
Construction Laborer Dies from Burns Received when Scalding Hot Water Floods Sewer.
Missouri FACE INVESTIGATION #92MO037
SUMMARY:
A construction laborer died from the thermal burns received when a sewer he was working in flooded with scalding hot water. Upstream a wood and sandbag bulkhead gave away allowing the water to flood the 2.5 by 3.5 foot sewer line where the victim and two co-workers were working. The rush of water washed the men nearly two blocks downstream where they were able to rescue themselves and climb out of the sewer through a manhole. The co-workers suffered 2nd and 3rd degree burns over 30 percent of their bodies and the victim suffered 2nd and 3rd degree burns over 60 percent of his body and survived 26 days. The Missouri Occupational Fatality Assessment and Control Evaluation investigator concluded that, in order to prevent future similar occurrences, employers should:
- use slide gates instead of, or in conjunction with, conventional sewer plugs.
- develop and implement specific confined space entry and work procedures.
INTRODUCTION:
On September 25, 1992, a 29 -year-old male construction laborer died after a wood and sandbag bulkhead gave way and the 2.5 by 3.5 foot sewer line flooded with scalding hot water, burning the victim and two co-workers. The victim died as a result of these burns on October 20, 1992. The MO FACE investigator was notified of the fatality on October 21, 1992.
The employer in this incident is a tunneling and sewer repair contractor who has been in business for 24 years. At the time of the incident there were approximately 103 employees in the company, 80 of which were union laborers. The company employed a full time safety officer who dedicated up to 100 percent of his time to company safety and safety training.
The company contracted with a municipality to repair and line a portion of the city’s sewer system. The employer had been working at the incident site for 22 days and the victim had worked for the company five days and all these days were at the incident site.
INVESTIGATION:
The employer in this incident was contracted to repair a several city-block section of 2.5 by 3.5 foot sewer line. Part of this construction contract was to reinforce the sewer line with steel bands and then line the sewer with a polyvinyl chloride (PVC) type product. In order for the workers to work in the sewer, the normal flow of waste water had to be diverted around the work area. This was accomplished by building a wood and sandbag bulkhead in an upstream 11.5-foot-deep manhole, then pumping the backed-up waste water to a different portion of the sewer system. A six-inch pump was used in the first stages of the project. However, it soon became apparent to the employer the pump was not able to keep up with the cycling waste water discharge from a local industry. A second four-inch pump was then used to compensate for the surges. This setup was maintained through the incident date.
