
Solid Waste Compost Facility Worker Dies, Body Is Recovered In Digester Tube - Tennessee
NIOSH In-house FACE Report 2010-01
August 26, 2011
Summary
On July 22, 2010, a 50-year-old worker was found deceased in a compost digester tube at a solid waste facility. The victim worked as a picker on a tipping floor.b His duties were to separate compostable from non-compostable trash that was unloaded onto the tipping floor by residential and commercial waste haulers. Once the trash was separated, the compostable material was pushed into an open digester pit by a co-worker operating a front-end loader. A hydraulic ram located near the pit floor would then push the material into the digester tube.
In this incident, the victim’s shift had begun at approximately 7:00 am. Approximately three hours later coworkers became concerned because he was not at his workstation. Public safety officials were notified and arrived on the scene at approximately 12:15 pm. Emergency workers searched the worksite and surrounding area, as well as the accessible areas of the digester tubes. Three days later, the victim’s body was discovered in one of the tubes approximately ten feet from the loading end.
Note: Subsequent to the NIOSH field investigation, the medical examiner ruled that the victim had died of natural causes related to heart disease. However, since the investigation identified the presence of workplace safety and/or health hazards with the potential to cause serious injury to workers at solid waste facilities, it was decided to report the investigative findings in hopes of providing injury prevention information to employers and workers with similar work environments.
Factors that may contribute to worker injury at solid waste facilities include procedures that place workers-on-foot near moving equipment, unguarded floor openings, limited communication and visual contact with mobile equipment operators, and working conditions that may include high concentrations of toxic gases and high temperatures.
NIOSH investigators concluded that employers should:
- develop, implement and enforce traffic control and worker accountability procedures to ensure equipment and vehicle operators are aware of worker locations
- install and maintain physical barriers that protect workers from falling through floor openings; and develop, train on, and enforce safe work practices when it is not possible to install physical barriers
- develop, implement, and enforce a comprehensive occupational safety and health program that includes training workers in hazard recognition and the avoidance of unsafe conditions
- ensure the working environment is free from harmful concentrations of toxic gases and, when possible, heat stress conditions
aA digester is an enclosed composting system with a device to mix and aerate compostable materials.
bA tipping floor is an unloading area for vehicles that are delivering municipal solid waste to a transfer station or solid waste composting facility.
Introduction
On July 22, 2010, a 50-year-old worker (the victim) died while separating compostable from non-compostable materials at a solid waste processing facility. He was seen at approximately 9:00 a.m. and noted to be absent from his worksite at approximately 9:20 a.m. His body was found three days later inside a composting digester tube. On July 29, 2010, officials of the Tennessee Occupational Safety and Health Administration (TOSHA) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR) of the fatality. On September 1, 2010, a DSR Safety and Occupational Health Specialist and a guest researcher conducted an investigation of the incident. The incident circumstances were reviewed with the investigating TOSHA safety compliance officer, the police investigator, and the victim’s employer. The incident site was visited and the police report along with incident scene photographs and diagrams were reviewed. A copy of the Medical Examiner’s report was requested and was received approximately three months later.
Employer
The victim’s employer operated a solid waste disposal and composting facility that was founded in 1989. Composting operations have been running at the current site since 1992 with the exception of 2007 – 2009 when the facility was being rebuilt due to a destructive fire. The company has 21 employees with 13 individuals working onsite at the compost facility. Two employees, including the victim, worked in the immediate vicinity of the incident. This was the company’s first fatality.
Written Safety Programs and Training
The worksite did not have dedicated safety personnel. The facility manager operated as the safety officer for the site. The company had a generic safety program that they were in the process of updating. On-the-job safety training was provided by facility management personnel.
Victim
The victim was a 50-year-old male who had been working at the site for 10 years. His family and co-workers reported to police investigators that he had a history of cardiovascular disease, and had been suffering from infrequent fainting spells.
