
Hispanic Flagger Dies After Being Run Over by a Dump Truck - North Carolina
NIOSH In-house FACE Report 2004-10
July 22, 2005
Summary
On June 29, 2004, a 34-year-old Hispanic flagger (the victim) died after being run over by a partially-filled dump truck. The victim was a member of a three-man crew filling drop-off areas along the shoulders of a secondary state road with a dirt/gravel mixture of unclassified stone, also known as UCL. The victim was flagging from a position on the passenger side of the ten-wheel dump truck, on the shoulder of the opposite side of the road. As the amount of UCL became insufficient to level the road shoulder, the driver-side worker motioned for the truck driver to stop the truck and raise the bed to allow more UCL to flow to the rear of the truck. When sufficient material to fill the low spots again began to flow, the worker motioned for the driver to pull forward. As the truck moved forward, the rear of the truck swayed and the driver-side worker again motioned the driver to stop. He then walked around the rear of the truck to the passenger side and discovered the victim underneath the two sets of rear tandem wheels. He called to the driver, who ran around the front of the truck to the passenger side and immediately called 911 from a cell phone. Emergency Medical Service (EMS) and fire personnel responded and used a jack to raise the rear axle of the truck and extricate the victim. Two emergency room physicians passing the scene stopped to assist the EMS personnel in treating the victim. The victim was transported by life flight helicopter to the hospital where he was pronounced dead by the attending physician.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
- develop, implement and enforce a comprehensive safety and training program in language(s) and literacy level(s) of workers, which includes training in hazard recognition and the avoidance of unsafe conditions, including the identification of blind areas around construction vehicles
- ensure that roadway construction workers strictly adhere to the provisions on temporary traffic control set forth in the Manual on Uniform Traffic Control Devices (MUTCD)
- consider the use of proximity warning devices such as radar and sonar based systems and/or rear view-camera systems to enable operators to detect when someone is near or approaching a vehicle or piece of machinery
- ensure that before each work shift begins, communications signals between machine operators and workers on foot are reviewed and confirmed
- consider instituting a progressive discipline program to reinforce the need for workers to follow established safe work procedures
- ensure that the nearest area office of the Occupational Safety and Health Administration is notified within 8 hours of a fatality or in-patient hospitalizations of three or more workers as a result of a work-related incident at their company
Introduction
On June 29, 2004, a 34-year-old Hispanic flagger (the victim) died after being run over by a partially-filled dump truck. On July 7, 2004, officials of the North Carolina Occupational Safety and Health Administration (NCOSHA) notified the Division of Safety Research (DSR) of the incident. On August 17- 19, 2004, a DSR senior investigator conducted an investigation of the incident. The case was reviewed with the NCOSHA compliance officer assigned to the case. The incident site was visited but it could not be determined exactly where the incident took place since work on the project had been completed. Photographs taken by the North Carolina Highway patrol immediately after the incident and the Highway Patrol incident report were reviewed. A copy of the Highway Patrol report was obtained. A copy of the contract between the employer and the North Carolina Department of Transportation (NCDOT) was obtained from the (NCDOT) district engineer.
The employer was a paving and seal coating contractor that had been in operation for 30 years and employed 4 workers at the time of the incident. The employer had no written safety and health or worker training programs. The employer held periodic safety meetings as he deemed necessary and discussed job hazards with employees on a regular basis. None of these meetings were documented. The employer received a video tape on work zone safety and flagger duties from NCDOT two days after being awarded the contract to do the work. He said that he gave the tape to the workers and told them to take it home and watch it. The employer did not ensure that the workers had watched the tape and did not question or test them on the content of the tape. The video tape was presented in English. The employer and the driver/crew chief spoke only English. The victim and his coworker spoke “broken” English, but the employer and crew chief felt that both workers clearly understood any instructions given. The NCOSHA compliance officer stated that he conversed with the coworker in English without any difficulty. The victim had worked for the employer for approximately two months. This was the employer’s first workplace fatality.
