FAQs on Reporting COVID-19 Vaccination Data – April 2024
- Data Reporting: Requirements
- Data Reporting: General
- Data Reporting: Primary Series and Up to Date Vaccination
- Data Reporting: Additional and Booster Doses
- Data Reporting: Healthcare Personnel
- Locations and Enrollment
- Data Reporting: Resources
- Data Reporting: CSV Upload
- Data Reporting: Dialysis Facilities
- Reporting COVID-19 Healthcare Personnel Vaccination Data
- Data Reporting: Long-term Care Facilities
- Data Reporting: Long-term Care Facilities - Optional Reporting of Influenza and Respiratory Syncytial Virus Vaccines
- Person-Level Vaccination Reporting: General
- Person-Level Reporting: Data entry
Data Reporting: Requirements
At this time, only skilled nursing facilities are required to report COVID-19 vaccination data.
Please see the CMS quality reporting program final rule: Federal Register :: Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long-Term Care Hospital Prospective Payment System and Policy Changes and Fiscal Year 2022 Rates; Quality Programs and Medicare Promoting Interoperability Program Requirements for Eligible Hospitals and Critical Access Hospitals; Changes to Medicaid Provider Enrollment; and Changes to the Medicare Shared Savings Program
CMS Skilled Nursing Facilities (SNFs) should also review the final rule: Federal Register :: Medicare and Medicaid Programs; COVID-19 Vaccine Requirements for Long-Term Care (LTC) Facilities and Intermediate Care Facilities for Individuals With Intellectual Disabilities (ICFs-IID) Residents, Clients, and Staff
Please refer to the final rule issued by the Centers for Medicare & Medicaid Services on 8/13/21.
Please refer to the final rule issued by the Centers for Medicare & Medicaid Services on 08/04/21.
Please contact the programs listed below for specific facility types:
- Inpatient quality reporting program (hospitals): CMS Q&A Tool
- PPS-exempt cancer hospital quality reporting program: QRFormsSubmission@hsag.com
- Inpatient psychiatric facility quality reporting program: IPFQualityReporting@hsag.com
- Inpatient rehabilitation facility quality reporting program: questions@cms.hhs.gov
- Long-term acute care quality reporting program: LTCHQualityQuestions@cms.hhs.gov
- Skilled nursing facilities (SNF) QRP HelpDesk: SNFQualityQuestions@cms.hhs.gov
- Ambulatory Surgery Centers: CMS QualityNet Question and Answer Website
- Dialysis facilities: CMS QualityNet Question and Answer Website
NHSN allows for, and encourages, weekly submission of COVID-19 vaccination data via the Weekly COVID-19 Vaccination Module.
Beginning on October 1, 2021, facility types that are part of the CMS Inpatient Quality Reporting Program (or Inpatient Psychiatric Facility Quality Reporting Program, Inpatient Rehabilitation Facility Quality Reporting Program, or Long-term Acute Care Quality Reporting Program) will need to submit COVID-19 vaccination data via the Weekly COVID-19 Vaccination Module for at least one week per month to fulfill CMS reporting requirements.
Facilities can select any week within the month to report data. Facilities may choose to report these data weekly.
COVID-19 vaccination data should be submitted by the end of the quarter as defined by CMS.
A week is designated as belonging to the month of the week-end date. For example, reporting data for the week of September 27 through October 3 is considered as submitting data for a week in October.
Beginning on January 1, 2022, ambulatory surgery centers are required to submit COVID-19 vaccination data via the Weekly COVID-19 Vaccination Module for at least one week per month to fulfill CMS reporting requirements.
The week-end date determines which month a week is included. For example, reporting data for the week of January 31 through February 6 is considered as submitting data for a week in February, not January. This is because the week-end date (February 6) is in February. For facilities that choose to report more than one week per month, the last week of the reporting month will be shared with CMS.
Yes. Reporting COVID-19 vaccination data for HCP the NHSN Healthcare Personnel Safety (HPS) Component will remain required for CMS-certified facilities following the ending of the PHE on May 11, 2023. Facilities required to report data as part of a CMS Quality Reporting Program should continue to report data for at least one week per month for each reporting quarter.
CMS-certified long-term care facilities should continue reporting COVID-19 vaccination data for residents and HCP weekly. Dialysis facilities should report COVID-19 vaccination data for patients and HCP for the last week of each month.
Please see the chart below for information on the upcoming CMS deadlines. Additionally, more guidance can be found here: Healthcare Facility HAI Reporting Requirements to CMS via NHSN Current or Proposed Requirements (cdc.gov) [PDF – 141 KB]
Information on Upcoming CMS deadlines
| Encounter Quarter | Reporting Period | Submission Deadlines |
|---|---|---|
| Q4 2023 | September 25, 2023 – December 31, 2023 | May 15, 2024 |
| Q1 2024 | January 1, 2024 – March 31, 2024 | August 15, 2024 |
| Q2 2024 | April 1, 2024 – June 30, 2024 | November 15, 2024 |
| Q3 2024 | July 1, 2024 – September 29, 2024 | February 18, 2025 |
Yes, facilities can run line list reports to view their data submitted to the weekly COVID-19 Vaccination Cumulative Summary Modules. Using the current reports available in the NHSN application, you should refer to the “All COVID-19 Vaccination Cumulative Summary Data” line listing report to view weekly rates of up to date vaccination coverage. Our website contains quick reference guides on how to run these reports. Resources are listed below.
Follow our How to Run Reports for Long-Term Care Facilities guide: https://www.cdc.gov/nhsn/pdfs/ltc/covidvax/how-to-run-LTC-reports-508.pdf [PDF – 717 KB]
Refer to Quick Reference Guide: Reporting up to date COVID-19 vaccination status through the COVID-19 Vaccination Modules: https://www.cdc.gov/nhsn/pdfs/covid19/quickreferenceguide-uptodateguidance-508.pdf [PDF – 246 KB]
The data dictionary can be used to identify the variables of interest. For example, totSumAllUpToDate is the variable that corresponds with the cumulative number of all HCP in question 1 who are up to date with COVID-19 vaccines. A user can calculate the percent of HCP who are up to date as totSumAllUpToDate/(SumAllHCP – SumAllMedUpToDate) x 100: https://www.cdc.gov/nhsn/xls/covid-19-rpv-public-data-dictionary.xlsx [XLS – 30 KB]
Please keep in mind that the definition of Up to Date may change quarterly based on the latest CDC guidance. You can find the definition for a given reporting quarter here: COVID-19 Vaccination Modules: Understanding Key Terms and Up to Date Vaccination (cdc.gov) [PDF – 114 KB]
Data Reporting: General
Yes, every data field is either required or conditionally required.
Facilities can enter (and edit) data retrospectively; however, they are not required to do so.
Remember that when reporting for any calendar week, report the total number of individuals at the facility for that week.
Then, of these individuals at the facility that week, report the number who have ever received COVID-19 vaccines (at that facility or elsewhere) since they became available in December 2020.
See the FAQs in the section titled Data Reporting: Requirements for information on the timeline for reporting requirements for quality reporting programs.
If there are no changes to your data (for example, there are not any changes in the number of individuals and their vaccination status), then you would report the same numbers as the previously reported week.
Because there could be new staff, residents, and/or patients joining or leaving the facility, vaccination coverage could change week by week even though no new vaccines are given.
Once COVID-19 vaccination data are entered and saved in NHSN, a week cannot be deleted in its entirety.
We highly encourage NHSN application users to enter the appropriate data for the week where data were entered incorrectly.
If you do not have these data available, enter zeros (0) on the data collection form for the incorrect week.
Please note that data can be updated or edited at any time.
For the correct week, you can proceed to enter your COVID-19 vaccination data.
Acceptable forms of documentation include a signed statement or form, or an electronic form or e-mail from the individual indicating when and where they received the COVID-19 vaccine.
A note, receipt, vaccination card, etc. from the outside vaccinating entity stating that the individual received the COVID-19 vaccine at that location is also permitted.
Verbal statements are not acceptable to document vaccination outside the facility for the purposes of NHSN COVID-19 vaccination summary data reporting.