Incident Scene
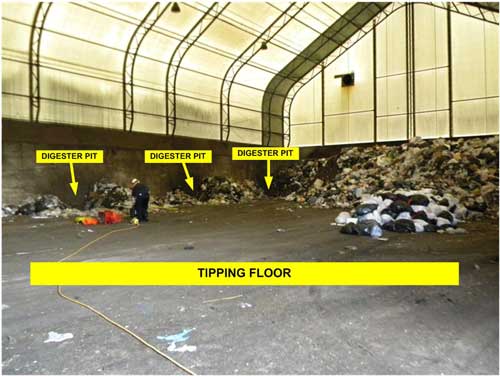
The solid waste facility consists of approximately 200 acres and four waste processing buildings. The fatality occurred in the building where the tipping floor was located. The structure has a poured concrete floor and measures approximately 80 feet x 120 feet (Photo 1). There are five digester pits located along one wall that feed waste into five digester tubes. The pits are approximately six feet square and about five and one half feet deep. Each digester tube can hold 75 tons of composting waste. The tubes are 14 feet in diameter, 180 feet long, and are made of ¾-inch steel. The tipping floor building is equipped with large bay doors and fans to provide ventilation. The temperature inside the building at the time of the incident is unknown.
Work Process
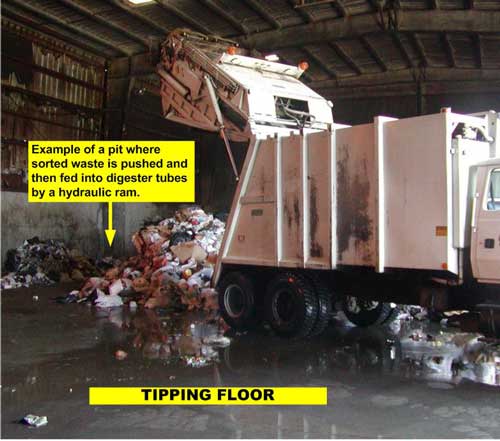
The composting process begins when municipal waste haulers deliver commercial and residential solid waste to the facility. Drivers stop at a weigh station near the entrance to the facility to check in, and then proceed to the tipping floor to dump their load of waste (Photo 2). The picker (victim) then sorts through the waste to remove large items and non-compostable materials that are then taken to an appropriate solid waste landfill. After the non-compostable items are removed, the remaining waste is pushed by a front-end loader (Photo 3) into one of the digester pits (Photo 4).
At the time of the incident the standard operating procedure was for the picker to hand signal to the front-end loader operator when he was done sorting materials and the waste was ready to be pushed into the pit. Radios were not used due to the relatively small size of the tipping floor and the perceived ease of maintaining visual contact. After motioning to the loader-operator, the picker would then move from the area and the front-end loader would push the waste into the pit.
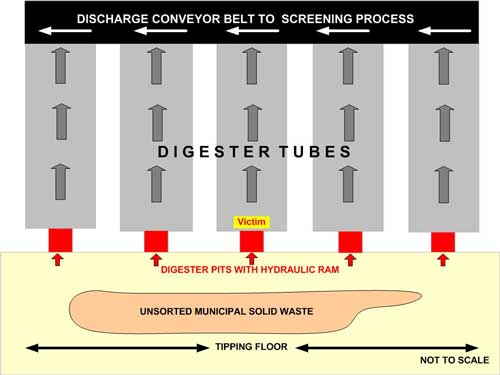
The hydraulic ram in the pit would continuously cycle until all material had cleared the pit and was pushed into the digester tube (Photo 5). The biodegradable material (e.g. paper, food waste and bio-solids) in the waste would break down over a three-day period at a temperature of approximately 120°- 140°F. After this three-day period, the remaining digester material was discharged onto a conveyor belt and sent to a screening process (Diagram). Screened materials were moved by a front-end loader to an aeration floor where the material was periodically turned and dried while continuing the composting process for an additional four weeks.
Weather
The incident occurred in the morning at approximately 9:00-9:15 a.m. At that time, the temperature outdoors was between 77° and 80° F with humidity between 81% and 90%.1 There is no indication that weather played a role in this incident. However, working in high temperatures and humidity without proper monitoring, hydration, resting and cooling breaks, could be stressful to an employee with an underlying heart condition.
Investigation
On July 22, 2010, at approximately 7:00 a.m. the victim reported to his job at the solid waste disposal facility where he worked as a picker on the tipping floor. At 9:00 a.m. the victim directed a waste hauler onto the tipping floor to dump a load of solid waste. The next driver, whose truck weighed in at the facility at 9:17 a.m., did not see the victim upon his arrival. He proceeded onto the tipping floor, dumped his load, and left the premises.