Back to Top
Investigation
The employer had been contracted by the state Department of Transportation (DOT) to perform “shoulder–rutting” operations on select two-lane, low-volume roads in two counties. This involved filling drop offs on the sides of the roads an inch or more in depth with a dirt/gravel mixture known as UCL. Work had begun on the project June 16, 2004, and was to continue until all the roads had been completed.
The employer had agreed to a fully operated equipment rental proposal whereby he would provide the equipment and personnel necessary to perform the work to the DOT at an hourly rate. The contract stipulated that although the employer could use two flaggers while the work was being performed, he would only be reimbursed for one. The Manual on Uniform Traffic Control Devices (MUTCD)1 indicated that only one flagger was necessary for the job because of the low volume of traffic on the road and the good sight conditions afforded the flagger. There was a verbal understanding between the employer and the DOT that only one flagger would be used.
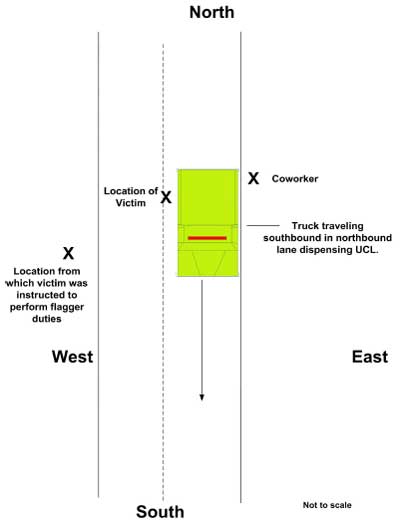
Work started at 7:00 a.m. on the day of the incident. The crew was working in a southbound direction in the northbound lane of a five-mile stretch of road (Diagram). The crew consisted of a truck driver/crew leader, a worker positioned on the driver side of the truck with a rake to smooth the fill mixture as it was dispensed from the rear of the truck, and the victim, positioned on the opposite shoulder of the road with his flag. The ten-wheel dump truck blocked the northbound lane of the road. Work on the southbound lane had been completed the previous day. The workers were wearing hard hats and reflective vests. The workers were equipped with two-way radios that they wore at their waists. The noise level at the rear of the truck was measured at 90 dba by the OSHA compliance officer. The noise level in the truck cab was measured at 76 dba with the truck idling. This would have made it very difficult for the workers to hear any radio signals during normal operations with the position of the radios.
As the truck bed was raised, UCL would slide into a hopper at the rear of the truck. It would then be dispensed onto a conveyor that would deposit it on the northbound lane shoulder where a coworker would smooth it with a rake. The victim had been instructed by the truck driver/crew leader to stand on the shoulder of the southbound lane to serve as a flagger to direct traffic around the truck as work progressed (Diagram).
At approximately 11:00 a.m., two miles of the road had been completed. The truck bed was raised between five and six feet in the air and approximately two thirds of the load had been dispensed. The truck driver stated that the last time he had seen the victim he was positioned at the rear of the passenger side of the truck, approximately thirty inches from the side of the truck.
The coworker signaled by hand for the truck driver to raise the bed a little farther to allow more UCL to be dispensed into the hopper. The coworker then motioned the truck driver by hand to pull forward. As the truck moved forward the coworker saw the rear sway and the truck driver felt a bump. The coworker walked around the back of the truck to the passenger side and saw the victim under the truck’s rear passenger-side tandem wheels. He called to the truck driver who ran around the front of the truck to the passenger side and immediately called 911 from his cell phone. Emergency medical service (EMS) and fire personnel responded within ten minutes and used a jack to lift the rear wheels of the truck and extricate the victim. Two emergency room physicians riding bicycles past the scene stopped and assisted in treating the victim. The victim was transported by helicopter to a trauma center where he was pronounced dead by the attending physician.
Although not a factor in this incident, the NCDOT, the North Carolina Highway Patrol investigating officer, and the NCOSHA compliance officer assigned to the case, stated that two warning signs were placed on each end of the work zone in accordance with the MUTCD. Two NCDOT inspectors visited the site at least once daily and stated that all warning signs were in place and the operation was progressing in accordance with the MUTCD. The inspectors were at the site earlier the day of the incident and said the job was progressing as it should. They also stated to the NCOSHA compliance officer that the victim was stationed on the opposite shoulder of the road. Varying distances between the signage and the work zone were given by the investigating parties (North Carolina Highway Patrol and NCDOT). The signage had been removed at the time of the NIOSH investigation making it impossible to determine the exact distance between the signage and the work zone.