Data Reporting: Primary Series and Up to Date Vaccination
The Novavax COVID-19 vaccine was originally authorized in July 2022 as a 2-dose primary series vaccine by the Food and Drug Administration (FDA). It was formerly administered to individuals 18 years of age and older. The updated 2023-2024 Novavax COVID-19 vaccine was authorized in October 2023 and is now available to individuals 12 years of age and older. For more information on the vaccine, please see the following guidance: Clinical Guidance for COVID-19 Vaccination | CDC
As a result of the FDA’s previous authorization of bivalent vaccines for all doses on April 19, 2023, and the de-authorization of earlier monovalent vaccines, the weekly COVID-19 Vaccination Modules were simplified. Therefore, starting Quarter 3 of 2023, questions about partial primary vaccination series and additional/booster doses were removed across all modules in the Long-term Care Facility Component, Healthcare Personnel Safety Component, and the Dialysis Component.
Beginning Quarter 3 of 2023, questions on COVID-19 vaccination primary series for long-term care facility residents and dialysis patients were removed. Beginning Quarter 1 of 2024, these questions have also been removed for facilities submitting healthcare personnel data through the Long-term Care Facility Component and Healthcare Personnel Safety Component.
For healthcare personnel reporting between June 26, 2023 – December 31, 2023, a complete primary series is defined as receiving:
- A 2-dose series of a monovalent COVID-19 vaccine
- A single dose of Janssen COVID-19 vaccine
- A single dose of bivalent COVID-19 vaccine
- Beginning on September 25, 2023, a single dose of 2023-2024 updated COVID-19 vaccine
Please note that beginning January 1, 2024, the primary series question has been removed for healthcare personnel reporting forms across all components.
For further guidance on the definition of up to date, please review COVID-19 Vaccination Modules: Understanding Key Terms and Up to Date Vaccination [PDF – 672 KB].
Please refer to the CDC NHSN COVID-19 Vaccination Modules: Understanding Key Terms and Up to Date Vaccination [PDF – 672 KB] at least once per quarter. This document contains the current definition of up to date and example scenarios. Definitions and examples from prior quarters are also included. Always report vaccination data according to the definitions corresponding to the week you are reporting data for. For example, if you need to go back and report or modify data for the week of August 7-13, 2023, you will use the definition of up to date that was in place for Quarter 3 2023 (June 26, 2023 – September 24, 2023).
The latest information on medical contraindications may be found in Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States.
For NHSN COVID-19 vaccination surveillance, philosophical, religious, or other reasons for declining COVID-19 vaccine not listed as a medical contraindication in the Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States are not considered medical contraindications for COVID-19 vaccination and should be reported under question 3.2, offered but declined COVID-19 vaccine.
If a facility is not able to obtain information on medical contraindications, then the facility can enter a zero (0) in the NHSN application for this question.
Starting on June 26, 2023 for the LTC residents and dialysis patients forms and January 1, 2024 for the LTC and HPS healthcare personnel forms, question 3.1 pertains to a medical contraindication preventing an individual from obtaining the latest recommended COVID-19 vaccine necessary to be considered up to date with COVID-19 vaccination.
Prior to January 1, 2024, question 3.1 on the LTC and HPS healthcare personnel forms pertains to a medical contraindication preventing an individual from obtaining the COVID-19 vaccine necessary to complete COVID-19 vaccination primary series.
Starting on June 26, 2023 for LTC residents and dialysis patients and January 1, 2024 for LTC and HPS healthcare personnel, they should be categorized in question 3.1 as having a medical contraindication preventing them from being up to date with COVID-19 vaccination due to their severe allergic reaction after a monovalent dose.
Prior to January 1, 2024 for LTC and HPS healthcare personnel, they should be categorized in question 3.1 as having a medical contraindication preventing them from obtaining complete primary COVID-19 vaccine series due to their severe allergic reaction after a previous dose of COVID-19 vaccine.
LTC and HPS Healthcare Personnel: For reporting weeks between September 25, 2023 to December 31, 2023, the individual should be counted in question #2 (complete primary series), as receiving one bivalent dose of COVID-19 vaccine which is defined as having received complete primary series. For reporting weeks starting on January 1, 2024 and onward, the individual should be counted in question 3.2 (offered but declined COVID-19 vaccine), as they have declined the latest COVID-19 vaccine needed to be considered up to date.
LTC Residents/Dialysis Patients: For reporting weeks starting on September 25, 2023 and onward, the individual should be counted in question 3.2 (offered but declined COVID-19 vaccine), as they have declined the latest COVID-19 vaccine needed to be considered up to date.
An individual who declines to receive vaccination for any reason other than the medical contraindications listed in Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States should be categorized as declined to receive COVID-19 vaccination for question 3.2.
This is true even if your facility permits religious or philosophical exemptions for COVID-19 vaccination.
If individuals cannot provide any documentation of vaccination, they should be reported in question 3.3 under “Unknown/other COVID-19 Vaccination Status.”
If an individual has not received any doses of COVID-19 vaccine, but would like to be vaccinated, they should be reported in question 3.3 under “Unknown/other COVID-19 Vaccination Status.”
For example, if an individual stated that they have not had an opportunity to receive the vaccine but wishes to do so, they would be counted as “unknown/other”.
In addition, if an individual cannot produce documentation of COVID-19 vaccines received outside of the healthcare facility, they would be counted as “unknown/other.”
Alternatively, if an individual states he/she has not received any COVID-19 vaccines and does not intend to do so, they are reported in question 3.2 under “Offered but declined COVID-19 vaccine.”
Please report these individuals in question 3.3 under “Unknown/other COVID-19 Vaccination Status.”
Data Reporting: Additional and Booster Doses
The primary COVID-19 vaccine series received by an individual since December 2020 includes dose 1 and dose 2 of COVID-19 vaccines requiring two doses for completion or one dose of COVID-19 vaccine requiring only one dose for completion.
The additional dose or booster is received at least two weeks or more after completing a primary vaccine series.
Please note that beginning in Quarter 3 2023, the additional and booster dose questions were removed across all vaccination modules in the Long-term Care Facility Component, Healthcare Personnel Safety Component, and the Dialysis Component.
As a result of the April 19, 2023 FDA authorization of bivalent vaccines for all doses, and the de-authorization of monovalent vaccines, the weekly COVID-19 Vaccination Modules were simplified. Therefore, questions about additional, and booster doses were removed across all modules in the Long-term Care Facility Component, Healthcare Personnel Safety Component, and the Dialysis Component for reporting weeks beginning with quarter 3 of 2023.
An additional dose is a subsequent dose of vaccine administered to people who are less likely to mount a protective immune response after initial vaccination.
People who are moderately or severely immunocompromised and who received Janssen COVID-19 Vaccine for their primary series should receive an additional dose.
A bivalent COVID-19 vaccine includes a component of the original virus strain and a component of the omicron variant. These are called bivalent COVID-19 vaccines because they contain these two components. A monovalent COVID-19 vaccine only contains a component of the original virus strain.
Beginning in Quarter 3 2023, additional and booster dose questions were removed across all vaccination modules in the Long-term Care Facility Component, Healthcare Personnel Safety Component, and the Dialysis Component.
During weeks prior to July 2023, facilities reported the cumulative number of individuals with complete primary series vaccine in question 2.2 who have received any booster(s) or additional dose(s) of COVID-19 vaccine since August 2021 in the COVID-19 Vaccination Modules. For information on how to enter data for booster and additional doses for COVID-19 Vaccination Modules prior to July 2023, please see the Table of Instructions for the HCP, LTC, and Dialysis modules.
Facilities should refer to CDC’s Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States to determine individuals who are eligible to receive additional doses s after receiving a complete primary vaccination series.
Please note that beginning in Quarter 3 2023, the additional and booster dose questions were removed across all vaccination modules in the Long-term Care Facility Component, Healthcare Personnel Safety Component, and the Dialysis Component.
Individuals are only counted for the doses they receive. The facility would count this staff member under question 2.1 (Only 1 dose of a two-dose Primary COVID-19 vaccine series). The facility would not include the staff member in questions on additional or booster doses at this time. This individual also would not be counted under question 5 since they are not considered up to date.