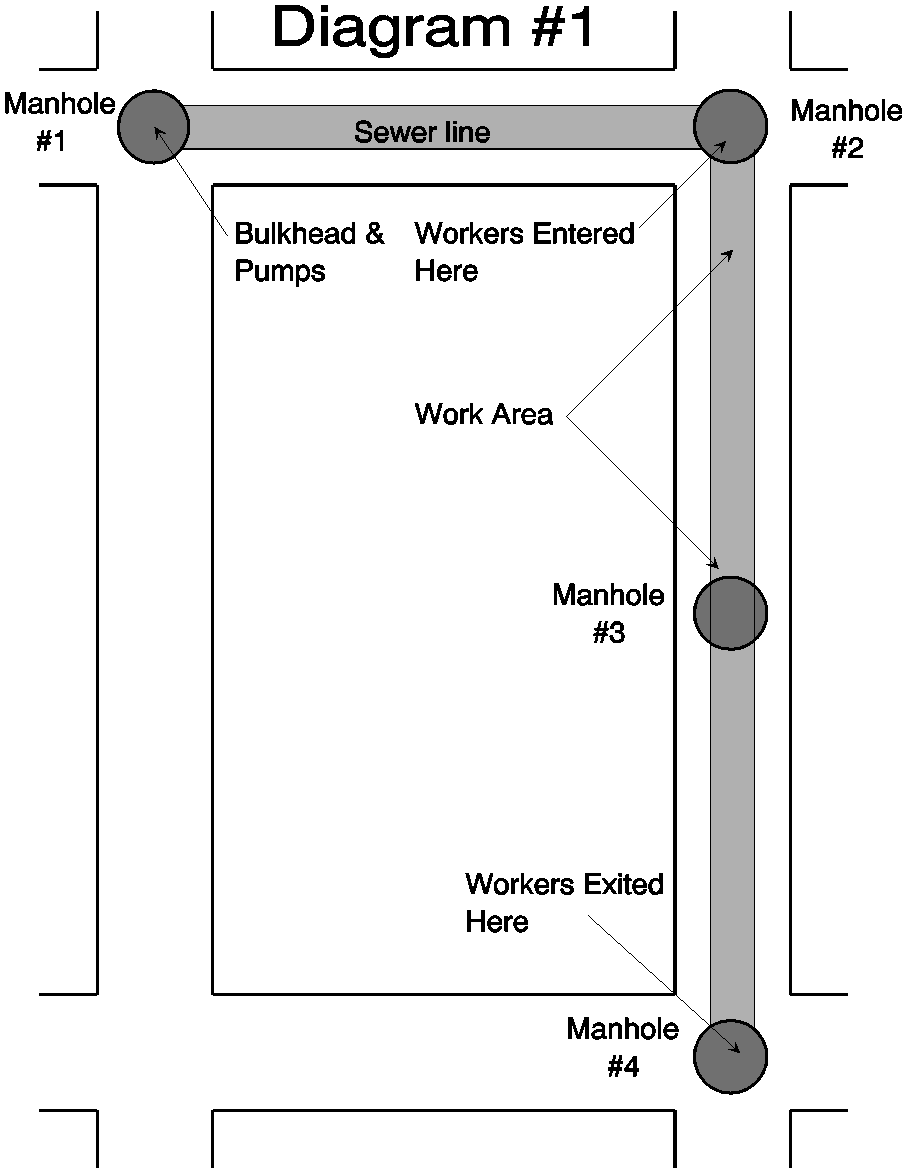
At the end of each work day the workers would tear down an upper section of the bulk head and shut down the pumps to allow the normal flow of water through the system. At the beginning of each workday the pumps, generators and ventilators were started and the project superintendent would rebuild, inspect, and test bulkhead by allowing the water to completely fill the manhole. The air would then be tested and the workers would enter the sewer line by manhole #2 (see Diagram #1)and begin reinforcing the line. The day prior to the incident the project superintendent worked with one of the laborers to go over the rebuilding of the bulkhead in his absence the following day.
On the day of the incident the work began at 7:00 a.m. with seven men on-site; a foreman, operator and five laborers, including the victim. The work to be completed that day consisted of reinforcing the sewer line with rolled steel plates. The operator started the generator, pumps and blowers at the location of the bulkhead. The labor, who worked with the project superintendent the day before, entered manhole #1 to rebuild the bulkhead and isolate the work area downstream. After the bulkhead was rebuilt the victim, the foreman, and a co-worker entered manhole #2 at approximately 7:30 a.m. The foreman proceeded down the line to inspect the sewer and the victim and co-worker began their work. At approximately 7:45 the two other co-workers entered manhole #2. Just as they reached the bottom of the manhole a large surge of scalding water came from upstream and flooded the manhole and the work area pinning them against the manhole. They were able to free themselves and climb out. They immediately and notified the other workers and a security guard to call 911 for emergency help. The security guard called 911 and also notified the ambulance crew of the industry where he worked. The employees proceeded down the street opening manholes in search of the trapped co-workers.
The surge of scalding water washed the victim, co-worker, and foreman nearly two city blocks. The foreman was able to brace himself and catch the two other men and assist them in exiting through manhole #4. By the time the men exited the manhole the ambulance from the nearby industry had arrived, and other rescue personnel arrived soon after. More co-workers from another nearby work-site arrived and assisted the emergency responders. Community ambulances arrived and transported the workers to burn treatment centers. The victim as admitted into intensive care and survived 26 days.
