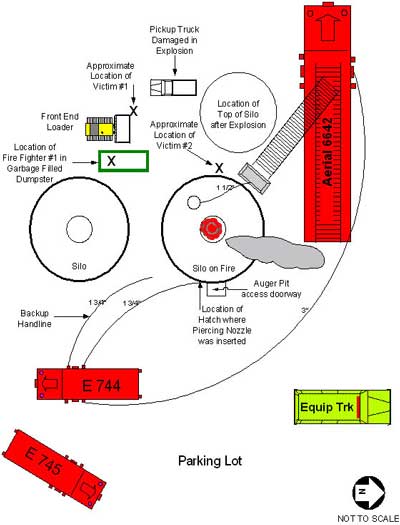
The explosion occurred in the silo at approximately 0850 hours. The top of the silo blew off and landed to the west (see Photo 4 and Diagram). Victim #1, Victim #2 and Fire Fighter #1 were thrown from the top of the silo and aerial basket (see photo 5) and were thrown approximately 70 feet to the ground. Victim #1 was found near the basket of a front end loader parked at the base of the silo. Victim #2 was found at the base of the west side of the silo. Fire Fighter #1 fell into a garbage-filled dumpster which helped break his fall. Debris rained down on the scene, injuring eight fire fighters and two lumber company employees. After the debris had settled, fire fighters recall hearing multiple personal alert safety system (PASS) alarms. The IC ordered an accountability check and radioed for rescue units to come to the scene. Fire fighters on the scene immediately began administering first aid to the injured.
Victim #1 and Victim #2 were transported to regional hospitals via ambulance where they were later pronounced dead. A helicopter transported Fire Fighter #1 and another fire fighter injured by falling debris to a regional trauma center. The incident command department had one fire fighter hospitalized with a broken foot and four fire fighters treated and released from the emergency room. Fire Fighter #1 was hospitalized with a broken arm and leg. Two other fire fighters from the mutual aid department were seen and released in the emergency room. Two plant employees from the lumber company were also hospitalized.
Cause of Death
According to the county medical investigator’s findings, the cause of death for both victims was multiple blunt force injuries.
RECOMMENDATIONS/DISCUSSIONS
Recommendation #1: Fire departments should train officers and fire fighters on the hazards associated with different types of silos and the appropriate fire fighting tactics.
Discussion: In this incident, the critical information that was not established during the initial size-up or determined in their pre-plan was that this silo was a modified oxygen-limiting silo. The IC had successfully fought a silo fire in the past at the lumber company, however that fire had been in a conventional silo. The tactics and strategies used by fire fighters in this incident were for a conventional silo. Since the silo was modified, it should have been treated as an oxygen-limiting silo by fire fighters.
There are two types of upright silos: conventional silos and oxygen-limiting silos or “sealed” silos. Conventional silos are typically used to store corn, hay or other foodstuff for livestock feed. These silos provide for the preservation, storage and disbursement of the feedstock. Conventional silos usually have outside doors stacked up the silo wall. Conventional silos are normally unloaded from the top.
Oxygen-limiting silos are sealed to prevent oxygen from entering the silo. These silos are constructed of steel or concrete and have tightly sealed openings and hatches. When the hatches are closed and the silo is filled, the oxygen concentration should be insufficient to support a fire.
Both types of silos can be found on farms and used at sawmills. It is critical for fire fighters to recognize the type of silo involved prior to beginning any fire fighting operations. In this incident, the silo no longer had tightly sealed top hatches (hence modified oxygen-limiting) and the amount of oxygen entering the silo was sufficient to initiate the explosion.
Recommendation #2: Fire departments should develop and implement standard operating guidelines (SOGs) for fighting oxygen-limiting silo fires.1-3
Discussion: SOGs are a set of written tactical directives that establish a standard course of action on the fireground. SOGs should include such items as fireground safety and guidelines that describe the tactical priorities and related support functions during silo fires. Important elements that should be incorporated into SOGs for conducting operations on an oxygen-limiting silo fire include:
- Confirm pre-plan information on arrival
- Do not direct water or foam onto the fire through the top hatches. This will allow oxygen to enter the silo and can cause a “backdraft-like” explosion of fire gases.
- Do not enter, breach, or open any external silo hatches in an attempt to extinguish the fire.
- If the top hatches are open, fire fighters should not close them if there is smoke coming out from the top, especially if the silo is vibrating or making unusual sounds.
- Lockout and tagout the electrical service to the silo.
- Roof hatches should be safe to close if the silo has been quiet for several days and there has been no smoke coming from the hatches. The hatch should be closed, but not securely, to permit the relief of any pressure that may build up.
- Leave the silo closed for up to three weeks or until the fire consumes all the oxygen in the silo and self-extinguishes.
- Establish a collapse zone around the silo, keep unauthorized personnel away from the area, inspect for extension and protect adjacent exposures.
- Some silos have external valves to inject carbon dioxide or liquid nitrogen from compressed gas cylinders to extinguish the fire.
- If the silo still continues to burn, seek assistance from the silo manufacturer.
Recommendation #3: Fire departments should ensure that pre-emergency planning is completed for silos within their jurisdictions.4-5