Please note that beginning in Quarter 3 2023 (the week of June 26, 2023 – July 2, 2023), HCP who receive a single monovalent dose are counted in question 3.3 as other/unknown vaccination status. This is because the partial primary series question was removed from the form beginning in Quarter 3 2023.
NHSN’s surveillance definition of up to date for COVID-19 vaccination data is based on CDC’s clinical considerations and up to date definition for the first day of the reporting quarter.
NHSN surveillance definitions are designed to assess trends in the population and inform public health response.
NHSN must be able to standardize criteria and apply these definitions in a consistent manner; therefore, for the purpose of surveillance tracking, the NHSN surveillance definition must remain stable for a reporting quarter and will not be updated until the following quarter even if CDC’s clinical considerations and up to date definition change.
Please refer to COVID-19 Vaccination Modules: Understanding Key Terms [PDF – 212KB] for definitions of key terms and up to date vaccination related to COVID-19 vaccination for the purpose of NHSN public health surveillance.
NHSN’s surveillance definition of up to date for COVID-19 vaccination data is based on CDC’s clinical considerations and up to date definition for the first day of the reporting quarter.
During Quarter 3 2022 (June 27, 2022 – September 25, 2022) and Quarter 2 2024 (April 1, 2024 – June 30, 2024), the NHSN surveillance definition of up to date vaccination status is different for individuals based on age.
For all other reporting quarters, the NHSN surveillance definition of up to date vaccination status is the same for all individuals regardless of age.
Please see more here: COVID-19 Vaccination Modules: Understanding Key Terms and Up to Date Vaccination [PDF – 200 KB].
Remember to always refer to the up to date definition associated with the calendar week for which you are reporting data.
NHSN’s surveillance definition of up to date for COVID-19 vaccination data is based on CDC’s clinical considerations and up to date definition for the first day of the reporting quarter. To avoid discrepancies in data reporting within quarters, the new definition is applied starting with the new quarter even if the definition guidelines were announced mid-way through the previous quarter.
Please refer to COVID-19 Vaccination Modules: Understanding Key Terms [PDF – 212 KB] for definitions of key terms related to COVID-19 vaccination for the purpose of NHSN public health surveillance.
Data Reporting: Healthcare Personnel
Facilities should report COVID-19 vaccination data on healthcare personnel who were eligible to have worked at this healthcare facility for at least 1 day during the week of data collection, regardless of clinical responsibility or patient contact.
To save a data record in the NHSN application, facilities must enter data on four categories of healthcare personnel: employees, licensed independent practitioners (non-employee physicians, advanced practice nurses, and physician assistants), adult students/trainees and volunteers aged 18 and over, and other contract personnel.
Healthcare personnel eligible to have worked include those scheduled to work in the facility at least one day every week.
For example, an employee who is scheduled to work in the facility every Monday would be included in the data.
However, an employee who is scheduled to work in the facility once a month would not be included in the data.
Working any part of a day is considered as working one day.
Facilities should include healthcare personnel even if they are on temporary leave during the week of data collection.
Temporary leave is defined as less than or equal to two weeks in duration.
If they are on leave that is greater than two weeks, then they should not be included for the week of data collection.
Advanced practice nurses include nurse practitioners, nurse midwives, clinical nurse specialists, and nurse anesthetists.
Advanced practice nurses paid through a contract should be reported in the licensed independent practitioner category.
However, advanced practice nurses who are employees of the facility should be reported under employees (staff on payroll).
Please note that travel nurses should be included under ‘other contract personnel’ if they are not considered advanced practice nurses and are paid through a contract.
Ambulance workers who physically perform work duties inside the facility (such as patient transporters) and who are eligible to have worked at the facility for at least 1 day during the week of data collection would be included (under the other contract personnel category if they are paid through a contract or vendor, or under the employee category if they are directly employed by the facility).
However, ambulance drivers who do not physically work inside the facility on a regular, weekly basis would not be included.
Yes, vendors providing care, treatment, or services should be included in the other contract personnel category if they work in the facility on a regular (weekly) basis, regardless of clinical responsibility or patient contact.
The list below includes examples of contracted and vendor HCP who provide direct patient care and who perform non-direct or non-patient care duties. This list is not exhaustive.
Contracted and vendor HCP can include the following non-employee care providers who may or may not be involved in patient care:
- Admitting staff/clerical support/registrars
- Agency nurses
- Ambulance drivers (who enter the facility to assist with transportation)
- Biomedical engineers
- Central supply staff
- Chaplains
- Construction workers (working inside the facility)
- Dietary/food service staff
- Dieticians
- Dialysis technicians
- EKG technicians
- EMG technicians
- Home health aides
- Housekeeping staff
- Information Technology staff
- Laboratory: Phlebotomists
- Laboratory: Technicians
- Landscapers (working inside the facility)
- Laundry staff
- Maintenance staff/engineers
- Nursing aides
- Occupational therapists
- Patient care technicians
- Patient transporters
- Pharmacists
- Pharmacy/medication technicians
- Physical therapists
- Psychologists
- Psychology technicians/Mental health workers
- Radiology: X-ray technicians
- Recreational therapists/Music therapists
- Respiratory therapists
- Security staff
- Social workers/Case managers
- Speech therapists
- Surgical technicians
- Traveling nurses
- Ultrasound technicians
- Utilization review nurses
You should count healthcare personnel who are eligible to work at the facility, regardless of clinical responsibility or patient contact.
For example, you should count healthcare personnel having official responsibilities in the facility such as attending regularly scheduled meetings or required training.
However, you would not need to count healthcare personnel who are not officially in the facility for work duties (e.g., coming into the facility for lunch) during the reporting period.
No. Only healthcare personnel who are eligible to physically work at the healthcare facility are included.
Facilities should include healthcare personnel if they are on temporary leave during the week of data collection.
Temporary leave is defined as less than or equal to 2 weeks in duration.
Examples of temporary leave may include sick leave or vacation.
In instances where temporary leave extends past 2 weeks, the healthcare worker should not be included in question 1 for the current week of data collection.
Therefore, facilities would include an individual who was on sick leave for 3 days during the week.
However, an individual on maternity leave for 2 months would not be included in the data.
Yes. These reports describe vaccination rates among individuals working at a specific facility, so all eligible individuals must be counted at each facility where they work during the week of data collection.
Please include healthcare personnel who were eligible to have worked at this healthcare facility for at least 1 day during the week of data collection, regardless of clinical responsibility or patient contact.
For example, if an individual worked at the facility from Monday through Thursday but was terminated on Friday of the current reporting week, you would still include the individual in the data for the current reporting week.
However, you would remove the individual from your data for subsequent reporting weeks.
Locations and Enrollment
If the facilities are physically separate buildings from each other, whether on the same property or over multiple campuses, then they should be enrolled separately in NHSN.
Each facility should have its own, unique NHSN OrgID.
When a CCN is shared across multiple facilities, the CDC will aggregate the data from all applicable NHSN OrgIDs and will send to CMS under the single CCN for CMS reporting purposes.
Each distinct OrgID should monitor and report COVID-19 vaccination separately, for the purposes of accurate tracking, public health surveillance, and analysis.
Please read more on the How Facilities Report [PDF – 250 KB].
Facilities should follow the guidance below when making determinations about which areas of the acute care facility to include when reporting healthcare personnel COVID-19 vaccination summary data to NHSN as part of the CMS Hospital Inpatient Quality Reporting (IQR) Program:
- Include all inpatient units/departments located within the acute care facility building and sharing the exact same CMS Certification Number [CCN] (100% identical) as the acute care facility. This includes any inpatient rehabilitation ward and inpatient behavioral ward that are not CMS-certified and do not have their own CCN.
Example 1: Rehabilitation ward within the acute care facility building that shares the same CCN as the acute care facility
- A rehabilitation ward is not a CMS-certified inpatient rehabilitation facility (IRF) unit and has a CCN of 337766.
- Acute care facility has a CCN of 337766.
