
Laborer Falls 48 Feet to His Death While Painting Inside of Empty Storage Silo
Indiana FACE Investigation 96IN123
SUMMARY
On September 20, 1996, a 28-year-old male laborer/painter (the victim) fell nearly 48 feet to his death while painting the inside of a storage silo. The 48-foot silo, empty at the time of the fatal incident, is normally used to store tiny plastic pellets used in the manufacturing of plastic soda bottles. It had previously had been sandblasted in preparation for painting. The interior of the silo is accessed by ascending an enclosed fixed ladder system on the outside and entering through a 20-inch opening in the top.
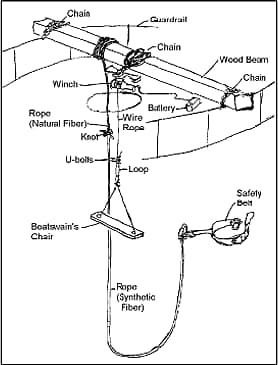
Figure 1. Boatswain’s chair and safety line showing attachments at top of silo.
The victim worked for a three-employee construction company which was sub-contracted to paint the inside of the silo. On September 20, 1996, all three began work on this job at about 8:30 A.M. First they mixed two different kinds of epoxy paint in a five-gallon bucket to get the right texture required for the inside of the silo. A co-worker then hauled the 5 gallon bucket to the top of the storage silo by means of a rope. This co-worker remained outside on top of the silo. The victim entered the 20″ opening and sat in a makeshift boatswain’s chair. (See Figure 1) The chair was a substandard 21″ x 5½” in size and was supported by a 3/8″ plastic coated cable (Figure 2). The working end of the plastic coated cable was attached to the boatswain’s chair support cable by two U-bolts and duct tape. The chair was lowered and raised by an electric winch powered by a large battery and a portable generator. Vise grips were used to connect the power cables to the battery.
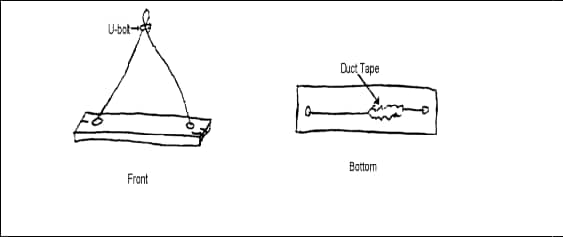
Figure 2. Boatswain’s chair.
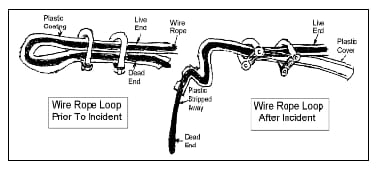
Figure 3. Loop in winch line before and after incident.
The electric winch was secured to a 6″x 6″ wood beam (not man tested) on top of the storage silo. This support timber was secured to the top of the storage silo frame by a length of chain wrapped around each end. The winch was secured upside down with a heavy chain wrapped around the support timber.
When the victim entered the silo on September 20, he was wearing an old safety belt 52″ x 4½” with a safety rope secured to a 10″ x 4½” triangular lock ring that was frozen in the open position. The safety line was made up of two different sizes, types, and lengths of rope tied together and secured to the 6″x 6″ timber on top of the storage silo.
The co-worker on top of the storage silo stated that around 2:00 p.m., when they were ending their day, he started the winch to bring the victim up to the 20″ opening in the top of the tank. The victim was near the top of the silo when the co-worker heard something snap but was not sure what it was. The next thing the co-worker knew, the victim and safety rope were plummeting 48 feet to the bottom of the silo. Investigation after the event revealed that the end of the winch line secured to the boatswain’s chair had pulled out of the improperly positioned U-bolts Figure 3) allowing the victim to fall.
A computer printout run sheet shows that the local fire department was called at 14:06 and arrived on the scene at 14:11. After local fire personnel used a fan to clear out hazardous paint fumes in the bottom of the tank, an advanced EMT-firefighter verified that the victim’s vital signs were non-existent. Because the local fire department did not have a confined space rescue team, it was necessary to call a department from a neighboring county to extricate the victim’s body.