Discussion: Pre-emergency planning, pre-planning, and pre-incident planning are all terms that mean essentially the same thing. By first identifying target hazards (oxygen-limiting silos present high risk to life safety and property) within a department’s jurisdiction, the fire department can prioritize and begin to establish pre-emergency plans for those target hazards. Pre-emergency planning enhances effective and safer operations and helps save lives and protect property. The pre-incident plan should not be confused with fire inspections which monitor code compliance. Pre-incident planning assumes an incident will occur and is one of the most valuable tools available for aiding responding fire fighters in effectively controlling an emergency.
In conducting pre-emergency planning for silos, fire departments must recognize the basic silo types as well as the construction features, materials used, presence of loading devices, other distinguishing characteristics, and the hazards associated with each type. In this incident, the silo was not identified as an oxygen-limiting silo in the pre-plan. Pre-emergency planning should identify the type of silo, the age of the silo, silo structural integrity, type of material normally stored in the silo, silo roof structure, and the silo interior layout. Whenever possible, silos should be inspected during the construction phase to aid in assessing the different types of construction, materials, etc. The silo manufacturer should also be consulted to insure that accurate information is obtained. Some silo manufacturers also have step-by-step instructions on how to extinguish fires within their silos.
Additionally,
Recommendation #4: Facilities with oxygen-limiting silos should ensure the proper operation and maintenance of their silos.1-3
Discussion: Silo owners should do the following to prevent fires and explosions in oxygen-limiting silos:
- Conduct proper maintenance of the silo to ensure the integrity of the oxygen-limiting features. The silo manufacturer should be consulted for proper operating and maintenance procedures for their silos. In this incident, the silo was originally built as an oxygen-limited silo but was not operated as such.
- Ensure that oxygen-limiting silos have all hatches closed and sealed when not being filled or emptied. There is little likelihood of a fire occurring since the amount of oxygen would be insufficient to support a fire. In this incident, the top hatches were not being used prior to the fire.
- Routinely inspect and maintain all loading and unloading equipment to ensure safe operation. In this incident, friction from a pulley belt on the unloader auger was the origin and cause of the silo fire.
- Consider installing smoke detectors in the auger pit to provide early warning of smoke and fire.
Recommendation #5: Municipalities should consider requiring an exterior placard with specific silo information for use during fire fighting.1-3
Discussion: Information regarding the type of silo would be invaluable to fire fighters should an incident occur. Placards should be placed on the silo warning fire fighters that the silo is an oxygen-limiting silo, and should include information concerning the proper extinguishing techniques. The placard should also warn fire fighters not to use water to extinguish an oxygen-limiting silo fire and have emergency contact information. The placard should state “DANGER – Sealed Silo – Water Contributes to Explosion of Sealed Silos.”
Recommendation #6: Silo manufacturers and research organizations should consider researching the causes and mechanisms of silo fires involving wood products and developing engineering approaches to reduce the risks to fire fighters.1
Discussion: In this investigation, the State Fire Marshall’s report mentions the role of wood products as a secondary cause of the silo explosion. While a backdraft explosion of the byproducts of combustion is the likely cause of the explosion in this incident, there has been no scientific research on silo fires and explosions with wood products or sawdust. Modeling the dynamics of oxygen-limiting silo fires could result in greater understanding of the engineering controls necessary for prevention. Engineering controls that would reduce the risk to fire fighters could include remotely operated top hatches, so climbing the silo is not required, installing blast panels to reduce the severity of an explosion, and developing a remote system of pre-piped injection ports for silo extinguishment.
REFERENCES
- USFA [1998]. The hazards associated with agricultural silo fires. Emmitsburg, MD: U.S. Department of Homeland Security, Federal Emergency Management Agency, U.S. Fire Administration, USFA Publication No. 096.
- NIOSH [1986]. Preventing fatalities due to fires and explosions in oxygen-limiting silos. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-118.
- NIOSH [1985]. Preventing hazards in the use of water spray (fog) streams to prevent or control ignition of flammable atmospheres. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 85-112.
- Dunn V [1992]. Safety and survival on the fireground. Saddle Brook NJ: Fire Engineering Books and Videos.
- Dunn V [2000]. Command and control of fires and emergencies. Saddle Brook NJ: Fire Engineering Books and Videos.
INVESTIGATOR INFORMATION
This incident was investigated by Steve Berardinelli, Carolyn Guglielmo, and Mark McFall, Occupational Safety and Health Specialists, Division of Safety Research, Surveillance and Field Investigations Branch, NIOSH. A technical review was provided by Ted Halpin, Cornell University.
Photographs AND Diagram

|
|
|

|

|
|
|
Diagram. Aerial view of incident scene after explosion
|
This page was last updated on 12/21/04.