- The ward resides within the walls of the acute care facility.
Guidance: Since the rehabilitation ward and acute care facility share the same CCN and are located in the same building, the data for the Enrollment and Reporting for Physically Separate Facilities/Units rehabilitation ward should be combined with the data for the acute care facility and reported through one OrgID.
Include all outpatient units/departments located within the acute care facility building that share the exact same CCN (100% identical) as the acute care facility.
Example 2: Outpatient department located within the acute care facility building and shares the same CCN as the acute care facility
- An outpatient radiology imaging department has a CCN of 441122.
- Acute care facility has a CCN of 441122.
- The facilities are located in the same building.
Guidance: Since the radiology imaging department and acute care facility share the same CCN and are located in the same building, the data for this department should be combined with the data for the acute care facility and reported through one OrgID.
If an inpatient or outpatient unit/department of the acute care facility has a different CCN (even if different by only one letter or number) from the acute care facility (such as a CMS-certified inpatient psychiatric unit or inpatient rehabilitation facility), then the CMS-certified unit should be mapped as a unit in the acute care facility and report its data separately.
The unit will share the same OrgID as the acute care hospital, but it will have a separate record reported to NHSN (under its unique CCN and mapped vaccine location).
Example 3: Inpatient unit within the acute care facility building with a different CCN from the acute care facility.
- An inpatient behavioral ward that is CMS-certified as an inpatient psychiatric facility (IPF) unit and has a CCN of 55S688 (this unit is located within the acute care facility).
- Acute care facility has a CCN of 556688.
- The facilities are located in the same physical building.
Guidance: The IPF unit should be mapped as unit in the acute care facility in NHSN. Since the IPF unit has a different CCN from the acute care facility, the data for this unit should be reported under the acute care facility NHSN OrgID, but with a separate IPF unit weekly vaccination record.
Facilities can learn more about this topic here: Guidance on Enrollment and Reporting for Physically Separate Facilities/Units* in NHSN (cdc.gov) [PDF – 233KB]
IPF units do not need to enroll or activate the Healthcare Personnel Safety (HPS) Component unless their affiliated acute care or critical access facility is not already enrolled in NHSN or the IPF unit is not physically located within the walls of the affiliated acute care or critical access facility.
IPF units located within hospitals can simply be mapped as locations of the already-enrolled acute care or critical access facility.
Once the IPF unit is added as a location of the facility, the IPF unit-specific CCN is linked with that location, and its data should be reported separately.
View more information about how to map an IPF unit and add an IPF unit-specific CCN [PDF – 200 KB].
If an inpatient or outpatient unit/department of the acute care facility has a different CCN (even if different by only one letter or number) from the acute care facility (such as a CMS-certified inpatient psychiatric unit or inpatient rehabilitation facility), then the CMS-certified unit should be mapped as a unit in the acute care facility and report its data separately.
The unit will share the same OrgID as the acute care hospital, but it will have a separate record reported to NHSN (under its unique CCN and vaccine location).
Exception: swing beds that reside in their own unit should be reported with the acute care hospital.
View more information about how to map an IPF unit and add an IPF unit-specific CCN [PDF – 200 KB].
View more information about how to add an IRF unit as a location in your facility [PDF – 500 KB].
Yes. IRF, IPF and hospital data can all be uploaded in one .CSV file.
No.
If the IRF or IPF unit CCN is 100% identical to the CCN of its acute care or critical access facility, then separate healthcare personnel COVID-19 vaccination summary data reporting is not required by CMS.
Therefore, counts of healthcare personnel working in the IRF or IPF unit can be included in the total counts for the acute care or critical access facility.
However, IRF or IPF units whose CCNs differ from the acute care or critical access facility CCN by even one letter or number – for example, having a “T” or “R” in the third position – must either be mapped as locations of the parent facility or enrolled as a separate NHSN facility, and their data must be reported separately.
Data Reporting: Resources
NHSN has developed many resources for facilities. Facilities can visit the following webpage to access training materials on reporting COVID-19 vaccination data through NHSN:
- Long-term care facilities reporting data on healthcare personnel and residents
- Non-long-term care facilities reporting data on healthcare personnel
- Dialysis facilities reporting data on patients
These webpages contain data collection forms, tables of instructions for reporting data, training slides, reporting and analysis guides, data tracking worksheets and .CSV file templates and instructions.
All facilities can submit COVID-19 vaccination data through NHSN using the COVID-19 Cumulative Vaccination Summary Form. Entering COVID-19 vaccination data into the COVID-19 Cumulative Vaccination Summary Form can be done in two ways:
- Direct data entry into the COVID-19 Cumulative Vaccination Summary Form
- CSV file upload into the COVID-19 Cumulative Vaccination Summary Form
The .CSV file templates and instructions for uploading COVID-19 vaccination data can be found under the “CSV Data Import” section of the following webpages:
- Long-term care facilities reporting data on healthcare personnel and residents
- Non-long-term care facilities reporting data on healthcare personnel
- Dialysis facilities reporting data on patients
Long-term care facilities and facilities that report COVID-19 vaccination data in the Healthcare Personnel Safety (HPS) Component can also submit data using the Person-Level COVID-19 Vaccination Forms. These forms are enhanced versions of the Excel documents that have previously been used to submit data. Entering COVID-19 vaccination data into the Person-Level COVID-19 Vaccination Forms can be done in two ways:
- Direct data entry into the Person-Level COVID-19 Vaccination Form
- CSV file upload into the Person-Level COVID-19 Vaccination Form
For more information on how to submit data using the COVID-19 Cumulative Vaccination Summary Form or the Person-Level COVID-19 Vaccination Form, please see the following webpages:
Facilities are encouraged to report data through NHSN (in addition to any other data reporting systems) because NHSN collects COVID-19 vaccination data at the facility-level.
Most state Immunization Information Systems do not include the information needed to determine if an immunized person is a resident of a nursing home, a dialysis patient, or a healthcare worker.
Using the NHSN COVID-19 Vaccination Modules allows tracking vaccination coverage among the residents, patients, or healthcare personnel in your facilities.
Please use NHSN-ServiceNow to submit questions to the NHSN Help Desk. Please use NHSN-ServiceNow to submit questions to the NHSN Help Desk. This link should be used in place of nhsn@cdc.gov, nhsntrain@cdc.gov, and nhsndua@cdc.gov. ServiceNow will help the NHSN team respond to your questions faster. Users will be authenticated using CDC’s Secure Access Management Services (SAMS), the same way you access NHSN. If you do not have a SAMS login, or are unable to access ServiceNow, you can still e-mail the NHSN Help Desk at nhsn@cdc.gov.
Data Reporting: CSV Upload
We recommend uploading files with a maximum of 500 rows to enable successful file upload for facilities submitting COVID-19 vaccination data through large .CSV files.
The .csv upload has an alert built into the reporting grid to show a message that indicates when the upload is successful.
NHSN will automatically populate the uploaded data. If errors are found during upload, a window displaying a description of these errors will be generated.
Data Reporting: Dialysis Facilities
The Centers for Medicare and Medicaid Services’ (CMS) End Stage Renal Disease (ESRD) Network program established COVID-19 vaccination reporting requirements beginning March 2021.
Since data reporting requirements are established by the ESRD Network program, we recommend that you contact your ESRD Network.
Your ESRD Network will be able to provide you with the relevant information on reporting COVID-19 vaccination data through NHSN for healthcare personnel and patients of dialysis facilities.
Each calendar week begins on a Wednesday and ends on a Tuesday for patients. Reporting weeks for staff are Monday-Sunday.
You would include all patients receiving dialysis care from the facility during the week of reporting, whether they received care at the facility or at home.
Home dialysis patients include those receiving hemodialysis and peritoneal dialysis at home.
If a patient receives care from the dialysis facility for multiple weeks, you should count the patient for each week the patient receives care.
For example, if a patient received care from the dialysis facility for five weeks, you would include the patient in the facility’s data for each of the five weeks.
Yes, if the patient received care in the facility for at least 1 day during the reporting week, they would be counted in question 1 on the data collection form for the current week.
