
29-Year-Old Mechanic Electrocuted in Indiana
FACE 86-29
Introduction:
The National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR) is currently conducting the Fatal Accident Circumstances and Epidemiology (FACE) Project, which is focusing primarily upon selected electrical-related and confined space-related fatalities. The purpose of the FACE program is to identify and rank factors that influence the risk of fatal injuries for selected employees.
On May 7, 1986, a 29-year-old class “A” mechanic was electrocuted while assisting the lead mechanic in the maintenance of an electrical distribution system.
Contacts/Activities:
Officials of the Occupational Safety and Health Program for the State of Indiana notified DSR concerning this fatality and requested technical assistance. This case has been included in the FACE Project. On June 25, 1986, the DSR research team (consisting of an industrial hygienist and a safety specialist) met with representatives of the company. The site of this fatality was visited and photographed. Interviews were conducted with surrogates of the fatality victim and co-workers, who perform the same tasks as the victim.
Overview of Employer’s Safety Program:
This is a public electrical utility company that has been in operation for 61 years and employs over 3,000 personnel.
The company consists of five divisions with four generating plants and employs a full-time Safety Director. Managers at each division and all supervisory personnel are held accountable for safety. The company has a written safety policy and safety program which establish safety goals.
Management implements and evaluates safety programs routinely and rewards and communicates effective results (i.e., no lost time injuries, good housekeeping, etc.). Safety rules are established, communicated, and enforced by supervisory personnel. Safety committees, which meet monthly to evaluate safety issues, are comprised of supervisory personnel and company hourly employees.
Synopsis of Events:
On Wednesday morning May 7, 1986, a crew consisting of a foreman, lead class “A” mechanic, and another class “A” mechanic (victim) was assigned to perform maintenance at one of the company’s substations. The maintenance was to include the replacement of a three-way connector. The grounding of the conductors and corresponding switches and breakers was put in place prior to the maintenance on the three-way connector. The foreman, after having discussed and established working procedures with the maintenance crew, moved approximately 150 feet away from the accident site to perform other activities. While preparing to remove the bolts and plates at the three-way connector the lead mechanic and victim were situated in the bucket of an aerial truck approximately 20 feet off the ground. For reasons unknown and without consulting the foreman, the crew moved a ground wire from the original grounded position (lead wire of the coupling cap to a grounded steel structure) to a secondary grounded position (horizontal conductor secured at the three-way connection point, to the grounded steel structure) (see Figure 1image icon). After repositioning the grounding wire to the secondary position the victim began removal of the bolts from the three-way connector. As the bolts were removed, the horizontal conductor with the grounding wire attached separated from the three-way connector; the victim momentarily contacted the grounded horizontal conductor with his left hand and the energized three-way connector with the right hand. This contact created a path-to-ground and the victim was electrocuted.
The victim slumped to the bottom of the aerial bucket breaking contact with the conductor. On site first aid (CPR) was provided within one minute of the accident and paramedics were at the scene providing advanced cardiac life support within six minutes. The victim died at the hospital approximately sixty-five minutes after the accident as a result of cardiac arrest due to electrocution.
Cause of Death:
The coroner reported that the cause of death was cardiac arrest due to electrocution.
Recommendations/Discussion
Recommendation #1: Standard operating procedures and hazard awareness should be routinely presented and reviewed at safety meetings. Employers should enforce strict adherence to company policy.
Discussion: The crew did not adhere to the safe job operating procedure while providing maintenance to the substation. Repositioning of the ground wire is a violation of the safe job operating procedure which contributed to this fatality.
Recommendation #2: A routinely administered hazard awareness identification program should be established to further educate all employees working with electrical energy.
Discussion: For reasons unknown at this time, a grounding wire was repositioned which resulted in this fatality. A better understanding of electrical energy and hazard awareness may have prevented the crew from repositioning the ground wire which contributed to an employee being electrocuted.
The managerial staff of the employer was provided the following documents and overviews:
- Warning – Confined Space! Article by Richard W. Braddee and Ted A. Pettit. Reprinted from Operations Forum (June 1986), Volume 3: 22-23.
- Request for Assistance in Preventing Deaths and Injuries from Excavation Cave-ins (85-110)
- Request for Assistance in Preventing Occupational Fatalities in Confined Spaces (86-110)
- Request for Assistance in Preventing Electrocutions from Contact Between Cranes and Power Lines (85-111)
- Request for Assistance in Preventing Electrocutions of Workers in Fast Food Restaurants (85-104)
- Request for Assistance in Preventing the Injury of Workers by Robots (85-103)
- Request for Assistance in Preventing Hazards in the Use of Water Spray (FOG) Streams to Prevent or Control Ignition of Flammable Atmospheres (85-112)
- Overview of the National Institute for Occupational Safety and Health (NIOSH)
- Overview of the Division of Safety Research (DSR) .
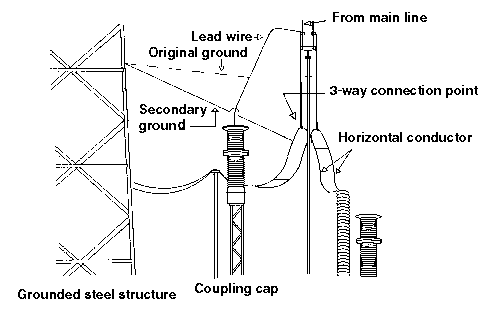
Figure 1.