
38-year-old Stevedore Fatally Injured After Being Struck by the Boom of the Mobile Crane on Site
NIOSH In-house FACE Report 2001-03
Summary

On December 14, 2000, a 38-year-old stevedore (the victim) was fatally injured while working at a river-port materials handling facility after being struck by the boom of the mobile crane on site. The victim and a coworker had been previously lowered from the dock level via a crane-suspended personnel platform, and landed on a barge. After they had disembarked from the personnel platform, the port manager, who was operating the crane, began to hoist it back to the dock. The platform had reportedly been raised about 2 feet when the right-side boom pendant rode out of the boom tip pendant sheave, immediately introducing 200 feet of slack into the boom-hoist system. The slack subsequently caused the boom to fall. The victim apparently observed the boom falling and pushed his coworker aside and out of the way. The boom hit the edge of the dock, broke over the dockside, and struck the victim (Photo 1). The port manager immediately left the crane cab and went to the edge of the dock. Seeing the victim under the boom tip, he contacted another river-port company for assistance. A truck driver who had been waiting on the dock called 911. Emergency medical service personnel and firefighters responded within 7 to 10 minutes. However, the victim died on the scene.
NIOSH investigators concluded that to help prevent similar occurrences employers should
- ensure that examinations are conducted each day prior to placing a crane in service to detect defective operating components or other conditions affecting safe operation
- ensure that idled cranes are positioned to facilitate effective pre-use examinations
- ensure that workers are trained to evaluate the effects of severe weather conditions on facilities and equipment.
Introduction
On December 14, 2001, a 38-year-old stevedore (the victim) at a river-port materials-handling service died after he was struck by the boom tip of a mobile crane. On December 19, 2000, the NIOSH Division of Safety Research (DSR) learned of the occurrence through an internet clipping service. On January 2, 2001, a DSR safety engineer met with the investigating Occupational Safety and Health (OSHA) compliance officer and reviewed the case. On January 3, 2001, the safety engineer traveled to the incident site, examined and photographed the dock and crane, and discussed the case with the company’s vice president of operations and the company safety and compliance officer.
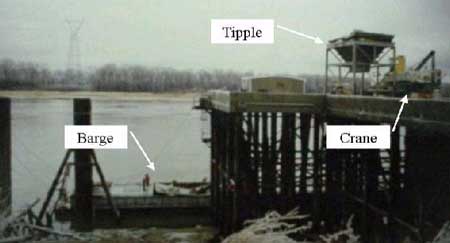
The company was a materials-handling service that had been in business since 1995. The company employed 150 employees in their river terminal division, 11 of whom worked at the incident site, a riverfront gypsum-unloading facility. The facility normally unloaded one barge-load of gypsum per day, using a lattice-boom mobile crane equipped with a clam bucket. The gypsum was transferred from the barge to a tipple for loading into trucks (Photo 2). The company had a full-time safety and compliance officer. The company had a comprehensive written safety program that included formal training for crane operators. The program also included daily, monthly, and annual examination and maintenance of cranes, lifting apparatus, and rigging. Written records of crane examinations were maintained. Personal protective equipment including hard hats, safety shoes, and personal flotation devices were required to be used when working from vessels. Weekly safety meetings were held at the facility. There were eight stevedores working at the facility. This was the company’s first fatality.
Back to Top
Investigation
The mobile crane was equipped with a 100-foot lattice boom and had a maximum capacity of 90 tons. The crane was primarily used with a clam bucket assembly to unload gypsum from the barges, but could also be used for other lifting duties at the facility when needed, including hoisting personnel.
On December 14, 2000, workers at the river-port facility began work at about 6:30 a.m. The weather was cloudy and icy with a temperature of 32 degrees. A major ice storm had struck the area the day before, suspending port operations, and the facility had experienced severe icing conditions on its equipment and travel-ways. The task that day was to unload a barge-load of gypsum that had docked the day before. The dock was about 40 feet above river level. Access from the dock to barges was provided by a vertical ladder protected by a cage-type back guard. Because of the severe ice conditions, the ladder was judged to be unsafe for normal use. The port manager decided to provide worker access to the barge by using a crane-suspended personnel platform. The port manager charged the crane’s battery and chipped ice from the crane’s windshield.
The crane was usually parked at the end of each working day with its boom about 5 feet above the surface of the dock and normal preparations for crane operation included inspection and lubrication with the boom in this position. However, on December 13, after the inspection and servicing had been completed and the crane’s boom had been elevated and readied for work, the ice storm had struck, causing work to be suspended. Because of this, the crane’s boom had been left elevated and since the daily servicing had been done on the 13th and the crane had not been worked, daily servicing was not done on the 14th. After the battery had been sufficiently charged, the crane was started and an attempt to operate it was made. The swing mechanism was not functioning due to ice buildup and the crane was shut down while additional deicing was conducted. Deicer was sprayed on the crane’s swing bands and ice was chipped from the cab lock. These efforts freed the swing mechanism. The personnel platform had been rigged to the crane’s load line. Although not the regular operator, the port manager was an experienced crane operator and he decided to operate the crane on the day of the incident. He assigned the regular operator to remain at the edge of the dock with a radio where he could see the barge deck and relay signals to the port manager in the crane cab. Prior to lifting personnel, a test lift was conducted by hoisting and lowering the personnel platform to the barge. During this lift, the port manager stated that he operated the load line hoist as well as the boom hoist to ensure that the systems were operating correctly.