However, these patients would not be included in data reporting for subsequent weeks.
Please include patients treated by your outpatient dialysis facility at least 1 day during the reporting week.
If a patient only received dialysis care during a hospitalization you should not report data for that patient.
However, if a patient was hospitalized during the week and was also treated by your dialysis facility at least 1 day during the reporting week, then you should report data for that patient.
Please include all patients who received dialysis care from the facility during the week, including those with chronic or acute conditions.
If healthcare personnel were eligible to have worked in hospital and dialysis facility, each facility should include the personnel in their data.
NHSN users can belong to multiple groups.
Users should be sure they are uploading and/or viewing COVID-19 vaccination data for the correct group in NHSN.
Users should be logged into the Healthcare Personnel Safety Component for uploading and/or viewing COVID-19 vaccination data for healthcare personnel.
The Dialysis Component should be used for uploading and/or viewing COVID-19 vaccination data for patients.
Please note that a facility should decide which of the groups that it has granted access to NHSN for the purpose of viewing their data will upload their data as these same groups will also have access to upload data on their behalf using the .CSV bulk upload process.
If data have been uploaded into NHSN for a facility by one group or supergroup via the .csv bulk upload, these data can be overwritten by a second group uploading data for the facility at a later time or date.
Therefore, NHSN recommends that facilities only grant access to one group/supergroup to upload data on their behalf.
Groups or supergroups can include health departments.
It is also important to note that if a facility has entered its own data, it will not be overwritten by a bulk upload by a group/supergroup. It should also be noted that in this instance, in contrast to a group upload, the facility can overwrite its previously uploaded data.
Reporting of COVID-19 vaccination among patients and staff will remain required after May 11, 2023. Dialysis facilities should continue reporting to NHSN’s Patient COVID-19 Vaccination and Healthcare Personnel COVID-19 Vaccination modules. However, after May 11, 2023, facilities only need to report COVID-19 vaccination data for patients and staff for the last week of each month.
As a reminder, a week is designated as belonging to the month that contains the week-end date. For example, the week of May 29, 2023 – June 4, 2023 counts as reporting for a week in June. For both staff and patients, data from the prior month are due on the Friday of the first full business week of each month.
| Patients Reporting Week | Staff Reporting Week | Due Date |
|---|---|---|
| 5/24/2023-5/30/2023 | 5/22/2023-5/28/23 | Friday June 9, 2023 |
| 6/21/2023-6/27/2023 | 6/19/2023-6/25/2023 | Friday July 7, 2023 |
| 7/19/2023- 7/25/2023 | 7/24/2023-7/30/2023 | Friday August 11, 2023 |
| 8/23/2023-8/29/2023 | 8/21/2023-8/27/2023 | Friday September 8, 2023 |
| 9/20/2023-9/26/2023 | 9/18/2023-9/24/2023 | Friday October 6, 2023 |
| 10/25/2023-10/31/2023 | 10/23/2023-10/29/2023 | Friday November 10, 2023 |
| 11/22/2023-11/28/2023 | 11/20/2023-11/26/2023 | Friday December 8, 2023 |
| 12/20/2023-12/26/2023 | 12/25/2023-12/31/2023 | Friday January 5, 2023 |
| 1/24/2024-1/30/2024 | 1/22/2024-1/28/2024 | Friday February 9, 2024 |
| 2/21/2024-2/27/2024 | 2/19/2024-2/25/2024 | Friday March 8, 2024 |
| 3/20/2024-3/26/2024 | 3/25/2024-3/31/2024 | Friday April 5, 2024 |
| 4/24/2024-4/30/2024 | 4/22/2024-4/28/2024 | Friday May 10, 2024 |
| 5/22/2024-5/28/2024 | 5/20/2024-5/26/2024 | Friday June 7, 2024 |
| 6/19/2024-6/25/2024 | 6/24/2024-6/30/2024 | Friday July 5, 2024 |
| 7/24/2024-7/30/2024 | 7/22/2024-7/28/2024 | Friday August 9, 2024 |
| 8/21/2024-8/27/2024 | 8/19/2024-8/25/2024 | Friday September 6, 2024 |
| 9/18/2024-9/24/2024 | 9/23/2024-9/29/2024 | Friday October 11, 2024 |
| 10/23/2024-10/29/2024 | 10/21/2024-10/27/2024 | Friday November 8, 2024 |
| 11/20/2024-11/26/2024 | 11/18/2024-11/24/2024 | Friday December 6, 2024 |
| 12/25/2024-12/31/2024 | 12/23/2024-12/29/2024 | Friday January 10, 2025 |
Reporting COVID-19 Healthcare Personnel Vaccination Data
Facilities can find the exact language of the applicable CMS Reporting Program on the CMS website using the links below:
- CMS Hospital Inpatient Quality Reporting Program (IQR)
- CMS Hospital Outpatient Quality Reporting Program (OQR)
- CMS Long Term Care Quality Reporting Program (LTCHQR)
- CMS Inpatient Rehabilitation Facility Quality Reporting Program (IRFQR)
- CMS End Stage Renal Disease (ESRD) Quality Incentive Program (QIP)
- CMS PPS-Exempt Cancer Hospital Quality Reporting Program (PCHQR)
- CMS Ambulatory Surgical Center Quality Reporting Program
- CMS Inpatient Psychiatric Facility Quality Reporting Program (IPFQR)
CMS provides CDC with a list of CMS certification number (CCNs) from which they expect to receive data for required reporting.
CDC then takes that list and extracts the appropriate data from each NHSN facility for CCNs on the CMS list.
Data are ‘frozen’ at midnight on the day of the reporting deadline, and CDC sends data to CMS according to CCN the next business day.
Please contact the programs listed below for specific facility types:
- Ambulatory Surgery Centers: CMS QualityNet Question and Answer Website
- Dialysis: CMS QualityNet Question and Answer Website
- Inpatient quality reporting program (hospitals): CMS Q&A Tool
- PPS-exempt cancer hospital quality reporting program: QRFormsSubmission@hsag.com
- Inpatient psychiatric facility quality reporting program: IPFQualityReporting@hsag.com
- Inpatient rehabilitation facility quality reporting program: questions@cms.hhs.gov
- Long-term acute care quality reporting program: LTCHQualityQuestions@cms.hhs.gov
- Skilled nursing facilities (SNF) QRP HelpDesk: SNFQualityQuestions@cms.hhs.gov
Healthcare personnel (HCP) COVID-19 vaccination summary data submitted to NHSN will be reported by CDC to CMS for each facility by CMS Certification Number (CCN).
For facilities that report more than one week per month, data from the last week of the reporting month will be shared with CMS.
CDC will provide a HCP COVID-19 vaccination percentage for each reporting CCN.
Each quarter, CDC will calculate the quarterly HCP COVID-19 vaccination coverage rates for each CCN, by taking the average of the data from the three weekly rates submitted by the facility for that quarter.
This calculation includes data from the core HCP categories of employees, licensed independent practitioners, and adult students/trainees and volunteers who completed a COVID-19 vaccination course.
HCP with NHSN-defined medical contraindications to COVID-19 vaccination are excluded from the denominator.
Tips for submitting COVID-19 vaccination data can be found in the Tips for Submitting Healthcare Personnel (HCP) COVID-19 Vaccination Data [PDF – 249KB]
Review the “COVID-19 Weekly Vaccination Summary” Form that can accessed by clicking on “Vaccination Summary” on the left-hand navigation bar in NHSN.
For complete reporting instructions see: 57.149 Instructions for Completion of the Weekly Healthcare Personnel Vaccination Summary Form Non-LTCF HCP (cdc.gov) [PDF – 287 KB].
Click “save” after any changes are made to data.
Instructions on how to run a line list report to verify multiple weeks of saved data are available: Weekly COVID-19 Vaccination Reporting – Inpatient Facility – January 2022 [PDF – 580KB].
Yes, these checks are described in detail in the following resources, COVID-19 Vaccination Quick Reference Guides in Response to Monthly Combined Data Quality [PDF – 1MB] and Data Quality Alert – July 2021. [PDF – 293KB]
Data Reporting: Long-term Care Facilities
Long-term care facilities can currently access the NHSN Weekly COVID-19 Vaccination Modules with Level 1 SAMS access.