The front-end loader operator reported that he noticed the victim was not in the area, but continued pushing the dumped waste into the digester pits because it was not uncommon for the picker to occasionally leave for short periods without notifying anyone. However, it soon became apparent that the picker was absent from his work area longer than usual. The operator informed management, the process was halted, and workers began searching for the victim.
The police department was notified, and the first detective arrived at approximately 12:15 p.m. Members of the local fire department, rescue squad, ambulance service, police department, and employees of the facility searched the premises for the victim. The search was expanded to the accessible areas of the digester tubes when he was not found in the facility or on the grounds. Due to the hazardous air quality and high temperature conditions inside the tubes, the rescue team adhered to protocols for confined space entry and heat stress conditions by donning appropriate personal protective equipment and limiting their exposure time.
On the third day of the search, July 25, 2010, the victim was found within 10 feet of the loading end of a digester tube. Dental records were used to positively identify the victim and the official ruling on the cause of death as natural causes as reported on December 13, 2010 by the Medical Examiner. It is surmised that the victim may have suffered and succumbed to a medical event prior to falling into or near the pit opening. His body may have been obscured from the loader operator’s field of vision and was fed into the digester tube by the hydraulic ram after falling or being pushed into the pit.
Back to Top
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in an injury or fatality. NIOSH investigators identified the following items as possible factors that may contribute to worker injury at solid waste facilities. Note that it is unknown if any of these factors contributed to this particular incident.
- Work procedures that place workers on-foot near moving equipment.
- Unguarded floor openings in areas where employees are required to travel on-foot to complete regular work duties.
- Limited communication and visual contact between mobile equipment operators and workers-on-foot.
- Conditions that include harmful concentrations of toxic gases and high temperatures.
Back to Top
Cause of Death
The Medical Examiner’s report indicated that the victim died from coronary atherosclerosis, with valvular heart disease and hypertensive cardiovascular disease identified as significant contributing conditions. The trauma to the body was considered post-mortem and the death was ruled to be from natural causes related to heart disease.
Recommendations/Discussion
Recommendation #1: Employers should develop, implement and enforce traffic control and worker accountability procedures to ensure equipment and vehicle operators are aware of worker locations.
Discussion: Effective control of all tipping floor activity through clear understandable directions is very important. The picker is usually the person on the floor for extended periods and should have the capability to safely direct moving traffic and pedestrians. In this facility, the victim did not utilize a radio and tipping floor procedures called for incoming trucks to wait to dump their loads, and the front-end loader operator to wait to begin moving waste into the pits, until instructed by the picker verbally or with hand signals. However, in this case, both a truck driver and the loader operator continued operating without the victim’s clearance to proceed. Although according to the Medical Examiner’s report, it is very likely the victim was deceased prior to his body entering the pit or the digester tube, had he been alive but unable to communicate or free himself from the pit, halting operation of the trucks and the front-end loader may have increased his chances of survival..
Recommendation #2: Employers should install and maintain physical barriers that protect workers from falling through floor openings; and develop, train on, and enforce safe work practices when it is not possible to install physical barriers.
Discussion: The most effective way to control employee exposure to occupational hazards is to eliminate the hazard.2 If the waste was separated prior to being delivered to the facility, there would be no need to sort through the waste after it is dumped onto the tipping floor. The facility manager stated that the third party providers of waste materials have been instructed not to deliver non-compostable materials to the facility. However, due to lack of compliance with this request, the picker position had become an important part of the process. Mandating compliance through contractual penalties may provide an incentive for haulers to eliminate non-compostable items from their loads.
While the open digester pit was unlikely to have been a contributing factor to this fatality, an arrangement such as found at this facility does represent a fall hazard. OSHA Regulation 29 CFR 1910.23(a)(3)(i) indicates that “where operating conditions necessitate the feeding of material into any hatchway or chute opening, protection shall be provided to prevent a person from falling through the opening.”3 Though doubtful in this case, as the picker’s duties were generally located 20 feet away from the digester pit area, it is possible that an individual could fall into the pit, be rendered incapable of getting out, and be further injured by the ram mechanism and falling trash.