The confined space rescue team initially thought the safety rope had broken but found it still tied to the victim with eight to ten feet of slack. The safety rope, comprised of two lengths and sizes, measured 83′ 3″. Evidence indicates the victim fell just under 48 feet. These facts make it clear that the victim’s life could not have been saved with the PPE he was wearing at the time of the fatal incident.
The FACE investigator concluded that, in order to prevent similar incidents, employers and employees involved in work at elevations should:
- Ensure that a boatswain’s chair seat is of at least minimum dimensions and properly reinforced on the underneath side by cleats and that it is properly secured to an adequate suspension system.
- Perform a hazard evaluation at each work site before any work is initiated.
- Train employees in the recognition of hazardous work conditions and provide methods to control such hazards, including the use of appropriate PPE for fall protection.
INVESTIGATION:
This FACE investigation was prompted by a phone call from the county coroner reporting the incident and requesting an investigation be conducted. The FACE investigator met with the county coroner and the sheriff’s department crime laboratory technician the same day. Pictures and measurements were taken of the PPE which the victim had used, and statements were taken. The FACE investigator visited the scene of the incident the same day. The next day the FACE investigator met with the IOSHA compliance officer and members of the local fire department that responded to the call. Four fire fighters were interviewed.
The employer involved in the incident was subcontracted by a larger contractor to paint the inside of two storage silos. The subcontractor has been in business for three years and employs three workers. There were no written safety procedures or on-the-job safety training. This was the subcontractor’s first fatality.
CAUSE OF DEATH:
The cause of death as reported on the Indiana certificate of death is Blunt deceleration trauma.
RECOMMENDATIONS AND DISCUSSION
Recommendation #1: Ensure the boatswain’s chair seat used to sit on while painting the inside of the storage silo is of at least minimum dimensions, reinforced by cleats, and properly suspended.
DISCUSSION: In this incident the boatswain’s chair seat was less than the minimum dimensions of 12″ x 24″ x 1″ thick and was not reinforced with cleats to prevent the board from splitting. Furthermore, the “U”- bolts used to secure the loop in the wire rope which was supporting the boatswain’s chair were installed backwards such that they were not contacting the dead end of the wire rope. This improper arrangement allowed the dead end to slip out causing the boatswain’s chair to fall.
Recommendation # 2: Employers should perform a hazard evaluation at each work site before any work is initiated.
DISCUSSION: The employer should identify all potential hazards at a work site. Each specific job involves hazards particular to that job or working environment. A jobsite and/or hazard analysis survey in this incident would have determined workers would be working at elevation and adequate fall protection would be necessary.
RECOMMENDATION #3: Employers should train employees in the recognition of hazardous work conditions and provide methods to control such hazards, including the proper use of appropriate fall protection equipment.
DISCUSSION: Employers are required by OSHA reg. 29 CFR 1926.21 (b) (2) to instruct each employee in the recognition and avoidance of unsafe conditions, and to control or eliminate any hazards or other exposures to illness or injury. In this incident the fall protection equipment used for this work task was inadequate and contributed to the fatal incident. The safety belt lanyard (rope) worn by the victim was of a length that would allow a fall much greater than the standard 6 feet. This lanyard, which consisted of two different types and lengths of rope knotted together, measured 83.3 feet and was set up such that the victim fell the full height of the storage silo (48 feet) when the boatswain’s chair he was using broke loose from its support cable. Furthermore, the victim was working 48 feet high inside the storage silo and did not have a lifeline attached to the structure independent of the rigging.
According to the General Duty Clause of the Occupational Safety and Health Act (section 5 (a) 1), employers are required to provide a safe and healthy workplace for employees. To do so, employers must regularly survey the workplace to identify hazards. All identified hazards must be adequately addressed through engineering control measures or changes in work practices. Employers should instruct each employee in the recognition and avoidance of unsafe conditions. In this and similar situations, the employer may need to provide additional training to employees to understand the hazards and how to properly use equipment.
Please use information listed on the Contact Sheet on the NIOSH FACE web site to contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.