However, Level 1 access is an interim measure with limited access to the NHSN application.
NHSN continues to encourage facilities to obtain Level 3 access once Level 1 registration is completed.
The difference between Level 3 and Level 1 is data security safeguards, as Level 3 provides a more secure data upload.
If your facility does not have a Level 3 user, please contact the SAMS Help Desk between the hours of 8:00 AM and 8:00 PM EST Monday through Friday (excepting U.S. Federal holidays) at the following:
- Toll Free: 877-681-2901
- E-mail: samshelp@cdc.gov
You can also find additional information in the SAMS User FAQs published on the SAMS Homepage at https://sams.cdc.gov
Please note that users with level 1 SAMS access will be unable to use the new optional event-level (person-level) COVID-19 vaccination forms to summarize and submit data to the Weekly COVID-19 Vaccination modules.
For more information on how enroll a facility, please go to Enrollment for Long-term Care Facilities.
COVID-19 vaccination data for healthcare personnel and residents is to be reported to NHSN each calendar week and must represent data for each standard week, which is Monday through Sunday.
For example, vaccination data for the week of Monday, 5/10/2021 through Sunday, 5/16/2021 can be reported to NHSN during the following week (5/17/2021-5/23/2021).
As another example, a nursing home reports COVID-19 vaccination data to NHSN every Wednesday.
Data reported on Wednesday, May 26 represented vaccination data for the previous standard week of Monday, May 17 through Sunday, May 23.
Data may also be reported during the current standard week if preferred. Data may be updated at any time.
Additional specific questions related to CMS reporting requirements for long-term care facilities and data submission deadlines should be sent to the following e-mail box: DNH_TriageTeam@cms.hhs.gov.
Newly added question 4.1 and question 4.2 ask the user to report the cumulative number of residents that received both only one booster dose question 4.1) and two more booster doses (question 4.2).
In the above scenario, the individual would be counted in question 2, as having received a complete primary dose, question 4, as having received any additional booster and question 4.2, as having received two or more boosters.
Additionally, based on the current CDC guidance, they would be included in question 5, up to date.
Please include residents occupying a bed at the facility for at least 1 day (at least 24 hours) during the week of data collection.
For example, if a resident stayed at a facility for two days during the current reporting week but was then discharged, you would still include the resident in the data for the current reporting week.
However, you would remove the resident from your data for subsequent reporting weeks.
Pharmacies and other vaccinating organizations are not reporting COVID-19 vaccination data to NHSN, so it is important for long-term care facilities to report these data to NHSN.
Data Reporting: Long-term Care Facilities - Optional Reporting of Influenza and Respiratory Syncytial Virus Vaccines
Reporting Influenza and RSV vaccination data to the NHSN Respiratory Pathogens Vaccination Module is optional. If long-term care facilities choose to report Influenza and RSV vaccination data to the NHSN Respiratory Pathogens Vaccination Module, data can only be reported for residents of the long-term care facility. Participating facilities that choose to report Influenza and RSV vaccination data must report their data using the NHSN definitions outlined in the 2023 Respiratory Pathogens Vaccination Protocol [PDF – 414 KB] to ensure data are uniformly reported across facilities.
The Influenza and RSV vaccination summary data forms are set up to be reported on a weekly basis. Users can choose how often and which weeks to report Influenza/RSV vaccine data. Ideally, it would be reported in same “weekly” cadence as COVID-19 vaccines. A reporting week in NHSN is defined as beginning on a Monday and ending on a Sunday. Additionally, a reporting week is designated as belonging to the month of the week-end date. For example, reporting data for the week of September 25 through October 1 is considered as submitting data for a week in October.
Influenza and RSV vaccination data can be reported in the optional weekly Resident Flu/RSV Cumulative Vaccination Summary for Long-Term Care Facilities [PDF – 182 KB] form in NHSN. To find this form within the NHSN application, please hover to the “COVID-19/Respiratory Pathogens” tab found on the left-side menu of the NHSN homepage, and click on “Vaccination – Residents.” From the Weekly Vaccination Calendar view, each reporting week will have three tabs:
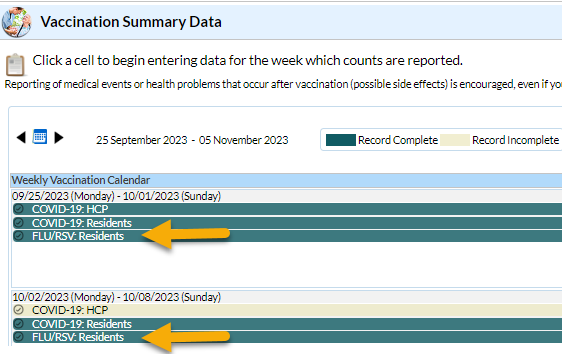
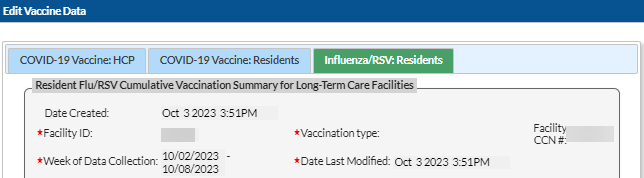
Clicking on the FLU/RSV: Residents tab will populate the weekly Resident Flu/RSV Cumulative Vaccination Summary for Long-Term Care Facilities form. Please note that the FLU/RSV: Residents tab that populates the Resident Flu/RSV Cumulative Vaccination Summary for Long-Term Care Facilities form is only accessible if the Resident COVID-19 Cumulative Vaccination Summary for Long-Term Care Facilities form has already been saved and submitted in NHSN.
If a long-term care facility chooses to report Influenza and RSV vaccination data in NHSN, the following questions must be answered:
Question #1 (number of residents staying in this facility for at least 1 day during the week of data collection). Question #1 will autofill from the total saved and submitted from Question #1 of the Resident COVID-19 Cumulative Vaccination Summary for Long-Term Care Facilities form.
Users may report data for the Influenza section only (questions 2-2.3), the RSV section only (questions 3-3.3), or report for both sections. Questions 2-2.3 or 3-3.3 (Influenza and RSV Vaccination sections) must be manually entered. If at least one value is entered in either Question #2- 2.3 or 3-3.3, then the other remaining data fields in the Influenza and RSV Vaccination sections must also have values entered. Therefore, facilities should enter a “0” in a data field if no residents in the facility pertain to a specific category.
To successfully save and submit Influenza and RSV vaccination data, the sum of the values reported in Questions #2-2.3 or 3-3.3 must equal the total reported in Question #1.
Residents who have received an Influenza vaccine for the current season from September 2023 – May 2024 should be counted as up to date with Influenza vaccination.
Residents who have received a RSV vaccine since it became available in August of 2023 should be counted as up to date with RSV vaccination.
Users can refer to the Influenza and RSV Table of Instructions (TOI) [PDF – 386 KB] for full details on how to categorize residents based on the Influenza or RSV vaccination status. The TOI will review which residents should be counted in questions: medical contraindications, offered but declined, and other/unknown vaccination status. The TOI is a useful resource that includes information on all the data fields included on the influenza/RSV collection form.
If a resident was administered an Influenza or RSV vaccine in the long-term care facility they are residing in, documentation from the facility is sufficient, and the resident can be counted as up to date with Influenza or RSV vaccination.
If a resident has received an Influenza or RSV vaccine outside of the long-term care facility they are residing in, a resident should report in writing (paper or electronic) or provide documentation that the vaccine(s) were received elsewhere to be counted as up to date with Influenza and RSV vaccination.
If a resident is unable to provide written documentation that they have received either vaccine outside of the long-term care facility they are residing in, the resident should be counted in the Other/Unknown Vaccination status category, as verbal statements are not acceptable forms of documentation.
If your long-term care facility has reported and submitted Influenza and RSV vaccination data for residents using the Resident Flu/RSV Cumulative Vaccination Summary for Long-Term Care Facilities form, the FLU/RSV: Residents tab of the Weekly Vaccination Calendar view in NHSN will appear green to indicate that the record has been completed and submitted.