Back to Top
Cause of Death
The attending physician listed the cause of death as massive internal trauma.
Recommendations/Discussion
Recommendation #1: Employers should develop, implement and enforce a comprehensive safety and training program in language(s) and literacy level(s) of workers, which includes training in hazard recognition and the avoidance of unsafe conditions, including the identification of blind areas around construction vehicles.2
Discussion: Over the past several years, the United States has seen a dramatic increase in its population of Hispanic, Spanish-speaking citizens who are entering the work force. The Bureau of Labor Statistics estimated 15.4 million employed Hispanics in 2000, making up 10.9% of the U.S. workforce. The Hispanic workforce increased 43% between 1990 and 2000, and is expected to increase another 36% by 2010 to nearly 21 million employed Hispanic workers.3
A comprehensive safety and training program should identify required safety training (e.g., flagger duties and basic roadwork work site safety). Overcoming language and literacy barriers is crucial to providing a safe work environment for a multilingual workforce. Companies that employ workers who do not understand English should identify the languages spoken by their employees, and design, implement, and enforce a multilingual safety program. The safety program and training should be developed at a literacy level that corresponds with the literacy level appropriate for the company’s workforce.
Employers should ensure that employees who do not speak English or have limited use of English are afforded an interpreter who can clearly convey instructions, and ensure that employees clearly understand the instructions given. The safety and training program, in addition to being multilingual, should include a competent interpreter to explain worker rights to protection in the workplace, safe work practices workers are expected to adhere to, specific safety protection for all tasks performed, ways to identify and avoid hazards, and who they should contact when safety and health issues or questions arise. A method to ensure comprehension could include testing to ensure that the information conveyed was understood. In this incident, the victim was given a Department of Transportation tape in English that detailed basic flagger duties and how to perform them safely. It is not certain that the victim watched the tape, or if he did, that he fully understood the instruction or comprehended the hazards associated with not following safe work procedures. If videos are used as a training tool, they should be viewed in the presence of employers or their representatives. This would allow any questions the employee might have to be answered, and would allow for a clear definition of the role of each crew member. Additionally, neither the NCOSHA compliance officer nor the NCDOT engineer knew of any training the victim had received as to the existence of blind spots around construction vehicles. It could not be determined if the victim understood the existence of blind areas around construction vehicles and the driver’s inability to see him when he was positioned in certain locations. Roadway construction workers should be made aware that blind areas exist around construction vehicles and they should receive training in the identification of these blind areas.
Additional safety information and recommendations for protecting roadway construction workers can be obtained from the NIOSH document entitled “Building Safer Highway Work Zones: Measures to Prevent Worker Injuries from Vehicles and Equipment.”4
Recommendation #2: Employers should ensure that workers strictly adhere to the provisions on temporary traffic control set forth in the Manual on Uniform Traffic Control Devices (MUTCD).1
Discussion: Section 6E.05 of the MUTCD states that at a spot lane closure where adequate sight distance is available for the safe handling of traffic, the use of one flagger may be sufficient. At a spot lane constriction, the flagger may have to take a position on the shoulder opposite the closed section in order to operate effectively. The victim reportedly had been instructed by the crew leader to position himself on the opposite shoulder of the road to perform his flagging duties, and to stay in that position as the work zone progressed. Although the NCDOT said that two flaggers could be used on the job, a verbal agreement between the NCDOT and the employer allowed compensation for only one flagger. Both parties felt that with the low volume of traffic on the road, one flagger would be sufficient. After the incident, the agreement was amended to require two flaggers on the job. Whenever possible, two flaggers should be used. This would allow the flaggers to be positioned well in front of and behind the truck, eliminating the workers’ exposure to moving equipment.