At about 8:30 a.m., the platform was hoisted to the dock and two stevedores boarded the platform, carrying with them a bag of oil dry for use in improving the footing on the icy barge deck. The workers were hoisted, swung out over the barge, and landed on the barge hatch covers. During the landing, the platform was lowered to within a few feet of the hatch cover using the load line hoist. Then, the platform was landed on the hatch cover by lowering the crane’s boom, as this method provided a gentler landing than could be accomplished using the load line hoist. The two stevedores dismounted from the platform and gave the signal to hoist the platform back to the dock. At this time, they were standing on either side of the platform. The port manager began to hoist the platform by raising the crane boom. A few seconds later, when the personnel platform was only a few feet above the barge, he heard a noise which he thought was ice breaking off and falling from the crane. He stopped booming up and waited about 10 to 15 seconds. He then engaged the boom hoist and immediately heard a pop. Workers on the dock saw the boom pendants fall slack as the crane boom fell, striking the edge of the dock and breaking over the dock side. When the boom fell, the victim pushed his coworker out of the way, placing himself directly in the path of the falling boom, and he was struck and pinned under the boom tip. The port manager then called the regular crane operator stationed on the dock near the edge and told him to check on the stevedores on the barge. The regular crane operator replied that one of the stevedores was under the boom. The port manager left the crane cab to direct initial rescue efforts. A 911 call was made by a truck driver who was on site while the port manager contacted another riverfront company and requested the use of a mobile crane. Emergency medical service personnel and fire fighters responded within 7 to 10 minutes. However, it took several hours to remove the crane boom and recover the victim. He was pronounced dead at the site by the county coroner.
Evidence indicates that as the boom was raised, ice from the top surfaces of the right-side boom pendant collected in the groove of the right-side boom tip pendant sheave. The sheave was equipped with a closely fitted guard to help maintain the rope in the groove (Photo 3). However, there was enough ice buildup to squeeze the rope between the guard and the top of the sheave groove (Photo 4). When this occurred, the entire boom pendant system went slack, allowing the boom to drop (Photo 5). After the incident, the sheave guard was found to have been bent outward from the sheave and the rope had been pinched flat.
Back to Top
Cause of Death
The county coroner established the cause of death as internal injuries.
Recommendations/Discussion
Recommendation #1: Employers should ensure that examinations are conducted each day prior to placing a crane in service to detect defective operating components or other conditions affecting safe operation.
The employer in this facility had implemented a policy of daily examination of the crane for defects that would affect its safe operation. Each morning, before the crane was started and its boom was raised, the crane operator and the maintenance mechanic performed routine servicing and examination. This included lubrication and inspection of the boom tip components. However, on the day of the incident, the boom tip components were not lubricated because on the previous day, shortly after the morning examination and servicing had been completed, work had been suspended. The crane had been parked with the boom angled between 45 and 50 degrees. Since the crane had not been used, workers felt that there was no need for lubrication and the crane was examined with its boom in the raised position. However, as evidenced by the incident, conditions were present at the boom tip pendant sheaves and along the boom pendants that affected safe crane operation.
Recommendation #2: Employers should ensure that idled cranes are positioned to facilitate effective pre-use examinations.
Normal procedure was to park the crane at the end of each working day with the boom lowered. However, as previously noted, the crane had been parked with the boom at an angle of 45 to 50 degrees. At this angle, the boom tip sheaves would be about 70 feet away from the eyes of an examiner. Although the exam was conducted, no defects or adverse conditions were noted. Had the boom been lowered to nearly horizontal as normal, the boom tip would have been more easily observed and the severe icing conditions on the tip sheaves and boom pendant ropes may have been noted and corrected.
Recommendation #3: Employers should ensure that workers are trained to evaluate the effects of severe weather conditions on facilities and equipment.
A severe ice storm had swept through the area on December 13, 2000, forcing the facility to suspend normal operations. On December 14, the facility was in the process of resuming operations after the storm, however, effects of the storm were still present. At the beginning of the work period, the port manager had examined the work areas of the dock and determined that the vertical ladder normally used to access the barge decks from the dock was too severely iced to provide safe access. Since the facility had available the use of a personnel platform, he decided that it would offer the safest means of access to the barge decks. He therefore planned to hoist the victim and coworker from dock to barge via a personnel platform. Once on the barge, the victim and coworker were to determine if the walking surfaces of the barge deck could be made safe. Some of the storm’s effects on the crane and its operation were obvious, such as the ice-covered walking surfaces and the interference of ice buildup with the swing mechanism. However, a less obvious effect was ice buildup on the boom pendant ropes and boom tip pendant sheaves. Had the storm’s effects on the crane been completely recognized, the incident may have been avoided.
Back to Top
Investigator Information
This investigation was conducted by Paul H. Moore, Safety Engineer, Surveillance and Field Investigation Branch, Fatality Assessment and Control Evaluation Team.
Back to Top
Photographs

|
|

|

|

|
|
Photo 5. Crane parked in normal position, after repair.
|