
Hispanic Carpenter’s Helper Dies after Crane Boom Fell on Him during Disassembly - North Carolina
NIOSH In-house FACE Report 2006-01
December 22 , 2006
Summary
On January 30, 2006, a 37-year-old male Hispanic carpenter’s helper (the victim) was fatally injured while assisting in disassembling a lattice boom on a truck-mounted crane. The crane operator and the victim were working together removing pins that secured the 40-foot center section to the base boom section. After dislodging the second bottom pin, the boom hinged on the top two pins and fell on the victim’s back pinning him to the ground. The supervisor summoned a coworker who contacted 911 and company managers immediately. A hydraulic crane located nearby was brought to the site and used to lift the boom off of the victim. Approximately 5 minutes after receiving the 911 call, emergency medical services (EMS) personnel arrived and extricated the victim. They attempted resuscitation but were unsuccessful. EMS personnel notified the EMS medical director of the victim’s condition, and resuscitation efforts were suspended. The victim was transported to the hospital where he was pronounced dead about 45 minutes after the incident.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should
- ensure that manufacturer’s safety recommendations for proper blocking and support procedures to prevent movement of the boom sections are implemented when disassembling cranes
- ensure that all workers assigned to disassemble or assist in disassembling cranes are trained on correct procedures, using a language and literacy level that workers can understand, so that they can recognize the hazards of improper disassembly sequences
- ensure that prework safety meetings are conducted each day to discuss the work to be performed, identify the potential safety hazards, and implement safe work procedures to control the hazards.
Introduction
On January 30, 2006, a 37-year-old male Hispanic carpenter helper (the victim) was fatally injured while assisting in disassembling a truck-mounted crane boom at a bridge construction site. On February 16, 2006, the North Carolina Occupational Safety and Health Administration (NCOSHA) office notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), of the incident. On April 11 and 13, 2006, a DSR safety and occupational health specialist met with the NCOSHA compliance officer assigned to the incident. The DSR safety and occupational health specialist traveled to the company headquarters on April 12, 2006, and met with the company’s managers and reviewed training records. The DSR safety and occupational health specialist traveled to the incident site with the company’s safety manager and interviewed the crane operator, a coworker who witnessed the incident, the bridge superintendent and the project manager. The incident site and the crane were examined. The police report and medical examiner’s report were reviewed. The cause of death was obtained from the medical examiner’s report.
Employer
The victim’s employer, a construction company specializing in highway and bridge construction, employed over 1,200 employees (300 of whom were Hispanic) and had been in business for fifty-four years. On the day of the incident, the company had eight employees on the bridge construction site, two of whom were directly involved in the disassembly process.
Victim
The victim was employed as a carpenter’s helper and had worked for the company on- and-off for 2 years on a seasonal and job-completion basis. His country of origin was Mexico and he spoke Spanish. He had attended a general employee orientation session that dealt primarily with an overview of the company’s history, employee compensation, and general rules of conduct for employees. His attendance was documented. According to the company representative, employees, including the victim, were provided with a copy of the company’s corporate safety and health program at the time of hire, but this document was written only in English. The victim was not provided with training that specifically addressed hazards associated with working near cranes. There were no records that documented that the victim had received any training sessions in Spanish. The victim’s primary job duties included tasks such as constructing wood forms and cutting concrete and rebar.
Note: The victim’s age recorded on company records and based on documentation provided by the victim at the time he was hired, was 48 years old. The NCOSHA compliance investigation record reflects that age. During the course of the medical examiner’s investigation, a close personal associate of the victim provided official documentation that indicated that the victim was 37 years old at the time of the incident, therefore age 37 was used for the victim’s age in this report.
Equipment
The truck-mounted lattice boom crane used at the time of the incident was a 1985 model and was purchased in used condition by the employer in 1990. The crane had been inspected monthly by company employees and inspections were documented. No problems with the crane were identified. An abbreviated visual inspection of the crane conducted by the NCOSHA compliance officer on January 30, 2006, did not reveal any apparent mechanical defects. The operator’s manual was kept in the cab of the truck-mounted crane.