Recommendation#3: Employers should consider the use of proximity warning devices such as radar and sonar based systems and/or rear-view camera systems to enable operators to detect when someone is near or approaching a vehicle or piece of machinery.4
Discussion: Roadway construction workers often work in close proximity to moving vehicles or heavy equipment. Being exposed on a daily basis to the constant noise can desensitize individuals to the movement of such vehicles. Additionally, devices such as a strobe light or different noises should be considered as additions to the standard alarm systems to warn workers of a moving vehicle. Radar or sonar based systems as well as rear-view camera systems are available for use in these conditions and can detect the presence of persons in the blind spots of vehicles and provide a warning to the driver.
Recommendation #4: Employers should ensure that before each work shift begins; communications signals between equipment operators and workers on foot are reviewed and confirmed.
Discussion: In this instance, the crew was equipped with two-way radios; however, noise levels outside the truck cab and around the truck and conveyor would have made it very difficult for the ground workers to have heard any communications, given the fact that they were wearing the radios at their waist. In instances where the effectiveness of two-way radios is compromised, other methods of communications, such as hand signals, should be explored. Once a method of communication is agreed upon, the signals should be reviewed and confirmed by all crew members before work begins.
Recommendation #5: Employers should consider instituting a progressive discipline program to re-enforce the need for workers to follow safe work procedures.
Discussion: The company owner, the truck driver/crew leader, and the other crew member had all spoken to the victim concerning his practice of positioning himself too close to the truck during work operations. The victim had been reportedly verbally reprimanded by the company owner for similar previous behavior, and the truck driver stated that he warned the victim to stay away from the side of the truck. Employers should consider implementing a progressive discipline program to deter such behavior, and explain why displaying such behavior could expose a worker to serious injury or even death. The progressive discipline program could consist of 1) a verbal warning after the first offense; 2) a written reprimand after the second offense; and 3) dismissal after the third offense. Knowledge that these disciplinary actions would take place may help to reinforce the need to follow established safe work procedures for workers.
Recommendation #6: Employers should ensure that the nearest area office of the Occupational Safety and Health Administration is notified within 8 hours of a fatality or in-patient hospitalizations of three or more workers as a result of a work-related incident at their company.5
Discussion: Within eight hours after the death of any employee from a work-related incident or the in-patient hospitalization of three or more employees as a result of a work-related incident, employers must report the fatality/multiple hospitalizations by telephone or in person to the area office of the Occupational Safety and Health Administration (OSHA), U.S. Department of Labor, that is nearest to the site of the incident. Employers may also use the OSHA toll free central telephone number, 1-800-321-OSHA (1-800-321-6742). This early reporting allows OSHA investigators to accurately assess the hazards present and to remove other workers from potential hazardous situations. In this incident, the employer was unaware of this reporting requirement and thought the fatality would be reported by the “authorities” that were present at the site after the incident.
Back to Top
References
- FHWA [2003]. Manual on uniform traffic control devices. U.S. Department of Transportation, Federal Highway Administration (FHWA).
- Code of Federal Regulations 2001 edition. 29 CFR 1926.21(b)(2). Safety Training and Education. Washington, D.C.: U.S. Printing Office, Office of the Federal Register.
- BLS [2001]. BLS Releases 2000-2010 Employment Projections. [http://www.bls.gov/news.release/History/ecopro_12032001.txttxt iconexternal icon]. Date accessed: November 19, 2004. (Link updated 3/20/2008)
- Pratt SG, Fosbroke DE, Marsh SM [2001]. Building Safer Highway Work Zones: Measures to Prevent Worker Injuries from Vehicles and Equipment. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (Pub. No. 2001-128).
- Code of Federal Regulations [2003]. 29 CFR 1904.39(a). Reporting fatalities and multiple hospitalization incidents to OSHA. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
Back to Top
Investigator Information
This investigation was conducted by Virgil Casini, Senior Investigator, NIOSH Division of Safety Research, Surveillance and Field Investigation Branch, Fatality Investigations Team.
Diagram
|
|
Diagram. Overhead view of the shoulder-rutting operation.
|