The influenza virus and respiratory syncytial virus (RSV) are common viruses that cause mild, cold-like symptoms. However, individuals living in nursing homes or long-term care facilities are at highest risk of serious illness and health complications from these pathogens. For the first time, vaccines are now available for Influenza, RSV, and COVID-19 pathogens and will help protect against severe illness. For further information, please see the Immunization Overview for Fall and Winter 2023-2024 | CDC
In contrast to incident vaccination data, which are the number of new individuals who received the influenza vaccine in a specific week, cumulative vaccination data are the total number of individuals in the facility who have ever received the influenza vaccine since it became available. For weekly influenza reporting, facilities report cumulative data. An example of this is below:
- Week 1: 10 residents received influenza vaccination.
- Week 2: 5 more residents received influenza vaccination.
Facility should report 15 residents received influenza vaccination at the facility by the end of week 2.
Person-Level Vaccination Reporting: General
No.
The Person-Level COVID-19 Vaccination Forms are optional tools that can be used to report COVID-19 vaccination data. The Person-Level forms replaced the optional excel data tracking worksheets previously offered to facilities to assist with reporting to the Weekly COVID-19 Vaccination Modules.
As of March 28, 2022, long-term care facilities have the option to use these Person-Level COVID-19 Vaccination Forms and select the “view reporting summary and submit” button to submit HCP and resident data to the Weekly Modules.
As of September 11, 2023, facilities that report COVID-19 vaccination data in the Healthcare Personnel Safety (HPS) component will also be able to report data to the main weekly HCP Vaccination module using the Person-Level COVID-19 Vaccination Form. We encourage all LTC and HPS facilities to use these forms to simplify aggregating data for the Weekly COVID-19 Vaccination Modules.
If facilities do not choose to use the Person-level COVID-19 Vaccination Forms, they can continue to submit data through the following ways: Directly into the data entry screens of the COVID-19 Vaccination Modules
- Through .CSV file upload into the Weekly COVID-19 Vaccination Modules
- Note that users with level 1 SAMS access will be unable to use the optional Person-Level COVID-19 Vaccination Forms in the LTC component to summarize and submit data to the Weekly COVID-19 Vaccination modules.
No.
The optional Person-Level COVID-19 Vaccination Form is a tool that can assist Long-term Care Facilities, and Inpatient Facilities/Ambulatory Surgery Centers in managing and reporting COVID-19 vaccination data to the main weekly HCP and Resident vaccination modules.
If facilities chose to use this tool, they must select ‘view reporting summary and submit’, select the week of interest and submit data to the COVID-19 Vaccination HCP and Resident Modules at least once per week for Long-term Care Facilities and at least one week per month for Inpatient Facilities/Ambulatory Surgery Centers.
Yes.
Level 3 Access is required to use the optional Person-Level COVID-19 Vaccination Forms.
If you do not see the Person-Level vaccination forms under the COVID-19 tab, you may not have SAMS Level 3 Access.
To request Level 3 access, please contact the SAMS Help Desk between the hours of 8:00 AM and 8:00 PM EST Monday through Friday (except U.S. Federal holidays) at the following:
- Toll Free: 877-681-2901
- E-mail: samshelp@cdc.gov
The Person-Level COVID-19 Vaccination Form for LTC residents and staff can be used to report data to the Weekly COVID-19 Vaccination Modules beginning with the week of March 28, 2022 – April 3, 2022 and forward.
As of September 11, 2023, the Person-Level COVID-19 Vaccination Form for Healthcare Personnel within the Healthcare Personnel Safety (HPS) Component can be used to report data to the Weekly COVID-19 Vaccination Module. Users will have the option to save and submit data for reporting weeks beginning with the week of June 26, 2023 – July 2, 2023 and forward.
When you click the ‘Week of data collection first day” drop down menu, you will see each reporting week since the Person-Level Vaccination Forms became available listed. You will also note that there is sometimes text next to the date with information about the data for that week. A description of what each label means is below.
Not eligible for submission using the Person-Level Vaccination Form: Weeks already reported to the Weekly COVID-19 Vaccination Summary Modules using the weekly summary form or weekly summary CSV upload are not eligible for submission using the Person-Level Vaccination Form. Instead, please update those weeks by navigating to the Weekly COVID-19 Summary Module directly and updating the weekly summary form.
Never submitted: Data for that reporting week has not been submitted.
Changed since submitted using the Person-Level Form: The summary counts for one or more questions for that reporting week have changed since that week was lasted submitted using the Person-Level Form. Please use the “re-submit all changed weeks” button (next to the week of data collection drop down menu) to re-submit all weeks at the same time where the counts have changed.
If you only see a date, and there is no corresponding text: This indicates that you already submitted data that week via the Person-Level form, and there have been no updates to the data for that week since submission. No action is needed!
No.
The totals are calculated for you on the summary form, but you still need to review the data, click the “View and Reporting Summary & Submit” button (outlined in a red box below), select the week you want to submit data for, and click “Save and Submit Data”. Note that when submitting data in the HPS component you will need to select the vaccination location & week for submission.
You should then confirm the data saved to the weekly form by checking the calendar view and seeing that the week appears green.



You should review data and submit for all weeks affected by updated or newly entered data at least once per week.
Even if you don’t make any changes to the data, Long-term Care Facilities still need to submit once per week and Inpatient Facilities/Ambulatory Surgery Centers need to submit once week per month. If you do not submit data for a given week, it will not be shared to the Weekly COVID-19 Vaccination Module.
If during a reporting week, there are no new changes, you should still be sure you review the data and submit at least once per week.
Vaccination data are not shared with CMS at the person-level.
However, if a facility reports data as part of a CMS Quality Reporting Program, and the facility uses the Person-Level COVID-19 Vaccination Forms to submit their data to the weekly COVID-19 vaccination module (by selecting “view reporting summary and submit”), then this aggregate (summary) weekly COVID-19 vaccination module data is reported to CMS. This will fulfill the CMS reporting requirement.
On the Person-Level COVID-19 Vaccination Form, you should enter the information on the individual’s single dose and on the medical contraindication.
On the reporting summary, you will see that an individual who has a medical contraindication after a dose of a COVID-19 vaccine will be categorized as medical contraindication.
This is consistent with our general guidance for the weekly summary form that if an individual has a severe allergic reaction to the vaccine after a dose of a COVID-19 vaccine, you should classify them as a medical contraindication in accordance with the CDC definition of a contraindication to COVID-19 vaccination.
Starting with Quarter 4 2023, if an individual has a medical contraindication after a receiving a single dose of the 2023-2024 Updated COVID-19 vaccine, this individual will be classified as up-to-date with COVID-19 vaccination and not as a medical contraindication. This is because the individual received the latest COVID-19 vaccine needed to be up-to-date with COVID-19 vaccination, despite having a medical contraindication afterwards.
Yes. Click any column to sort in ascending order. Click the same column again to sort in descending order.
Yes.
Click on the “Hide all HCP with an end date” button of the Person-Level COVID-19 Vaccination Form for Healthcare Personnel to hide all healthcare personnel that have a date entered in the HCP End of Employment Date column:

Click on the “Hide all discharged residents” button of the Person-Level COVID-19 Vaccination Form for Residents to hide all residents that have a date entered in the Resident Discharge Date column:

Note: You can click on the same button above to unhide the rows. On the Person-Level COVID-19 Vaccination Form for Healthcare Personnel, the “Unhide all HCP with an end date” button will appear. On the Person-Level COVID-19 Vaccination Form for Residents, the “Unhide all discharged patients” will appear.
These individuals are counted as declined to receive vaccination. The Person-Level COVID-19 Vaccination Form includes a field where you may provide a reason for declination, including religious exemption.

You can find more information on the Person-Level COVID-19 Vaccination Forms and how to use them in the Table of Instructions. These can be found at:
LTCF Person-Level Vaccination Form Table of Instructions: Healthcare Personnel
LTCF Person-Level Vaccination Form Table of Instructions: Residents
HPS Person-Level Vaccination Form Table of Instructions
Free standing IPF’s and IPR’s should select hospital when choosing the vaccine location type for their HCP because they have their own Facility ID and CCN.