In this work process, it is difficult to design a guard for the floor opening because the opening is an integral part of the work process. If the open digester pit was equipped with a guard, a worker, or a procedure, would be required to remove the guard numerous times per work shift to allow material to be pushed into the pits. This could create additional safety hazards including falling into the pit, or being injured by equipment or truck traffic. A removable railing that is mechanized and could be operated remotely, in addition to signage identifying the location of an opening in the floor surface, would aid in mitigating the identified hazards.
The company had requested waste haulers to bring only compostable materials to the facility to eliminate the need for the picker position and remove the hazard of workers and heavy machinery operating in the same workspace. However, due to standard procedures for collecting commercial and residential waste, their efforts were not always successful and there continued to be the need to separate waste prior to beginning the composting process.
The risk of the picker being inadvertently pushed into the pit by the loader could be eliminated if the process were re-designed into a one-person job. This could be achieved by having the front-end loader operator assume the picker duties and separate the compostable from the non-compostable materials prior to pushing the waste into the pit. As a result of this incident, the employer has implemented the single worker process, and installed monitored video surveillance cameras to check on employees working in the tipping floor area.
Recommendation #3: Employers should develop, implement, and enforce a comprehensive occupational safety and health program that includes training workers in hazard recognition and the avoidance of unsafe conditions.
Discussion: A comprehensive written occupational safety and health program should be developed by employers for all workers. The program should include, at a minimum, an explanation of the workers’ rights to protection in the workplace, safe work practices workers are expected to adhere to, specific safety protection for all tasks performed, ways to identify and avoid hazards, and who workers should contact when safety and health issues or questions arise4.
Some minimum components for employers to consider when providing safety training to workers are the following: 1) general recognition and prevention of hazards, 2) safe performance of assigned tasks, and 3) safe use and maintenance of tools or equipment. It is also recommended that the training program content, and the names and dates of employees completing the training, be documented and retained by the employer. Employers should also ensure that the trainer is qualified, as an instructor, through education and/or experience. To ensure the effectiveness of the safety training, an employer might consider ways to ensure that the worker comprehends the important information (e.g., written testing, verbal questions, or role playing in simulated settings).4
In the solid waste treatment and composting industry, it is recommended that a safety program include site-specific hazard recognition and safety training that addresses compliance with all applicable OSHA regulations including, but not limited to: 1) walking and working surfaces3, hazard communication,5 bloodborne pathogens,6 personal protective equipment,7 lockout-tagout and the safe operation and preventative maintenance of equipment8 Hazard recognition training should be based on an evaluation of the tasks workers will perform for all potential hazards. The training should also stipulate that workers never risk physical harm to accomplish tasks.4
Recommendation #4: Employers should ensure the working environment is free from harmful concentrations of toxic gases and, when possible, heat stress conditions.
Discussion: Consideration should be given to the possibility that harmful working conditions could be present, including carbon monoxide from the front-end loaders internal combustion engine, methane gas from the composting waste byproducts, or high temperatures.9
OSHA Regulation 29 CFR 1910.178(i)(1)10 states “Concentration levels of carbon monoxide gas created by powered industrial truck operations shall not exceed the levels specified in 1910.1000,” or 50 ppm11
Methane gas has been a well-documented hazard in work processes involving composting or manure processing.12 It seems unlikely to have been a primary contributing factor to this case for at least two reasons. First, there is a lack of agitation of the composting materials near the opening into the tipping floor room. Second, the picker’s main work area was 20 feet from these openings. However, it is recommended that environmental testing be considered to ensure this is not a risk factor in processes involving composting materials in a closed space.
While hot and humid working conditions are not regulated directly, such regulation can fall under the OSHA General Duty clause Section 5(a)(1) of the Occupational Safety and Health Act of 1970.13 A temperature of 80°F outside with up to 90% humidity on the day of the fatality can give an apparent heat of 87°F, which should be bearable. It is unknown what the temperature inside the building was at the time, but it is feasible it could have exceeded the outside temperature due to the opening of the 120-140°F composting tubes into the tipping floor room. An increase in temperature of only 2°F would increase the heat index to 91°F, elevating the level of heat risk to “extreme caution.” 14 Without proper monitoring, hydration, resting, and cooling breaks this temperature could be stressful for one with an underlying heart condition.