Safety Program and Training
The company had a safety and health training program which was written in English. According to the full-time safety manager, portions of the safety program were translated as needed into Spanish by another full-time employee in the safety office who was bilingual. Documents such as ladder safety, scaffolding safety, and fall protection were available in Spanish. The safety and health program did not specifically address the company’s safety procedures and training for workers-on-foot in construction areas, nor did it provide specific procedures for protection of workers during crane assembly and disassembly. Safety meetings (called safety huddles by the company) were routinely held each morning before work, but a safety huddle was not held on the day of the incident because the supervisor who conducted them arrived to work late due to an off-site appointment. These meetings were conducted in English.
The crane operator involved in this incident had worked for the company for 6 years and spoke English. He received crane operator certification from the National Commission for the Certification of Crane Operators in 2005. This type of certification requires extensive class room training and supervised crane operation.1 The crane operator was deemed by the company to be a competent person for crane operation and it was within his job duties to disassemble crane booms. The company had a team of two workers who ordinarily conducted crane boom disassembly, but one of these workers was occupied with another crane on the day of the incident, and the other worker had not arrived on the jobsite when disassembly began. The crane operator involved in the incident had trained under them.
This was the employer’s first fatality in its Bridge Construction Division. There had been 5 fatalities in its Highway Construction Division over the company’s 54 years of operation; none involving cranes.
Back to Top
Investigation
The incident site was a bridge overpass, part of a larger state-funded highway construction project that began August 4, 2005, and was to be completed by July 1, 2007. A truck-mounted crane with an 80-foot lattice boom (Photo1) had been used to set approximately 20 girders which spanned the southbound lanes of the bridge. The next task, unloading and placing concrete decking over the girders, required a longer boom. The company had a 30-foot and a 40- foot lattice boom section lying on the ground next to the truck mounted crane. These sections were to be assembled and then added to the existing 80-foot boom (which was comprised of a 20-foot end boom section, 40-foot center section, and a 20-foot lower boom section). The boom on the truck-mounted crane was to be disassembled between the 40-foot center section and the 20-foot lower boom section. After the 70-foot section was inserted, the overall boom length was to be 150 feet.

|
|
Photo 1. This photograph illustrates the truck-mounted lattice boom crane that was involved in the incident |
Work began at about 7 a.m. on the day of the incident. The crew was told that a truck carrying concrete bridge panel decking was on its way to the site and the decking needed to be offloaded and placed on the bridge that afternoon. According to the crane operator, there was a sense of urgency to get the crane ready for the day’s work. The site superintendent, crane operator, and two carpenter’s helpers assembled the 70-foot section of boom. After the boom section was assembled, the site superintendent walked about 100 feet away and helped unload materials for the next phase of the job.
The crane operator was left in charge of the crane assembly and disassembly, and he asked the victim to help him disassemble the boom so that they could insert the 70-foot section. Note: The crane operator reported that he had some experience in his training with disassembly and assembly of booms, as it had been covered briefly in his crane operator classes. He had performed boom assembly and disassembly procedures with the company’s more experienced crew many times, but he had not taken the lead in disassembling a boom before the day of the incident.
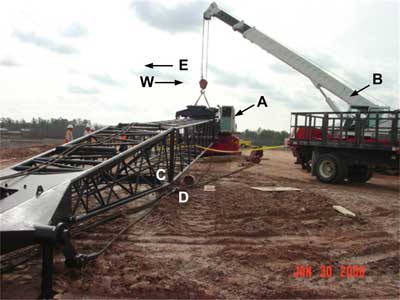
The crane operator began the process of disassembly so that they would be ready when the concrete decking arrived. The crane operator lowered the hook block assembly to the ground and placed it to the left (west) side of the crane. He then lowered the 80-foot boom, resting the peak of the end boom section on the ground (Photo 2-peak is marked A). The live mast was then lowered and the cables and pendants were slackened. The 40-foot center section was about four feet off of the ground. The crane operator asked the victim to help him remove the pins that secured the 40-foot center section to the 20-foot lower boom section. There were four pins securing the center section to the lower boom section, two upper and two lower pins. Each pin was about seven inches long, two inches in diameter, tapered on one end, and secured with a cotter pin. The crane operator went under the boom and knocked out the first lower pin easily. He tried to knock out the second lower pin, but it would not budge. The victim picked up the pin that had landed on the ground on the west side of the lattice boom and indicated with hand motions that he could use it as a punch to drive out the second bottom pin. The crane operator moved from under the boom and reached through the lattice and pounded on the pin held by the victim as the victim, located under the boom, held the first pin against the second bottom pin. The crane operator reported that he told the victim to move as the boom could fall, and the victim moved from the center section to underneath the lower boom section. After the crane operator pounded on the pin about four more times with a sledge hammer, the second bottom pin came out. The boom hinged on the top two pins and the lower boom section fell on the victim’s back and pinned him to the ground (Photo 3). It was approximately 8:30 a.m.

