
Vibratory Hammer Operator Killed when Crushed Between a Crane Superstructure and its Left Rear Track
Massachusetts Case Report: 03-MA-006-01
Release Date: January 26, 2005
Summary
On March 24, 2003, a 57-year-old male vibratory hammer operator (the victim) was fatally injured when he was crushed between a crane superstructure and its left rear track on a construction site. The crew had been on site to install steel sheet pilings. There had been an extended delay in the steel sheet piling installation task due to an obstruction in the ground. During the installation delay, the victim entered the crane’s swing radius and was crushed when the crane operator moved the crane and swung the superstructure without advanced notice. An onsite worker and a Massachusetts State trooper, who was passing by the construction site, discovered the victim. The trooper stopped and placed a call for help. Emergency Medical Services (EMS) personnel arrived within minutes of the call, and the victim was pronounced dead at the incident site. The Massachusetts FACE Program concluded that, to prevent similar occurrences in the future, employers should:
- ensure that the swing radius of each crane has been barricaded to prevent employees from entering the swing radius
- store all tools that are needed by workers, other than the crane operator, outside of the crane’s swing radius
- ensure crane and/or superstructure movement occurs only when an “all clear” signal is given to the operator
- brief workers prior to beginning unscheduled tasks to discuss what tasks each worker will be performing
- consider the use of electronic devices or sensors to warn equipment operators of workers on foot in the immediate work area
Introduction
On March 25, 2003, the Massachusetts FACE Program was notified by the Occupational Safety and Health Administration (OSHA) through the 24-hour Occupational Fatality Hotline, that on March 24, 2003, a 57-year-old male construction worker was fatally injured when he was crushed by a crane. An investigation was immediately initiated. On March 27, 2003 the Massachusetts FACE Program Director and a co-worker traveled to the office location where the company’s general manager was interviewed. The police report, death certificate, corporate information, and OSHA fatality/catastrophe report were reviewed during the course of the investigation.
The incident company was a general and marine contracting construction firm and had been in business approximately 56 years at the time of the incident. Depending on the time of year and current projects, the number of employees ranged from four to twenty-five. During the winter season was when the company would have approximately four employees, all office workers. The work crews were represented by unions and typically consisted of seven workers per job, hired through the union halls.
The day of the incident, the seven crew members on site included a crane operator, a vibratory hammer operator (the victim), a pile driver foreman, and four pile drivers. The victim and the crane operator each had approximately 23 years of work experience. The incident company had developed an employee safety manual that was provided to workers, but the company did not provide health and safety training. Workers received training through union apprenticeships, provided by the unions. The project’s general contractor held weekly “toolbox talks”.
Investigation
The incident company had been subcontracted to install steel sheet pilings and pipe pilings as part of a larger construction project. The company’s first day on site was February 10, 2003 and the incident occurred six weeks later. The victim had been working full-time at the incident site for these six weeks installing the steel sheet piling, which would act as an earth support so that excavation could eventually be performed.
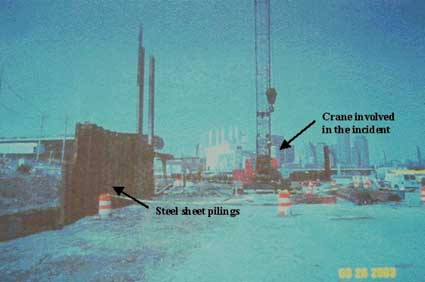
The crane involved in the incident was a 70-ton lattice boom crawler, manufactured in 1975. The company had purchased the crane approximately one year prior to the incident. A vibratory hammer rigged to the crane was being used to install the steel sheet pilings (Figure 1). The vibratory hammer was powered by a power pack, which consisted of a diesel engine that provided the energy required by the hydraulic motors and hammer clamps.
