
Worker Dies After Being Pinned Between Wheel And Bed Of Flat-Bed Trailer
MN FACE Investigation 02MN002
Date: August 26, 2002
SUMMARY
A 54-year-old male worker (victim) died when he was crushed between a wheel of a flat-bed trailer and the bed of the trailer. The victim and his brother were working on the dual axle trailer while it was parked on a concrete floor. The front of the trailer was supported by two stands located at the front of the trailer. A payloader equipped with a bucket was used to lift the back end of the trailer. The trailer’s front axle was attached to two leaf springs. The ends of the leaf springs were attached to the trailer’s frame with metal pins. Prior to raising the back end of the trailer, the pins holding the back end of the front axle’s springs were removed. When the back end of the trailer was raised, the front axle swung forward and hung from the pins at the front end of the leaf springs.
After completing the repair work, a chain was hooked to the end of one of the front axle’s leaf spring that was near the floor. The victim was to pull on the chain to swing the front axle toward the rear of the trailer as the payloader bucket was lowered. As the back end of the trailer was being lowered, the chain apparently unhooked from the leaf spring. The victim crouched between the wheels of the trailer to rehook the chain without signaling to his brother to stop lowering the trailer.
While the victim was between the wheels, the trailer suddenly slid forward and the back end fell from the payloader bucket. The victim was pinned between the top of the front axle wheel and the frame/bed of the trailer. After the trailer fell, the victim’s brother exited the payloader and found his brother pinned between the trailer and the wheel. He returned to the payloader and raised the back end of the trailer. After raising it, he removed the victim and laid him on the concrete floor. He placed a call to emergency personnel who arrived shortly after being notified. They examined the victim and pronounced him dead at the scene. MN FACE investigators concluded that, in order to reduce the likelihood of similar occurrences, the following guidelines should be followed:
- workers should only use machines and equipment for tasks for which they were intended and designed; and
- workers should maintain visual contact, either directly or indirectly via other workers, whenever the actions of one worker may directly impact the health and safety of any other coworkers.
INTRODUCTION
On February 20, 2002, the MN FACE program was notified of a work-related fatality that occurred on February 19, 2002. The county sheriff’s department was contacted and a copy of their report of the incident was obtained. On June 8, 2002 an investigation of the incident was conducted by a MN FACE investigator. During the investigation, the victim’s brother who was at the scene at the time of the incident was interviewed and provided detailed information about the incident. During MN FACE investigations, incident information is obtained from a variety of sources such as law enforcement agencies, county coroners and medical examiners, employers, coworkers and family members.
INVESTIGATION
On the day of the incident, the victim and his brother were working on a dual axle flat-bed trailer. The victim’s brother was a self-employed “freight” hauler who used trailers similar to the one associated with this incident to haul large items such as farm equipment for area businesses and local farmers. The victim worked for a local electronics manufacturing company however at the time of the incident he was temporarily laid-off from his position. On the day of the incident, he was helping his brother check, lubricate and replace worn bearings and other components on the axles of the flat-bed trailer.
The trailer was parked on a concrete floor inside a building at an out-of-business lumber yard. The flat-bed trailer had a carrying capacity of about 10,000 pounds per axle. The bed of the trailer was approximately 25-30 feet long and was made of wooden plank secured to a steel frame. Welded to the back end of the trailer frame were two rectangular loops that were approximately ten inches long and extended out beyond the end of the trailer’s frame about 4 to 5 inches.
The trailer was configured with what is commonly referred to as a goose-neck hitch. When towed, the trailer’s goose-neck hitch was connected to a pivot point anchor assembly mounted in the box of a standard pickup. When unhooked, the front of the trailer was held up by two stands located at the front corners of the trailer. The stands were steel tubes that were approximately 5 inches square and several feet long. The stands were locked in a retracted position when the trailer was in use and were extended and locked in a fixed position when the trailer was parked. Attached to the bottom of each stand was a steel pad or foot that prevented the stand from sinking into the ground if the trailer was not parked on a solid floor such as concrete. At the time of the incident the trailer was unhooked from a vehicle and the front end of it was supported by the two stands.
A large industrial payloader equipped with a standard bucket was parked in the vacant lumber yard building. The victim’s brother was familiar with the operation of the payloader and had used it on previous occasions. He drove the payloader toward the back end of the trailer with the bucket lowered to a position below the frame of the trailer. He drove toward the trailer until the bucket was underneath the two rectangular loops that extended from the frame of the trailer. He raised the payloader bucket until it contacted the loops and lifted the trailer until the wheels were off the concrete floor. The back of the trailer was now supported by the payloader bucket while the front end was supported by the two stands at the front of the trailer.