The work area is a large, open room with large bay doors opening to the outdoors. These doors may provide adequate ventilation, but air monitoring would provide an accurate measurement and verify compliance with applicable contaminant permissible exposure levels.
References
- Weather Underground [2010]external icon. [http://www.wunderground.com/history/airport/KTYS/2010/7/22/DailyHistory.html?req_city=Sevierville&req_state=TN&req_statename=Tennessee]. Date accessed: August 2011.
- CDC [2010]. CDC 24/7 Saving lives, protecting people, saving money: Workplace safety and health topics, engineering controls. [ https://www.cdc.gov/niosh/topics/engcontrols/]. Date accessed: August 2011.
- Code of Federal Regulations [2008]. 29 CFR. 1910.23. Guarding Floor and Wall Openings and Holes. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- OSHA [2007]. Training Standards Policy Statement.external icon [https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=25658 ]. Date accessed: August 2011.
- Code of Federal Regulations [2008]. 29 CFR 1910.1200. Hazard Communication. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2008]. 29 CFR 1910.1030. Bloodborne Pathogens. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2008]. 29 CFR 1910.Subpart I. Personal Protective Equipment. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2008]. 29 CFR 1910.147. Control of Hazardous Energy (Lockout/Tagout). Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- CDC [2009]. CDC 24/7 Saving lives, protecting people, saving money: Carbon monoxide poisoning. [ https://www.cdc.gov/co/faqs.htm]. Date accessed: August 2011.
- Code of Federal Regulations [2008]. 29 CFR 1910.178. Powered Industrial Trucks. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2008]. 29 CFR 1910.1000 Table Z-1. Table Z-1 Limits for Air Contaminants. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- CDC [1990]. Preventing Deaths of Farm Workers in Manure Pits. NIOSH Publication No. 90-103, Cincinnati, OH.
- Occupational Safety and Health Act [1970]. Pub L 91-596. 84 Stat. 1590. 29 December 1970. Print.
- NOAA National Weather Service [2010]. Office of climate, water, and weather services: Heat: a major killer.external icon [http://www.nws.noaa.gov/os/heat/]. Date accessed: August 2011. (Link updated 8/14/2012)
Investigator Information
The investigation was conducted by Virginia Lutz, Safety and Occupational Health Specialist, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, and Andrew Yorgason D.O., Guest Researcher, West Virginia University Occupational Medicine Residency Program, Surveillance and Field Investigations Branch, Division of Safety Research. The report was co-authored by the investigators.
Acknowledgement
The NIOSH FACE Program would like to acknowledge the compliance officer and staff of the Tennessee Occupational Safety and Health Division (TOSHA), and the police investigator and local police department, for providing information and assistance with this investigation.
 |
|
Diagram: Composting process flow diagram
|
|
|

|
|
Photo 3. Photo of the front-end loader that was used to push |
 |
|
Photo 4. Photo of the digester pit and hydraulic ram. |
 |
|
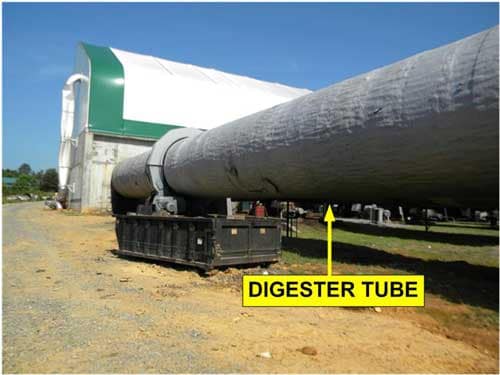
Photo 5. Photo of the digester tube extending from the tipping floor to the discharge area. (Photo courtesy of local Police Department) |
|
Fatality Assessment and Control Evaluation (FACE) Program The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1982, NIOSH initiated the Fatality Assessment and Control Evaluation (FACE) Program. FACE examines the circumstances of targeted causes of traumatic occupational fatalities so that safety professionals, researchers, employers, trainers, and workers can learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent occupational deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under the FACE program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit the program website at www.cdc.gov/niosh/face/ or call toll free at 1-800-CDC-INFO (1-800-232-4636). |