|
|
Photo 2. This photograph illustrates the peak of the lattice boom (A) after it had been lowered to the ground |

|
|
Photo 3. This photograph illustrates a close up of the location where the victim was struck by the boom. The 4×4’s shown on the photograph were brought to the site and used to pry the boom up as it was lifted by the second crane. The pin is marked with a circle and was one of two lower pins removed. The two lower pins had been replaced during rescue efforts. An insert shows a larger illustration of the pin. |
The supervisor called a coworker who immediately called 911, and then company managers. Within about 5 minutes, a hydraulic crane located nearby was positioned next to the lattice boom. The crane operator rigged a strap to the lattice boom, connected it to the hook of the hydraulic crane, and lifted the boom off the victim (Photo 4). The two pins were driven back into place to secure the boom sections.
|
|
Photo 4. This photograph illustrates the truck-mounted lattice boom crane (A) that was involved in the incident. It was taken after the hydraulic crane (B) had been used to lift the boom section off the victim and both lower pins had been replaced. The victim’s location at the time of the incident is marked with a C, and a D illustrates the location of the crane operator. |
Approximately 5 minutes after receiving the 911 call, EMS personnel arrived and extricated the victim. They attempted resuscitation but were unsuccessful. At 8:45 a.m. cardiac monitoring indicated asystole (disruption of normal heart beat). EMS personnel notified the EMS medical director of the victim’s condition and resuscitation efforts were suspended. The victim was transported to the hospital at 9:15 a.m. where he was pronounced dead.
Back to Top
Cause of Death
The medical examiner’s office reported that the cause of death was traumatic asphyxiation due to blunt force trauma.
Recommendations/Discussion
Recommendation #1: Employers should ensure that manufacturer’s safety recommendations for proper blocking and support procedures to prevent movement of the boom sections are implemented when disassembling cranes.
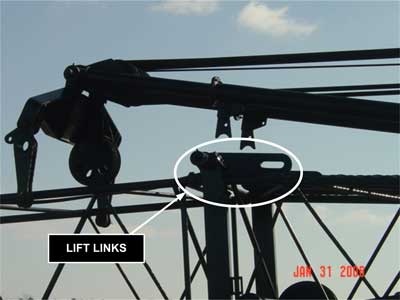
Discussion: According to the crane operator involved in the incident, the operator’s manual located in the truck-mounted crane was the sole source of safety procedures for crane operation at the company. The crane operator stated that he had observed the assembly and disassembly of the boom crane with the assistance of a second or “helper crane.” He stated that the “helper crane” would support the boom by hooking onto a nylon strap wrapped around the lower boom section. At other times, if the helper crane was not available, they (the crane operator and one of the team of two workers with more experience in disassembly) would use the live mast as a hoist and connect a hook from the live mast to a nylon strap wrapped around the lower boom section of the boom. Tension on the hoist cable would support the boom. Workers interviewed by NCOSHA reported that this was a common practice, that they believed these procedures were written in the operator’s manual, and that the company did not have any alternative written procedures. The trainer for crane operators employed by the company agreed that this was the practice, provided that the crane boom was 80 feet or shorter. An authorized manufacturer’s procedure required the retraction of the live mast to a 20-foot length, and attachment to the lower boom section with the lift links (Photo 5). As an alternative, the manufacturer’s disassembly procedure recommended blocking tightly under the pin connection before removing the pins.2 The crane operator involved in the incident indicated that this would be too time consuming for the task. The operator’s manual did not include instructions on the use of a “helper crane,” or instructions for connecting the live mast hoist to a strap wrapped around the boom, indicating that the workers were mistaken about the safety procedures written in the operator’s manual for this truck-mounted crane. The company safety manager indicated that the company’s written crane operation procedures were out of date and the company had made it a policy to use only the safety procedures written in the operator’s manual for each crane. Supervisors should ensure that safety measures specified in the manual are followed and the procedures are reviewed with all involved workers before each assembly and disassembly. Since the operator’s manual does not assign responsibility for crane assembly and disassembly tasks, company policy and retraining should also cover these responsibilities.
