
19-Year-Old Warehouseman Electrocuted by a 440 Volt Trolley Wire in Kentucky
FACE 85-06
INTRODUCTION:
The National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), is currently conducting the Fatal Accident Circumstances and Epidemiology (FACE) Project, which is focusing upon selected electrically-related fatal injuries and confined space fatalities. By scientifically collecting data from a sample of fatal accidents, the FACE will identify and rank factors which influence the risk of fatal injuries for selected employees.
On December 8, 1984, at approximately 3 p.m., a 19-year-old warehouseman employed by a mine service equipment company was assisting with the removal of a mine machine part from a metal pallet storage rack. The employee climbed approximately nine feet to the top level of the rack. While awaiting the positioning of an overhead bridge crane, he came in contact with both the bare 440 volt runway conductor providing power to the crane and the “grounded” metal rack. After the victim maintained this contact for several seconds, the supervisor de-energized the line. The fatally injured worker fell to the concrete below. The attending coroner concluded that death was due to electrocution.
CONTACTS/ACTIVITIES:
On December 10, 1984, DSR received a request from the State OSHA for technical assistance in evaluating the circumstances surrounding this fatality. On December 11, 1984, a research team consisting of an epidemiologist, a safety specialist, and a consulting engineer conducted a site survey and interviews. The general manager of the facility and co-workers who were present at the time of the accident were interviewed. The county coroner and the parents of the deceased worker were also interviewed. The site survey included video and 35 mm documentation.
SYNOPSIS OF EVENTS:
The company employing the victim started 42 years ago as a family-owned repair shop for coal mine equipment and was recently purchased by a large conglomerate mine service company. Presently, this facility employs a total of 54 people (4 office workers, 42 shop workers, 4 truck drivers, and 4 salesmen). The company is primarily engaged in repairing coal mine machinery, which involves disassembly/assembly of equipment, welding, fabrication, and machining. In addition, support activities include marketing, advertising, transporting, and shipping and receiving.
The victim was hired as a warehouseman two months prior to the accident and had little previous work experience. He worked primarily with two other people (supervisor and inventory control clerk) in shipping and receiving.
The three shipping and receiving personnel were assigned the task of retrieving a mining auger off the top pallet of a storage rack so that it could be shipped to a customer. Other workers were nearby unloading a truckload of furniture at a loading platform. Saturday is not a normal workday. However, there were approximately ten workers in the plant on the day of the accident.
The storage rack was located along the interior wall of the building beneath the overhead bridge crane track and runway conductors (see figure). As shown in the figure, the 3-phase, 440 V conductors were within a few inches of the top of the rack. The pallet and rack arrangement was set up so that a forklift could be used to lift and lower a pallet down to ground level, then the overhead crane could be used to lift and carry the part to its destination. On the day of the accident, the forklift was out of propane fuel, thus necessitating the use of the crane to remove the part from the rack. This usage required a worker (the victim) to climb to the top of the rack, attach a chain to the mining auger (after the crane was moved into position) and attach the chain to the crane hook. At the time of the accident, the crane was being operated by the inventory control clerk.
Shortly after the crane operator warned the victim to be careful and before the supervisor had time to de-energize the lines, the victim contacted the energized line. After de-energization occurred, the victim fell from the top of the metal rack to the concrete floor, a distance of approximately nine feet. Several people unsuccessfully attempted to resuscitate the victim before the Emergency Medical Service (EMS) arrived. The victim was pronounced dead in a hospital emergency room within an hour after the accident.
Inspection of the area around the top pallet provided insight about how the accident might have occurred. The victim was in a squatting position facing towards the back of the plant. The victim was looking in the direction of the moving crane, while trying to maintain his balance on the uneven surfaces of the parts on which his feet rested. His right hand was holding a metal brace of the pallet rack. Finger impressions in the dust on the lower runway conductor showed that his left hand made contact with the lowest bare runway conductor. The path of current flow passed through the victim probably through the unpainted metal lip of the brace he held with his right hand.
GENERAL CONCLUSIONS AND RECOMMENDATIONS:
The contributing factors leading to this electrocution include: a) proximity of the metal pallet rack to bare 440 V conductors; b) lack of visual danger signs in the vicinity of the bare conductors; c) deviation from the usual procedure of using a forklift to move items from the storage rack; and d) insufficient hazard recognition by the victim.
Specific recommendations for prevention include:
1. The pallet storage rack should be removed from the area of the runway conductors.
2. “Danger Voltage” signs should be placed in vicinity of exposed conductors.
3. Guarding should be installed in areas where close worker access to bare runway conductors is necessary.
4. The company should improve their safety training on hazard recognition and safe work practices.
The cooperation and assistance of the State OSHA investigator, plant manager and his employees are greatly appreciated.
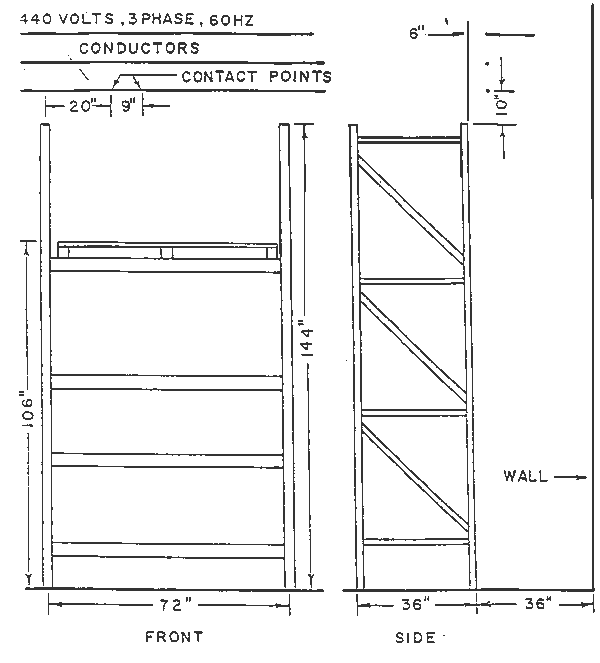
Figure 1.