
Trackman Dies after Being Caught Between a People Mover and a Clip Applicator while Replacing Railroad Ties- Massachusetts
Massachusetts Case Report: 06-MA-024
Release Date: June 22, 2009
Summary
On June 22, 2006, a 36-year-old male trackman was fatally injured while working with a tie gang to replace railroad ties. The victim’s main task as a trackman during this project was to retrieve clips from a clip bag located at the rear of the clip applicator (clipper), and insert the clips into the railroad track’s bracket and tie. The victim was standing in the track behind the clipper by the clip bag when a people mover (bus) that was being operated by a co-worker struck the victim crushing him against the clipper. Co-workers radioed the dispatcher who then placed a call for Emergency Medical Services (EMS). EMS responded to the incident site within minutes along with the transit, municipal, and state police. The victim was transported to a local hospital where he was pronounced dead. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, railroad transportation companies/agencies should:
- Ensure that routinely accessed items, such as clip bags, are not located where roadway workers have to repeatedly foul tracks (position themselves in between or near) to access them;
- Strictly enforce the required ten foot clearance between equipment as well as other regulations established to protect workers;
- Inspect and evaluate all purchased or acquired equipment, especially equipment altered by another entity, to ensure it is safe to operate prior to placing it in operation; and
- Conduct a routine job safety analysis (JSA) for each piece of equipment and the tasks the equipment will be involved in to ensure worker safety.
Introduction
On June 23, 2006, the Massachusetts FACE Program was alerted by the local media that on the day before, a 36-year-old male was fatally injured while replacing railroad ties. An investigation was initiated. On August 22, 2006, the Massachusetts FACE Program Director traveled to the transportation management company’s office and met with two company representatives to discuss the incident. The death certificate, corporate information, police incident report and the Federal Railroad Administration (FRA) documents were reviewed during the course of the investigation.
The employer, a private transportation management company, has a contract to operate a local commuter rail service for a public sector authority. At the time of the incident, the company employed approximately 1,700 people. Of these approximately 1,500 were represented by 14 unions, including the victim. The remaining non-union employees held management job titles. The victim held the job title of trackman for approximately seven years. On the day of the incident, the victim was assigned to be a worker on foot.
The company has a roadway worker protection manual that includes information on track safety procedures. There are designated individuals in charge of safety and health committees for the company’s four main departments – transportation, engineering, mechanical, and customer service. The victim was employed within the engineering department. The FRA is the federal agency responsible for enforcement of employee safety and health regulations in the railroad industry, with some exceptions, such as railroad yards, shops, and associated offices. The company provides employees with initial mandatory training (Roadway Worker Protection Training) required by the FRA and annual eight hour refresher courses. The effectiveness of the trainings is evaluated with written exams.
Investigation
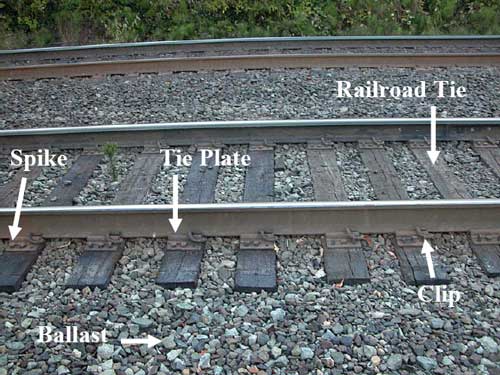
The FRA’s definition of a roadway worker is any employee of a railroad or of a contractor to a railroad.1 The task being performed was railroad tie replacement. The tie gang (work crew) involved in the incident consisted of 40 employees of whom 36 were onsite on the day of the incident. Among these 36 employees, there were 15 trackmen, including the victim, 16 machine operators, two foremen, two mechanics, and one assistant foreman. The railroad ties, which are made of hard wood (Figure 1), are on a schedule to be routinely replaced. Typically during a tie replacement job every third tie is replaced. This tie replacement job was estimated to take one month to complete.
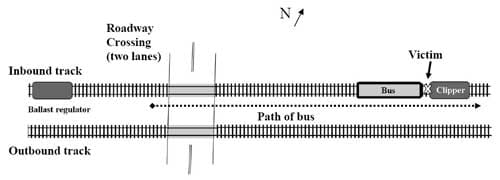
The company reported that typically a tie gang can replace approximately 300 – 600 ties per day and that approximately 41,000 ties are replaced per year. The number of ties replaced depends on the complexity of the section of track and the number of train stations within that section of track. The work location where the incident took place consisted of two sets of tracks that are adjacent to each other and run in the east and west directions. The task of replacing the ties was taking place on the northern most track (Figure 2).
When repair work or other tasks will result in workers fouling the tracks (the placement of workers or equipment in such proximity to tracks that the workers or equipment are at risk of being struck by a train or on-track equipment), these sections of tracks where the workers will be located are placed into a controlled state. Controlled tracks are tracks on which all movement of trains is authorized by a train dispatcher or control operator. Controlled tracks should eliminate train movement on the section of tracks where workers are located. On the day of the incident, both sets of tracks were in a controlled state.