|
|
Photo 5. This photograph illustrates the lift links that are used to secure the mast and the boom on booms 80 feet and under |
The manufacturer’s operator’s manual for the crane used in the incident provides the following WARNING:
“Incorrect Disassembly Of A Pin Connected Boom May Result In Machine Damage, Personal Injury, Or Even Death. Before Disassembling Boom, Read And Be Sure You Understand Fig. 7-23 And The Disassembly Procedures In This Section Of The Operators Manual. As An Alternative Disassembly Procedure, Block Tightly Under The Pin Connection Before Removing Pins. Never Stand Under A Boom When Removing Pins.”2 Note: The above warning is provided as an example of the information contained in the operators manual for the crane used in this incident and is only a small part of the section on disassembly. For complete information regarding the manufacturer’s safety recommendations for crane handling and operation, employers and operators should always refer to the operator’s manual for that specific crane.
An additional resource that provides recommendations for proper blocking and support of boom cranes during disassembly procedures is the NIOSH ALERT entitled Preventing Worker Injuries and Deaths from Mobile Crane Tip-Over, Collapse and Uncontrolled Hoisted Loads.3 This alert is available through the NIOSH website at https://www.cdc.gov/NIOSH/docs/2006-142 or by calling 1-800-356-4674. The Alert recommends that employers ensure that crane operators follow the manufacturer’s recommended assembly and disassembly and maintenance procedures when working on cranes and more specifically states that employers should ensure that employees:
- Use proper blocking methods to adequately support crane components during these operations.
- Block boom sections under each section’s support member to ensure the weight of the section is safely supported.
- Do not block between the support members, as this may cause damage to the boom section.
- Always check to ensure boom pendants (boom suspension cables or lines) are properly located before removing a connecting pin. The boom pendant should be between the pin and the crane body so that it supports the boom section closest to the crane body.
- When removing pins, block or support the removing boom sections(s) to prevent their collapse.
Refer to the manufacturer’s recommendations for long booms and booms with jibs.”
The Alert also recommends that riggers and ground workers located near hoisting operations follow the correct assembly and disassembly procedures when setting up or dismantling a crane, check to make sure boom sections are blocked or supported before removing pins, and warns them not to stand under the boom.3
Recommendation #2: Employers should ensure that all workers assigned to disassemble or assist in disassembling cranes are trained on correct procedures, using a language and literacy level that workers can understand, so that they can recognize the hazards of improper disassembly sequences.
Discussion:The victim was not specifically trained in safety hazards associated with disassembling booms in English or Spanish, and had never helped disassemble a crane boom before. The crane operator spoke English and, although a trained and certified crane operator, had never performed boom disassembly procedures as the lead worker before. He reported that there was a sense of urgency to get the crane ready for the tasks at hand, and that he forgot about making sure that the boom was supported. Just before the incident occurred, he motioned to the victim to move as the boom could fall on him, but the victim moved from under the center section to under the lower boom section.
This incident underscores the importance of ensuring that all members of the crew have a basic understanding of the correct procedures involved in hazardous operations such as assembling or disassembling cranes. Additionally, if the victim had fully appreciated the potential for uncontrolled movement, he may have positioned himself to the side of the boom rather than underneath, minimizing the danger of being struck by falling boom sections. The training should reiterate that boom sections need to be supported during disassembly, that standing anywhere near a crane during disassembly is hazardous, and that pins used to hold boom sections together are always to be removed while standing outside the boom, never under it. Training should emphasize that workers must stand to the side and reach through the lattice to remove the pins.