CAUSE OF DEATH:
Organ Failure as a result of Thermal Burns.
RECOMMENDATIONS/DISCUSSION:
Recommendation #1. Where worker entry into sewers is necessary, slide gates should be used instead of, or in conjunction with, conventional sewer plugs.
Discussion: Slide gates provide a more positive method for diverting/controlling the flow of waste water for purposes of maintenance, and should be utilized whenever possible.
Recommendation #2. Employers of sewer maintenance workers should develop and implement a comprehensive confined space entry programs outlined in NIOSH publication 80-106, “Working in Confined Spaces,” and 87-113, “A Guide to Safety in Confined Spaces.”
Discussion: Confined space entry procedures should address each type of confined space that sewer maintenance workers are required to enter (i.e., sewer manholes, sewer mains and lines, diversion chambers, wet wells, lift stations, utility vaults). At a minimum, the following items should be addressed:
- Is entry necessary? Can the assigned task be completed from the outside?
- Has a confined space safe entry permit been issued by the employer before each confined space is entered.
- If entry is to be made, has the air quality in the confined space been tested for safety based on the following criteria:
- Oxygen supply of at least 19.5%
- Flammable range less than 10% of the lowest explosive limit (LEL)
- Absence of toxic air contaminants?
- Are confined spaces posted with warning sign, and are confined space entry procedures posted where they will be noticed by employees and others (e.g. police, rescue personnel)?
- Are workers and supervisors being continually trained in the selection and use of:
- respiratory protection
- test equipment, including calibration and maintenance
- lifelines
- emergency rescue equipment
- protective clothing?
- Have workers been properly trained in working in and around confined spaces?
- Are confined space entry, safe work practices, and rescue procedures discussed in safety meetings?
- Is appropriate ventilation equipment available and/or used before entry and work?
- Is the air quality monitored when the ventilation system is operating?
- Is an outside observer posted and appropriate rescue equipment (safety belt/harness and lifeline) used during every confined space entry?
- Are employees continuously trained in confined space rescue procedures?
REFERENCES:
- National Institute for Occupational Safety and Health, Criteria for a Recommended Standard… Working in Confined Spaces. DHHS (NIOSH) Publication Number 80-106, December 1979.
- National Institute for Occupational Safety and Health, Guide to Safety in Confined Spaces. DHHS (NIOSH) Publication Number 87-113, 1987.
- National Institute for Occupational Safety and Health, Alert – Request for Assistance in Preventing Occupational Fatalities in Confined Spaces. DHHS (NIOSH) Publication Number 86-110, 1979.
- National Institute for Occupational Safety and Health, Safety and Health in Confined Workspaces- for the Construction Industry. DHHS (NIOSH) Publication, 1985.
- National Institute for Occupational Safety and Health, Fatal Accident Circumstances and Epidemiology. FACE-91-17. Public Health Service/CDC/NIOSH/DSR, December 6, 1991.
The Missouri Department of Health, in cooperation with the National Institute for Occupational Safety and Health (NIOSH), is conducting a research project on work-related fatalities in Missouri. The goal of this project, Missouri Occupational Fatality Assessment and Control Evaluation (MO FACE), is to show a measurable reduction in traumatic occupational fatalities in the State of Missouri. This goal will be met by identifying causal and risk factors that contribute to work-related fatalities. The identification of these factors will enable more effective intervention strategies to be developed and implemented by employers and employees. This project does not determine fault or legal liability associated with a fatal incident nor with current regulations. All MO FACE data will be reported to NIOSH for trend analysis on a national basis. This will help NIOSH provide employers with effective recommendations for injury prevention. All personal/company identifiers are removed from all reports sent to NIOSH to protect the confidentiality of those who voluntarily participate with the program.
Please use information listed on the Contact Sheet on the NIOSH FACE web site to contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.