The morning of the incident the tie gang met at 7:30 a.m. in a prearranged location, south of the work site where a daily morning safety meeting and an on-track safety briefing took place. Then all 35 employees were transported to the work site. The weather was clear, with some sun and a brief shower around noon. The section of track where the ties were being replaced was controlled starting at 9:00 a.m., after the peak travel time for the morning commuter trains. Once the tracks were controlled, the gang had a set amount of time to complete their daily tasks. On this particular day, the track was scheduled to be back in service at 4:00 p.m. for the peak travel time of the night commuter trains. This meant that the gang would have to finish their task at 3:30 p.m., which would give them one half hour to get all of the gang members and equipment back to the starting location.
This tie replacement task involved 15 pieces of on-track equipment and operators that work in a manner similar to an assembly line. After the morning safety meeting and on-track safety briefing, the assistant foreman and several of the trackmen headed out to the work location first. Once at the work location, the foreman started to mark the railroad ties to be replaced, approximately every third tie, and the trackmen then started pulling spikes from the marked ties (Figure 1). The 15 separate pieces of on-track equipment were positioned on the track in the sequence that they were to be used during the replacement process and were then driven by the machine operators out to the work location in this sequence. The third to last piece of equipment to head out to the worksite was a clipper followed by a people mover (bus) and the last piece of equipment was a ballast regulator. Ballast is gravel that is used around the tracks and ties (Figure 1). The ballast regulator’s function is to sweep the ballast out of the shoulder area of the track area before the tie is removed and then sweeps the ballast back once a new tie is replaced.
The two pieces of equipment directly involved in the incident were the clipper and bus. The clipper (Figure 3) was manufactured in 1985 and is equipped with steel wheels. At the rear of the clipper there are two signs warning other equipment and workers on foot to keep ten feet away. The main function of the clipper is to tighten/squeeze the clips once they are set in place on the tie plates (Figure 1). These clips fasten the track to the tie plate. One machine operator and four trackmen are typically assigned to the clipper, and this was the case on the day of the incident. The four trackmen, including the victim, were workers on foot and their main task was to put clips into place on the tie plates for the clipper to tighten.
The bus (Figure 4), which was originally manufactured in 1981 as a tie mover, was converted in 1997 to a bus by the company that had previously operated the commuter rail. The bus is used to transport both supplies and tie gang members who are not assigned to operate equipment to the work location when the work location is a distance from access roads. When needed, the bus is also used to pull a tool trailer. The bus is rectangular in shape and has steel wheels that are for on-track use only. Top speed for the bus is approximately 30 miles per hour, and the bus has a pneumatic breaking system. The front and rear of the bus have large plastic windows and the sides of the bus are open. The main part of the bus has seating for workers that face perpendicular to the movement of the bus, therefore when the workers are seated they are facing and looking out the sides of the bus. The operator’s area is located at the front of the bus and the operator’s seat faces the left side of the bus. When the operator is seated in the operator’s seat, the operator is looking out to the left side of the bus. To look through the windshield of the bus, the operator’s head has to be turned 90 degrees to the right (Figure 4).
On the day of the incident, the bus was pulling a tool trailer that weighed approximately 8,000 pounds. The bus operator, a senior operator with over 20 years of experience, was also in charge of operating the ballast regulator. The bus operator’s task included moving the bus in the forward direction when the clipper, the piece of equipment in front of it, had moved far enough ahead. After pulling the bus up to the clipper, the bus operator would then walk back to the ballast regulator, the last piece of equipment on the tracks, and move it forward to the bus while sweeping the ballast back within the track area. This activity occurred multiple times throughout the day.
The incident occurred just after 3:00 p.m. with approximately 60 ties left to replace that day. The ballast regulator was the only piece of equipment that had not yet been moved in the forward direction, easterly, across a motor vehicle roadway crossing located approximately 300 feet to the west of the incident location. At the time of the incident, the bus operator was in the process of moving the bus forward to bring it in line with the rest of the equipment, behind the clipper. The clipper was not moving and the clipper operator was in the operator’s seat.
As the bus approached the clipper, the victim fouled when he entered the track’s gauge, the location between a track’s two rails, to retrieve a clip from the clip bag located at the rear of the clipper. It was reported that about the same time, the bus operator applied the bus’s brakes and that the bus started to skid along the tracks. It was also reported that the bus operator then cut the bus’s throttle and released the air in the bus’s air tank in an attempt to stop the bus. As the bus skidded towards the clipper, the victim was still standing in the track’s gauge behind the clipper with his back to the bus. The bus then struck the victim and the rear of the clipper crushing the victim between the two pieces of equipment and resulting in the two pieces of equipment to become jammed together. During the impact, the clipper was pushed forward five feet. At this same time the three other workers on foot assigned to the clipper were standing in front of the clipper and jumped out of the way as it was pushed forward when impacted by the bus.