Employers are required to follow Occupational Safety and Health Administration (OSHA) standards which mandate safety training and education in the recognition and avoidance of unsafe conditions, and the regulations applicable to the work environment to control or eliminate any hazards or other exposure to illness and injury (29CFR 1926.21(b)(2)).4 Employers should ensure that all workers who are to work on and around cranes used in construction are trained to follow all standards found in Occupational Safety and Health Administration (OSHA) 29 CFR 1926.550,5 cranes and derricks.
Information useful for safety training for workers who work around or operate cranes can be found in the NIOSH ALERT entitled Preventing Worker Injuries and Deaths from Mobile Crane Tip-Over, Collapse and Uncontrolled Hoisted Loads3 available through the NIOSH web site at https://www.cdc.gov/niosh or by calling 1-800-356-4674. The Alert contains a tear-out sheet that summarizes safety precautions for operators of mobile cranes and for those who work on or around mobile cranes. Including the Alert in jobsite training materials and posting the tear-out sheet at the worksite may serve as an additional means of communicating safe work procedures to workers. Fatality case reports provide another valuable source for use in safety training programs and can be accessed by using the NIOSH Website www.cdc.gov/niosh/face. FACE report No. 97-03 describes another fatality that occurred during crane boom dismantling.6
Workers should be trained using a language and a literacy level they understand. OSHA developed the Compliance Assistance: Hispanic Employers and Workers web page to assist employers with a Spanish-speaking workforce in learning more about workplace rights and responsibilities, identifying Spanish-language outreach and training resources, and learning how to work cooperatively with OSHA. In addition, the web page provides a list of OSHA’s Hispanic/English-as-a-second-language coordinators, fact sheets, Quick Cards, public service announcements, success stories, dictionaries, electronic assistance tools, and other useful information to help protect Hispanic employees’ health and safety. These materials are available at https://www.osha.gov/dcsp/compliance_assistance/index_hispanic.htmlexternal icon 7 or can be obtained by contacting an area OSHA office. Information provided can be used by employers who are developing or improving safety and training programs for their Spanish speaking employees.
Recommendation #3: Employers should ensure that prework safety meetings are conducted each day to discuss the work to be performed, identify the potential safety hazards, and implement safe work procedures to control the hazards.
Discussion: The company foreman or superintendent normally conducted a prework safety meeting, or in this case a “safety huddle,” in English each morning before work. On the day of the incident a safety huddle was not held. It is not possible to know if such a safety talk that morning would have focused on the specific hazards associated with boom disassembly. However, safety huddles, conducted in a language and at a literacy level that all workers could understand, could be used as an opportunity to discuss the work to be done and the associated hazards inherent to such work. During the pre-work meeting, the time-frames for the day’s work tasks could have been discussed and work tasks re-ordered to allow sufficient time for workers who had more extensive experience with boom disassembly to arrive and help perform the boom disassembly.
Back to To
References
- NCCCO [2006]. Certification Programs. [http://www.nccco.org/nccco/certification-programs/certification-overviewexternal icon] Date accessed: September 6, 2006. (Link updated 8/13/2013)
- Manufacturers Operator’s Manual.[1995].
- NIOSH [2006]. Alert: Preventing worker injuries and deaths from mobile crane tip-over, collapse and uncontrolled hoisted loads. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No.2006-142.
- Code of Federal Regulations [2005]. 29 CFR 1926.21(b)(2). Safety training and education. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2005]. 29 CFR 1926.550 Cranes and derricks. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
- NIOSH [1997]. Mechanic fatally injured during dismantling of crane at scrap metal yard-Pennsylvania. Morgantown, WV: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report No. 97-03.
- OSHA [2006]. Compliance Assistance: Hispanic Employers and Workers. https://www.osha.gov/dcsp/compliance_assistance/index_hispanic.htmlexternal icon Date accessed: September 7, 2006
Investigator Information
This investigation was conducted by Doloris N. Higgins, Safety and Occupational Health Specialist, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, National Institute for Occupational Safety and Health.