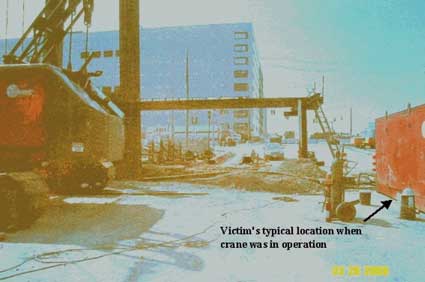
The hammer section (top section) of the vibratory hammer connects to the crane’s hook and the clamp section (bottom section) of the vibratory hammer attaches to the steel sheet pilings. A vibratory force is created in the steel sheeting by two counter rotating weights within the hammer section of the vibratory hammer. The vibratory force displaces the soil around the steel sheet piling allowing it to be driven down into the soil. When the vibration is stopped the soil returns to its former load bearing condition. The victim’s main task was to operate the vibratory hammer’s hand held controls, mainly turning the vibratory hammer on and off. The victim’s typical location during the steel sheet pile driving task was next to the power pack and outside of the crane’s swing radius (Figure 2).
The day before the incident, the crew was installing steel sheet piling and the last sheet of the day had struck an obstruction, which prevented it from being driven to the desired depth. On the day of the incident, the crew arrived at the work site at approximately 7:00 a.m. and attempted to finish driving the steel sheet piling that they started installing the day before. Because they could not get the steel sheet piling to go past the obstruction, the operation was stopped again. The general contractor of the project brought in excavation equipment to remove the obstruction, but was unsuccessful. During the general contractor’s attempt to remove the obstruction, the pile driving crew’s downtime led into their scheduled work break. The crane operator spent the downtime and the coffee break inside his truck, and the victim spent this time in his car.
The incident occurred at approximately 9:30 a.m., immediately following the coffee break, when the crew started an unscheduled task because the steel sheet pile driving task was still on hold. The unscheduled task was welding together the already driven sheets. The welding task was not part of the victim’s nor the crane operator’s job duties, and while the rest of the crew was performing the welding task, the victim and crane operator had additional downtime. During this downtime, the victim walked over to the crane, which did not have a swing radius barricade around the rear of the rotating superstructure. While standing inside the crane’s swing radius, between the left rear track and the crane superstructure, the victim was out of the crane operator’s line of sight. Without advance warning, the operator moved the crane and swung the superstructure to the right crushing the victim between the left rear track and the superstructure (Figure 3).
The employer reported that it is not known why the crane operator moved the crane and swung the superstructure at that time, but it could have been to reposition the crane to get it ready for when the steel sheet pile driving task could be resumed. In addition, the company stated that the victim might have accessed the swing radius location also to prepare for resuming the steel sheet pile driving task by retrieving a grease gun to grease the hammer. The task of greasing the hammer is typically performed once every two days. The grease gun for this task was stored in the engine compartment at the back of the crane, which is inside the swing radius.
The victim was discovered by an on site pile driver and a Massachusetts State trooper who was passing by the construction site. The trooper stopped and placed a call for help. Emergency Medical Services (EMS) personnel arrived within minutes of the call and the victim was pronounced dead at the incident site.
Cause of Death
The medical examiner listed the cause of death as multiple injuries, severe.
Recommendations/Discussion
Recommendation #1: Employers should ensure that the swing radius of each crane has been barricaded to prevent employees from entering the swing radius.
Discussion: The OSHA standard 29 CFR 1926.550, Cranes and derricks, specifically states “accessible areas within the swing radius of the rear of the rotating superstructure of the crane, either permanently or temporarily mounted, shall be barricaded in such a manner as to prevent an employee from being struck or crushed by the crane.”
In this case, the rear swing radius of the crane’s superstructure was not barricaded. A barricade, either temporary, such as three-inch caution tape, or permanent, such as cement barriers, will help prevent employees from accessing the swing radius and being struck or crushed by the crane. In addition, no one, including vibratory hammer operators and oilers, should ever enter a crane’s work area without notifying the crane operator.