IPF’s and IPR units who share a facility ID, and have their own unique CCN mapped as a location within the parent facility will be able to select the IPF or IPR unit in the vaccine location column.
Check eligible location types by comparing the locations shown in the Weekly Vaccination Summary calendar view of NHSN.
For more information see guidance for free standing facilities [PDF – 233 KB].
Person-Level Reporting: Data entry
To add a new Health Care Worker or Resident to the Person-Level COVID-19 Vaccination Form, please follow the following steps:
- Step 1: Click + Add Row button
- Step 2: New yellow section at the top of the form will appear to enter this individual’s data
- Step 3: Enter required and applicable fields
- Step 4: Click Save Row
You should report vaccine data on all HCP who are eligible to work in the facility at least once per week; these are the people who “regularly” work in the facility on a weekly basis.
Please see the instructions for question 1 in the:
When reporting COVID-19 vaccination data for health care personnel in the HPS component, you can designate which unit(s) the employee works in the Vaccine Location Type column. The choices are Hospital, IPF unit(s), and IRF unit(s). You will only see and be able to select the location types that are already associated with your Facility ID. For more information about vaccine location see FAQ Locations and Enrollment.
When you click “view reporting summary and submit,” each unit has a reporting week listed that can be selected to save and submit data for the specific unit. If your facility is enrolled in one location type, only that location type will display.

Data that are reported for individual units will be counted towards the summary/aggregate data for the unit. For example, if an employee works in both the hospital and the IPF unit, their data would be reflected in both the hospital and IPF weekly summary forms.
Add the new COVID-19 vaccine data to the existing row but do not delete the initial declined date of 3/1/2022.
This allows us to capture the data accurately over time.
No.
The Person-Level COVID-19 Vaccination Form captures changes in individuals’ vaccination status over time.
If an individual’s vaccination status changes, add the new status date to the existing row, and do not delete the old status.
For example, a resident who was recently admitted was offered the COVID-19 vaccine and initially declined on 3/1/2022.
The resident later decided to get vaccinated on 3/6/2022.
Add the new COVID-19 vaccine data to the existing row but do not delete the initial declined date of 3/1/2022.
This allows us to capture the data accurately over time.
Previously saved records can be updated directly in the NHSN person-level forms by clicking the cell that needs to be updated and enter the changes directly into the grid of the record.
Note: Be sure to click out of the cell(s) modified and then click “view reporting summary and submit” to share the new information for all weeks impacted by a change to the Weekly COVID-19 Vaccination Modules.
If you do not click “view reporting summary and submit” and save and submit for all modified weeks, this modified information will not be reflected in the Weekly COVID-19 Vaccination Modules.
If a HCW goes on leave and returns to work in 2 weeks (14 days) or less, nothing on their row needs to be changed, and their information can continue to be maintained on the original row.
If the HCW goes on leave for longer than 2 weeks (14 days) and returns to work after more than 2 weeks, you should enter an end date on the day they begin leave.
When they return to work, you should duplicate their row (using the + button next to their row) and enter a new start date on their new row.
The new start date on the new row is the day they return to work.
Note: This is consistent with our guidance for the weekly summary forms that says to continue including HCP on temporary leave (2 weeks or less) and to exclude HCP if their leave is longer than 2 weeks.
| Healthcare Personnel | Residents | |
| Include on same row if: |
|
|
| Add end date and create new row (using + button to duplicate row) if:
|
|
|
If the resident is discharged or leaves the facility for any reason, and then returns or is re-admitted within 1 week (7 days) or less, nothing on their row needs to be changed, and their information can continue to be maintained on the original row.
If the resident is discharged or leaves the facility for any reason for longer than 1 week (7 days) and returns or is re-admitted after more than 1 week, you should enter a discharge date on the day they were discharged or left.
When they return or are re-admitted, you should duplicate their row (using the + button next to their row) and enter a new admission date on their new row.
Note: This is consistent with our guidance for the weekly summary forms that says to count all residents occupying a bed at this facility for at least 1 day (at least 24 hours) during the week of data collection.
| Healthcare Personnel | Residents | |
| Include on same row if: |
|
|
| Add end date and create new row (using + button to duplicate row) if:
|
|
|
No. If data is entered and saved, the row cannot be deleted. It is recommended that you do one of the following:
Edit the row/ repurpose the row with someone else’s data or
Change the discharge/end date to a date that is before the event-level forms can be used to submit date (i.e., before 3/28/2022). This way, the incorrect individual won’t contribute to any data that can be submitted.
Note: If you do this, you should also change the name and ID to avoid confusion. Also, add a note to the “Comments” column on the far right to document that this entry is incorrect.

Yes. Please use the same identifier for individuals throughout the NHSN application, and ensure that each individual has a UNIQUE identifier. If you enter an individual who has a matching identifier to one in the POC form, the name, gender, date of birth, ethnicity, and race will automatically be filled in. Please note that although the row has auto filled the individuals’ demographics, the vaccination information will need to be entered prior to saving the row for that individual.
First, you will click ‘Upload CSV’.
Second, you will click ‘Browse’ to locate the saved file.
Third, once the selected file is visible in the Browse box, you will then click the ‘Upload CSV’ button.

- Information about the LTCF COVID-19 Person-Level Vaccination Forms can be found on the Weekly HCP & Resident COVID-19 Vaccination | LTCF | NHSN | CDC
- NHSN LTCF Person-Level Vaccination Forms: General Training – December 2022: Slideset [PDF – 3 MB]; YouTube Link
- LTCF Person-Level COVID-19 Vaccination Forms – Instructions and Guidance Documents [PDF – 233 KB]
- LTCF Person-Level COVID-19 Vaccination Forms: A How-To Guide
- LTCF 1 Pager: NHSN COVID-19 (Person-Level) Forms
- LTCF Person-Level Vaccination Form Table of Instructions: Healthcare Personnel
- LTCF Person-Level Vaccination Form Table of Instructions: Residents
- LTCF Person-Level COVID-19 Vaccination Data – CSV Data Import
- Variable description and file layout for person-level vaccination forms
- .CSV File Template for LTCF Residents
- Example .CSV File for LTCF Residents
- .CSV File Template for LTCF HCP
- Example .CSV File for LTCF HCP
- Information about the HPS COVID-19 Person-Level Vaccination Forms can be found on the HPS | Weekly HCP COVID-19 Vaccination | NHSN | CDC
- NHSN HPS Person-Level Vaccination Forms: General Training – September 2023:
- HPS Person-Level COVID-19 Vaccination Forms – Instructions and Guidance Documents
- HPS Person-Level COVID-19 Vaccination Forms: A How-To Guide
- HPS 1 Pager: NHSN COVID-19 (Person-Level) Forms
- HPS Person-Level Vaccination Form Table of Instruction
- HPS Person-Level COVID-19 Vaccination Data – CSV Data Import
- Variable description and file layout for person-level vaccination forms
- .CSV File Template for HPS HCP
- Example .CSV File for HPS HCP
Individuals are counted as unknown vaccination status in the following circumstances:
- The individual is listed as unknown vaccination status.
- The individual has a single dose of an unknown/unspecified manufacturer. This individual is categorized as unknown vaccination status because it is unclear if this single unspecified dose represents the most current recommendations for COVID-19 vaccines .
- The individual has a gap between their start date and the first status date that is entered, such as start date 1/1, declined on 2/3. The individual will be categorized as unknown vaccination status from 1/1 to 2/2.
- The individual has a single primary series monovalent dose, and the reporting week is June 26, 2023 or later.
- The resident is not up-to-date with COVID-19 vaccination, does not have a documented medical contraindication or declination of COVID-19 vaccine, and the reporting week is June 26, 2023 or later.
- The healthcare worker is not up-to-date with COVID-19 vaccination, does not have a documented medical contraindication or declination of COVID-19 vaccine, and the reporting week is January 1, 2024 or later.