
Print Machine Operator is Strangled When His Shirt is Caught on a Rotating Knob
| California Case Report: 09CA006 | ||
Summary
A 38-year-old machine operator was strangled when his clothing caught on a rotating knob of a printing machine. The rotating knobs did not have any guarding or protective barriers around them to prevent inadvertent contact. The CA/FACE investigator determined that in order to prevent future incidents, employers with printing machines that have exposed moving parts should ensure that:
- Employees are protected from moving parts by using printing machines designed with engineered safety features and/or appropriate guards.
Introduction
On Thursday, July 16, 2009, at approximately 1:30 a.m., a 38-year-old machine operator was strangled when his shirt got caught on a rotating knob of a printing machine. He died from his injuries on July 18, 2009. The CA/FACE investigator was notified of this incident on July 20, 2009, by the Santa Ana District Office of the Division of Occupational Safety and Health (Cal/OSHA). On July 31, 2009, the CA/FACE investigator inspected and took pictures of the incident site and interviewed the company president, operations manager, and the attorney representing the company. On August 18 and October 5, 2009, two maintenance personnel and a machine operator were interviewed to discuss the operation of the printing machine.
The employer of the victim was a cosmetic packaging manufacturer of plastic squeeze tubes and custom injection molded products. The employer had been in business for 25 years and had 60 employees. There were 12 employees working at the time of the incident. The victim had been employed with the company for one year as a machine operator and had 14 years of prior experience operating similar machines. The employer had a written Injury and Illness Prevention Program (IIPP). Safety meetings were held regularly and were documented. The employer also had a safety committee in which both management and employees participated. These safety committee meetings were held monthly and included reviews, status reports, and discussions of safety audits, safety action items, and employee safety suggestions.
The employer had a training program that addressed machine operation and safety. At the time of hire with the employer, the victim was provided one-on-one training by an experienced machine operator, and was tested on his knowledge and operational skills of the printing machine. Thereafter, the victim was provided on the job training by supervisory personnel.
Investigation
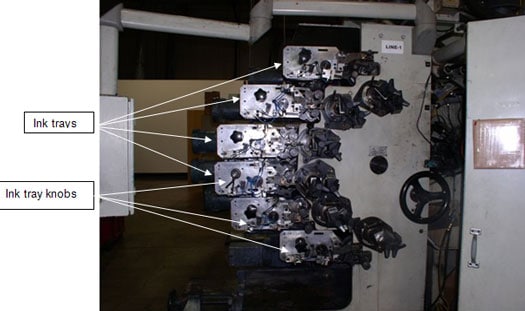
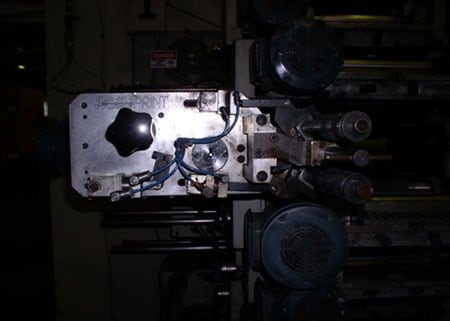
The machine involved in the incident was an automated high-speed, six-color, off set printing machine that was used to decorate plastic squeeze tubes for cosmetic and personal care products. The machine had six trays, each containing different color inks. There were knobs on the end of the ink trays attached to the ink dab roller shafts. The knobs turned constantly while the printer was running. The design of the printing machine required the operator to work in close proximity to the rotating knobs to check on the flow of the ink. There were no guards or barriers preventing inadvertent employee contact with the rotating knobs or the pinch points on the ink trays.
In the early morning on the day of the incident, the victim had stopped the machine to adjust the dab roller to modify the ink transfer rate according to the manufacturer’s procedure. Although the printing had been stopped, the color setup motor remained on and the dab rollers were turning. At approximately 1:30 a.m., a co-worker found the victim unconscious, strangled by his shirt. The shirt had become tangled around one of the ink tray knobs. The machine was not operating at the time. The co-worker began CPR and called for assistance. The paramedics and fire department personnel transported the victim to a local hospital where he died from his injuries on July 18, 2009.
Cause of Death
The cause of death according to the death certificate was asphyxia caused by mechanical compression of the neck.
Recommendations/Discussion
Employers with printing machines that have exposed moving parts should ensure that:
Recommendation #1: Employees are protected from moving parts by using printing machines designed with engineered safety features and/or appropriate guards.
Discussion: In this incident, the victim’s clothing was caught by a rotating knob when he was too close to the moving parts of the printing machine. Although this incident was not witnessed, the victim was probably checking the status of the ink trays while the machine was running. The victim was able to reach the computer screen of the machine and shut the machine off, but was unable to free himself from the rotating knobs. When employees work near moving machinery components, printing plant employers should ensure that safety features and appropriate guards are integral to printing machine design so that employees cannot become entangled and risk injury or death. In this instance, the printing machine was not manufactured with guards over the rotating knobs, and there was no mechanism to ensure that the knobs stopped rotating when the employee checked the ink tray status. For circumstances where guarding is not practical, employers should consider whether a long handled tool is practical and safe to use to perform service or maintenance while the machine is running. The employer in this incident is currently testing a clutch-type mechanism that stops the rotating knobs during machine troubleshooting, cleaning, and set-up. If the employee had been using a printing machine that was designed to prevent inadvertent employee contact with exposed rotating knobs, the victim would not have become entangled with injuries leading to his death.
References
- General Industry Safety Orders – Subchapter 7. General Industry Safety Orders Group 6. Power Transmission Equipment, Prime Movers, Machines and Machine Parts Article 41. Prime Movers and Machinery §4002. Moving Parts of Machinery or Equipment.
- Group 8. Points of Operation and Other Hazardous Parts of Machinery Article 54. Scope and General Definitions, §4184. Guarding Required.
- California FACE Investigation Report: 06CA002 pdf iconexternal icon
http://www.cdph.ca.gov/programs/ohb-face/Documents/06CA002.pdf
Exhibits

|
|
|
|
|
|
|
Exhibit 4. A picture of the name plate affixed to the machine.
|
California Fatality Assessment and Control Evaluation (FACE) Project
The California Department of Public Health, in cooperation with the Public Health Institute and the National Institute for Occupational Safety and Health (NIOSH), conducts investigations of work-related fatalities. The goal of the CA/FACE program is to prevent fatal work injuries. CA/FACE aims to achieve this goal by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact. NIOSH-funded, state-based FACE programs include: California, Iowa, Kentucky, Massachusetts, Michigan, New Jersey, New York, Oregon, and Washington.
To contact California State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.