Recommendation #2: Employers should store all tools that are needed by workers, other than the crane operator, outside of the crane’s swing radius.
Discussion: It was stated that the victim might have entered the crane’s swing radius to retrieve a grease gun, which was stored in an engine compartment, in order to grease the hammer. The task of greasing the hammer typically occurred once every two days. Storing the grease gun in a location outside of the crane’s swing radius would have limited the number of times the victim needed to access this area and might have prevented this incident. In addition, there could be scheduled times to perform routine preventive maintenance tasks such as greasing the hammer.
Recommendation #3: Employers should ensure crane and/or superstructure movement occurs only when an “all clear” signal is given to the operator.
Discussion: In this case, the crane operator, while located in the crane’s cab, had very limited visibility around the crane’s perimeter. Crane operators should wait for an “all clear” signal each time before they move the crane. If the operator is making an unplanned move, the signal person should be notified, and the operator should hold off from moving the crane until he has received the “all clear” signal. These signals can include, but are not limited to, hand signals and direct verbal contact, via a radio system, which might have been able to prevent this incident.
When hand signals are used, only one trained signal person should be designated to give signals to the operator. Hand signals should only be used when the operator and signal person have a clear and unobstructed view between their locations. When verbal contact via a radio system is being used, workers could notify crane operators prior to entering the swing radius. A radio system could include a mounted radio inside the crane cab and a handheld or wireless headset for the worker.
Recommendation #4: Employers should brief workers prior to beginning unscheduled tasks to discuss what tasks each worker will be performing.
Discussion: In this case, an obstruction was hit during the sheet driving task, resulting in unscheduled downtime for the crew, which led into the crew’s scheduled work break. After the scheduled work break, the pile driving crew started the unscheduled task of welding together the already driven sheets instead of continuing the originally planned sheet driving task. Both the victim and the crane operator did not have assigned tasks as part of the welding process and their unscheduled downtime continued.
Immediately prior to the incident, it appeared that both the victim and the crane operator were performing self-assigned tasks to keep themselves busy until the sheet driving task could be resumed. Briefing workers prior to performing unscheduled tasks to discuss the tasks might have alerted the crane operator that the victim planned to access the swing radius of the superstructure to retrieve the grease gun.
Recommendation #5: Employers should consider the use of electronic devices or sensors to warn equipment operators of workers on foot in the immediate work area.
Discussion: Workers on construction sites often work in close proximity to moving heavy equipment. Technology, such as video cameras and fiber optic systems are available and could be installed on construction equipment. This type of equipment could give the operator an unobstructed view of the area around the rear of the vehicle. Other available devices can detect the presence of persons in the blind spots of equipment and provide a warning to the operator. One example of this type of device is radio frequency identification (RFID) tags and tag readers. With the RFID system, each worker on foot wears a RFID tag and a tag reader is mounted on the equipment. When a tag reader senses a tag, an alarm is triggered warning the equipment operator.
References
- Code of Federal Regulations, 29 CFR 1926.550 Cranes and derricks, Government Printing Office.
- Code of Massachusetts Regulations, 520 CMR 6.00 Hoisting machinery, Massachusetts Department of Public Safety.
- NIOSH 1998. Program for mining research, navigation and warning aides for mobile equipment, U.S. Department of Health and Human Services, Public Health Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 98-114.
- NIOSH web site: https://www.cdc.gov/niosh/mining/works/coversheet296.html. NIOSH 2000. Test results of collision warning systems for surface mining dump trucks. U.S. Department of Health and Human Services, Public Health Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) RI 9652. (Link updated 3/20/2013)
Illustrations
 |
|
Figure 1 – Crane involved in the incident and some driven sheet pilings.
|
 |
|
Figure 2 – Victim’s typical work location during the crane operation.
|
 |
|
Figure 3 – Location where victim was crushed, between the left rear track and the superstructure.
|
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.