Figure 1 shows the trailer position while it was being worked on by the victim and his brother. The trailer’s front axle was attached to two leaf springs, one adjacent to each wheel of the axle. The ends of the leaf springs were attached with metal pins to the trailer’s steel frame. These pins were worn and were being replaced as part of the maintenance being performed on the trailer. Prior to raising the back end of the trailer, the pins holding the back end of the front axle’s leaf springs were removed. When the back end of the trailer was raised, the front axle swung to the position shown in Figure 1 . This provided the victim and his brother with an unobstructed area between the front and rear axles to work on the trailer’s axles and suspension components.
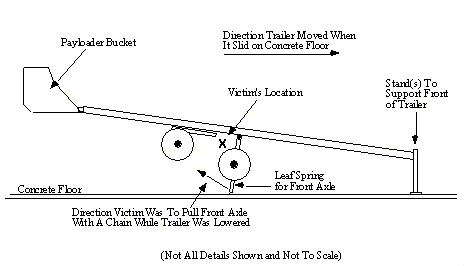
Figure 1. Side view of trailer, back end raised by payloader bucket.
After completing the needed repair work, a chain was hooked to the end of one of the front axle’s leaf spring that was near the concrete floor. The victim was to stand along the side of the trailer and pull on the chain to swing the front axle toward the rear of the trailer as the victim’s brother lowered the bucket of the payloader. The victim’s brother climbed into the cab of the payloader and began to slowly lower the trailer. Due to the size of the bucket, he could not see his brother standing along the side of the trailer. As the back end of the trailer was being lowered, the chain apparently unhooked from the lower end of the leaf spring. The victim crouched between the wheels of the trailer to rehook the chain without signaling to his brother to stop lowering the trailer. As the trailer continued to lower, the ends of the two leaf springs of the front axle contacted the concrete floor. The back of the trailer was no longer supported by the bucket and the trailer was completely supported by the two front stands and the ends of the two leaf springs.
While the victim was between the wheels, the trailer suddenly slid forward and the back end fell allowing the trailer to drop and come to rest on all four wheels and the front end stands. When the axles were in position for use and the trailer was on the ground, the space between the bottom of the trailer bed and the top of the wheels was only 4-5 inches. The victim was pinned between the top of the front axle wheel and the frame/bed of the trailer. After the trailer fell, the victim’s brother called to the victim be did not hear a response. He climbed down from the payloader and walked around to the side of the trailer where he discovered his brother pinned between the trailer and the wheel. He returned to the payloader and raised the back end of the trailer to free the victim. After raising the trailer, he removed the victim and laid him on the concrete floor. He placed a call to emergency personnel who arrived shortly after being notified. They examined the victim and determined that he had died instantly of severe head trauma when the trailer slid forward and fell to the floor.
CAUSE OF DEATH
The cause of death listed on the death certificate was traumatic closed head crush injury.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Workers should only use machines and equipment for tasks for which they were intended and designed.
Discussion: During this incident, an industrial payloader equipped with a front-end bucket was used to left and support the back end of the trailer while various repairs and maintenance tasks were completed. Although the lift capacity of the payloader was in all likelyhood more than adequate to lift and support the trailer, it’s use as a lifting device is not a purpose for which it was intended and designed. In addition, the physical size of the payloader may have contributed to the occurrence of the incident. If the back end of the trailer had been raised using traditional lifting devices such as mechanical or hydraulic jacks, the workers would have been in direct visual contact with each other while the trailer was being lowered. The physical size of the payloader and it’s front-end bucket prevented direct visual contact from being maintained while the trailer was being lowered. If direct visual contact had existed between the two workers while the trailer was lowered, the victim would have been able to notify his brother to stop lowering the trailer for any reason. He also would have been able to notify his brother of the need to position himself under any portion of the trailer for any reason such as re-hooking the chain to the end of the leaf spring. In this case, if the back end of the trailer had been raised using traditional lifting devices, this fatality may have been prevented.
Recommendation #2: Workers should maintain visual contact, either directly or indirectly via other workers, whenever the actions of one worker may directly impact the health and safety of any other coworkers.
Discussion: It is important for workers to never do anything that threatens the safety of themselves or their coworkers at any time or for any reason. In addition, whenever the actions of one or more workers has the potential to impact the health and safety of coworkers, visual contact, either directly or indirectly via other workers should be maintained between workers. In this case, the two workers at the incident site did not have visual contact with each other while the trailer was being lowered. Direct visual contact between the two brothers could have been attained by attaching, either a longer chain, multiple chains or a long rope to the end of the leaf spring. The use of multiple chains or a long rope that would have enable the victim to position himself further from the trailer axle and along the side of the payloader would have allowed the two brothers to be in direct visual contact while the trailer was lowered. Alternatively, indirect visual contact could have been attained through the assistance of a third worker while the trailer was being lowered. If either direct or indirect visual contact had existed between the workers, the victim could have signaled his brother to stop lowering the trailer and to again raise and support it before positioning himself under any portion of the trailer. If direct or indirect visual contact had existed between the victim and his brother, this fatality probably would have been prevented.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.