Supply Motorman Killed by Load Falling from a Forklift
FACE 8412
INTRODUCTION
The National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR) is currently conducting the Fatal Accident Circumstances and Epidemiology (FACE) Study. By scientifically collecting data from a sample of similar fatal incidents, this study will identify and rank factors which increase the risk of fatal injury for selected employees.
On January 26, 1984, a supply motorman with 39 years of mining work experience was helping a forklift operator load crib blocks onto mine flatcars. At approximately 1:20 p.m., one of the crib blocks came off the forklift and fatally injured the supply motorman. The attending medical examiner notified DSR about this fatality on January 27, 1984.
CONTACTS/ACTIVITIES
After receiving notification, DSR sent a research team, consisting of a safety specialist, an industrial engineer, and a statistician, to visit the company and examine the accident site on February 29, 1984. Interviews were held with the mine manager, his assistant, the regional safety manager, the forklift operator, the supply clerk, and a supply motorman. The information obtained from these interviews pertained to the company history, policies and procedures, accident scenario, safety and health training programs, and relevant work practices. The accident site was examined in the presence of three plant representatives who described the site’s appearance when the incident occurred. The site had changed greatly since the fatality had occurred, in that it had over 18 inches of new gravel and had been graded. The forklift, mine flat cars, broken crib block and broken crib straps were all gone from the site. However, the forklift and similar crib blocks and mine flat cars were examined. During the examination 35 mm pictures were taken of the site, forklift, and similar crib blocks.
SYNOPSIS OF EVENTS
The mine site employs approximately 310 employees of which 257 are United Mine Workers and 53 are salaried employees. The mine is an underground mine which produces about 7000 tons of coal a day. The mine is owned by a large corporation which is organized by regions. The northern West Virginia region has ten mines with about 4000 employees which produce about 70,000 tons of coal a day. There are about seven full time company safety officers in the region. For each job classification, the company has Safe Work Instructions (SWI’s), which each employee is supposed to know. However, the company admits that SWI’s for underground jobs are more complete and detailed than their SWI’s for aboveground classifications. No specific SWI’s regarding the handling of crib blocks with a forklift exist.
The victim had worked outside in the supply yard since before 1978 and had 40 years total experience in mining. His co-worker, the forklift operator, had 38 total years in mining experience and had been working in the supply yard since the fall of 1980. However, he had only six months experience in operating the forklift. The forklift operator had been trained, via on-the-job training, by the previous forklift operator.
At 8:00 a.m. on Thursday, January 26, 1984, the supply motorman and the forklift operator received the day’s supply order for the mine from the shop’s supply clerk. They proceeded to clean off the mine cars, straighten out the yard, and prepare the supplies. The two men loaded materials on the mine cars all morning, mostly crib blocks which they loaded off of a truck that had just come in. When they had unloaded all the crib blocks from the truck, they loaded crib blocks which had been sitting outside in the yard for some time. At 11:30 a.m. they took their lunch break.
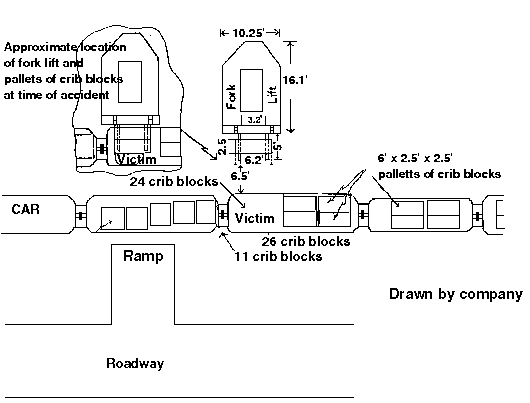
At approximately 11:45 a.m. the forklift operator took some repaired mine cars and placed them on the track. At about 12:00 noon the two men went back to finish loading crib blocks on the 7 foot wide mine flatcars. They had completed loading crib blocks, but noticed that one set of two blocks did not set properly on the mine flat car. The two blocks had dirt and ice on the bottom and had one end about 4 inches too high. Each crib block had 67 cribbing timbers (each of which are 6″ x 5″ x 30″) interwoven into a block (30″ x 30″ x 72″) weighing approximately 1570 pounds. The two crib blocks were each banded by four 1/2 inch steel bands which all ran in the same direction. The forklift operator raised the two crib blocks about 5-1/2 to 6 feet off the ground or 4 to 4-1/2 feet off the mine flat car, while the supply motorman took a shovel, stood in front of the raised load, and knocked the dirt and ice from under the crib blocks. When the blocks were set down on the flatcar, they were still found to sit improperly. So the blocks were raised again, and the supply foreman again used the shovel to knock dirt and ice from the bottom of the blocks. However, one of the cribs suddenly fell on the supply motorman.
It is believed that either the 1/2-inch steel bands broke or the load slipped and fell crushing the motorman. The forklift operator stated that he had the load all the way on his forks, had his forks tipped slightly to the rear, had his forklift in neutral, had his feet on the clutch and the brake, and had set the handbrake. The forklift operator did not see the load fall, but heard it fall. He then backed away about 6-1/2 feet and lowered the load. Three of the four 1/2 inch steel bands were broken and the cribbing was scattered on the car and ground.
The victim was doubled over with one foot on the flatcar and the other on the ground (see diagram). The victim was uncovered by the forklift operator and fellow workers and transported at 1:30 p.m. to the hospital by the emergency medical squad. The victim was alert and cooperative when he arrived at the hospital, but subsequently turned blue. After open cardiac massage and external pacing proved unsuccessful, the victim was pronounced dead at 3:40 p.m.
MEDICAL FINDINGS
Due to the nature of the injury, a physical inspection rather than an autopsy was conducted. The victim had palpable fractures of the upper left leg, both hips and the left ribs. He had a laceration of the left myocardium and bilateral chest tubes drained blood, 300cc from the right lung and 200-300cc from the left. A urinary catheter also drained gross blood. Toxicologic results were negative for blood alcohol. The victim had multiple healed irregular needle scars on the left arm from insulin injections. The victim had a prosthetic left eye. The medical examiner concluded that the cause of death was multiple traumatic injuries.
GENERAL CONCLUSIONS AND RECOMMENDATIONS
A major factor in this incident was the lack of forklift operation experience and training on the part of both the forklift operator and the victim . This type of forklift incident is not uncommon, and occurs in at least 7% of all cases involving forklifts. it is generally recognized in mechanical materials handling that no one should be allowed to work beneath or around a raised forklift load. Company management has already implemented measures aimed at preventing this type of incident from recurring. The bands on the crib blocks have been increased to three quarters of an inch. The whole storage yard has had 18 inches of gravel added and graded to improve yard drainage, thereby preventing ice from forming on the bottom of the crib blocks. Finally, employees have been instructed not to work in front of or beneath a raised forklift load. One further recommendation is to upgrade management’s Safe Work Instructions for aboveground workers by specifically obtaining or developing a formal training program for all forklift operators, mobile crane operators, and other aboveground materials handlers. This is necessary because there are other inherent dangers in forklift and crane materials handling operations which can not be left solely to on-the-job training. On-the-job training by previous operators may pass on unsafe work procedures from the old operator to the new operator. This is particularly true when the employees have a great deal of hazard experience in a previous work environment, but change jobs and have very little hazard experience in their new job environment. They often do not recognize serious hazards, or have a cavalier attitude towards such hazards.
The courtesy and cooperation of the Company officials and employees interviewed by the research team were outstanding and are gratefully acknowledged.