Co-workers radioed the dispatcher who then placed a call for emergency medial services (EMS). The co-workers had to use track jacks to separate the two pieces of equipment and free the victim. Once the victim was freed, co-workers attended to him. When EMS arrived at the incident location, the victim was transported to a waiting ambulance and then transported to a local hospital where he was pronounced dead. Transit, local and state police also arrived at the incident location within minutes.
After the incident, an engineer employed by the commuter railroad examined and tested the bus and its braking system and concluded that the bus’s braking system was in working order. The results of the tests showed that when the bus is moving approximately 10 to 12 miles per hour the bus would skid 26 feet before coming to a complete stop. It was reported that at the time of the incident there was oil present on the track, which was also reported as a typical occurrence. The oil would most likely come from the 15 pieces of equipment used during the tie replacement which had passed over this section of track prior to the bus. In addition, it was reported that the bus’s horn was not sounded prior to impact because the operator could not find the location of the horn’s switch. The bus’s horn was tested by the same engineer and found to be working properly.
Cause of Death
The medical examiner listed the cause of death as exsanguination due to laceration of popliteal vessels.
Recommendations/Discussion
Recommendation #1: Railroad transportation companies/agencies should ensure that routinely accessed items, such as clip bags, are not located where roadway workers have to repeatedly foul tracks (position themselves in between or near) to access them.
Discussion: The Federal Railroad Administration (FRA) standard 49 CFR 214.313 Railroad Workplace Safety states that “A roadway worker shall not foul a track except when necessary for the performance of duty.” In this case, one of the victim’s main tasks was to manually set clips into the tie plates. The storage location for the clips was in a bag located at the rear of the clipper. When trackmen needed to retrieve clips to continue their task, they had to access the clip bag located at the rear of the clipper, therefore fouling the track. To help minimize the number of times workers need to foul tracks, the single rear clip bag should be replaced with two clip bags, one located on each side of the clipper.
Recommendation #2: Railroad transportation companies/agencies should strictly enforce the required ten foot clearance between equipment as well as other regulations established to protect workers.
Discussion: The FRA standard 49 CFR 214 Railroad Workplace Safety states (Subpart C – Roadway Worker Protection) that each roadway worker is responsible for following the on-track safety rules of the railroad upon which the roadway worker is located.1 In this case, Rule Number 341(d) in the company’s Roadway Worker Protection Manual states that when two or more pieces of equipment are being used together, operators must maintain a ten foot clearance between them unless otherwise instructed by the employee in charge. It also states that while equipment is in working mode, roadway workers must stay ten feet from its working area unless otherwise specified by the operator (Rule Number 341(e)). In this case, it appears that these regulations were not strictly enforced. If the ten foot rule for both equipment and roadway workers had been strictly enforced, the probability of this incident occurring would have been minimized.
Recommendation #3: Railroad transportation companies/agencies should inspect and evaluate all purchased or acquired equipment, especially equipment altered by another entity, to ensure it is safe to operate prior to placing it in operation.
Discussion: The bus had been originally manufactured as a tie mover and was converted by the previous manager of the commuter railroad into a bus. When the current company took over the management of the commuter railroad, the bus was one of many pieces of equipment that was available for the company to use.
When purchasing or acquiring equipment, especially equipment that has been altered by an entity other than the original manufacturer, the equipment should be thoroughly inspected and evaluated to ensure that all aspects of the equipment are safe to operate. In this case when seated in the bus operator’s seat, the operator faces the side of the bus. When operating the bus, the operator has to turn their head 90 degrees to look in the direction that the bus is moving.
Recommendation #4: Railroad transportation companies/agencies should conduct a routine job safety analysis (JSA) for each piece of equipment and the tasks the equipment will be involved in to ensure worker safety.
Discussion: A job safety analysis (JSA) is a technique to systematically evaluate job tasks and how to perform these tasks safely. It involves identifying all potential hazards and hazardous situations that could occur when performing tasks by focusing on the relationship between the worker, the task, the tools and the work environment.2 JSAs should be routinely performed to identify uncontrolled hazards by breaking down the operation of the equipment and the tasks to be performed into steps. Each step should be evaluated to identify the hazards or potential hazards. Once hazards are identified, employers should take steps to eliminate or control these hazards. In this case, a JSA might have identified that the workers on foot who were assigned to the clipper fouled the track which placed them in the tracks gauge every time they went to retrieve clips, and led to changing the location of the clip bag (Recommendation # 1).
References
- Code of Federal Regulations, 49 CFR 214 (b)(4) Railroad workplace safety, Government Printing Office.
- DOL. OSHA. Job Hazard Analysis.pdf iconexternal icon Publication Number: 3071. [www.osha.gov/Publications/osha3071.pdf]. Date accessed: February 13, 2008.
- Northeast Operating Rules Advisory Committee. NORAC Operating Rules, 8th Edition.
|
|

|
|
Figure 3 – Clipper involved in the incident |
 |
|
Figure 4 – Operator’s area of the bus involved in the incident |
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.