Shingles Vaccination Among Adults Aged 60 and Over: United States, 2018
- Key findings
- From 2008 through 2018, the percentage of adults aged 60 and over who had ever received a shingles vaccine increased for all age groups examined.
- Among adults aged 60 and over, receipt of shingles vaccination varied by race and Hispanic origin, but not sex.
- Receipt of shingles vaccination varied by poverty status and educational attainment among adults aged 60 and over.
- Among adults aged 60 and over, the percentage who had ever received a shingles vaccine ranged from 26.3% in the East South Central region to 42.8% in the West North Central region.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 370, July 2020
PDF Version (589 KB)
Key findings
Data from the National Health Interview Survey
- Shingles vaccination among adults aged 60 and over increased from 6.7% in 2008 to 34.5% in 2018.
- In 2018, women (35.4%) were equally as likely as men (33.5%) to have ever received a shingles vaccine.
- Non-Hispanic white adults (38.6%) were approximately twice as likely as non-Hispanic black (18.8%) and Hispanic (19.5%) adults to have ever received a shingles vaccine.
- Vaccination coverage was highest for those who were not poor and those who had more than a high school education.
- The percentage of adults aged 60 and over who ever had a shingles vaccination ranged from 26.3% in the East South Central region to 42.8% in the West North Central region of the United States.
Shingles is a painful rash caused by the varicella zoster virus (1). Persons of all ages are at risk for shingles. However, this risk and the risk of complications increase with age (1,2). Vaccines have been developed to prevent shingles, and beginning in 2017, the Advisory Committee on Immunization Practices (ACIP) recommended that all adults aged 50 and over be vaccinated (3). Prior to this change, ACIP had recommended that only adults aged 60 and over receive a shingles vaccine (3). This report describes trends in shingles vaccination as well as variation by demographic, socioeconomic, and geographic characteristics among adults aged 60 and over.
Keywords: herpes zoster, vaccine, prevention, National Health Interview Survey
From 2008 through 2018, the percentage of adults aged 60 and over who had ever received a shingles vaccine increased for all age groups examined.
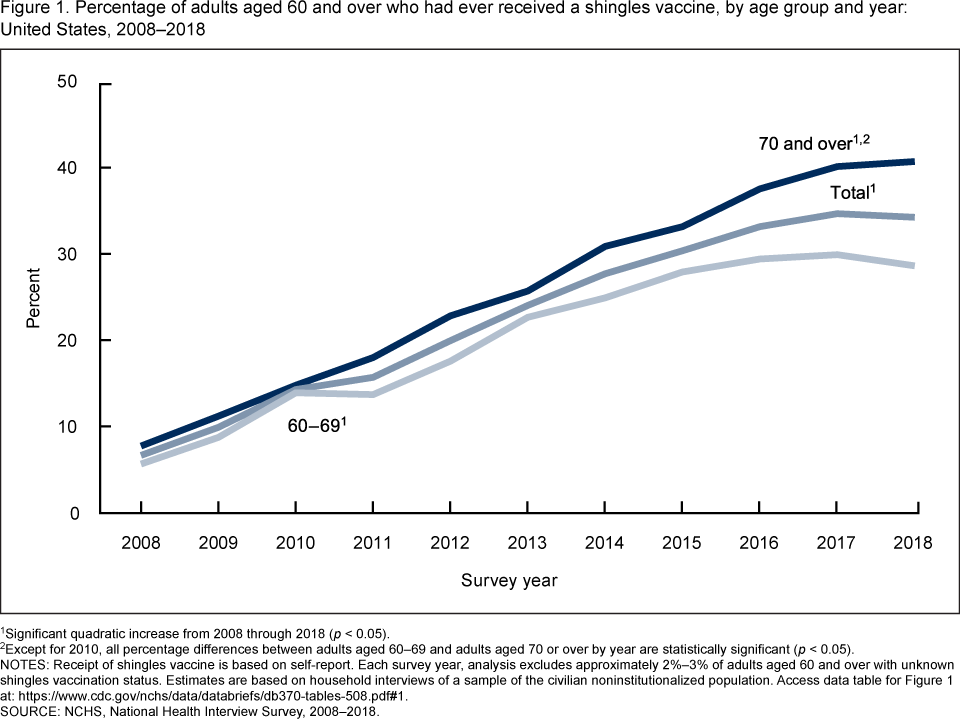
- Among adults aged 60 and over, the percentage who had ever received a shingles vaccine increased from 6.7% in 2008 to 33.4% in 2016, and then remained constant through 2018 (34.5%) (Figure 1).
- Among adults aged 60–69, the percentage who had ever received a shingles vaccine increased from 5.7% in 2008 to 29.6% in 2016, and then remained constant through 2018 (28.8%).
- Among adults aged 70 and over, the percentage who had ever received a shingles vaccine increased from 7.8% in 2008 to 37.8% in 2016, and then remained constant through 2018 (41.0%).
- For each year during 2008–2018, except for 2010, adults aged 70 and over were more likely than those aged 60–69 to have ever received a shingles vaccine.
Figure 1. Percentage of adults aged 60 and over who had ever received a shingles vaccine, by age group and year: United States, 2008–2018
1Significant quadratic increase from 2008–2018 (p < 0.05).
2Except for 2010, all percentage differences between adults aged 60–69 years and adults aged 70 or over by year are statistically significant (p < 0.05).
NOTES: Receipt of shingles vaccine is based on self-report. Each survey year, analysis excludes approximately 2%–3% of adults aged 60 and over with unknown shingles vaccination status. Estimates are based on household interviews of a sample of the civilian noninstitutionalized population. Access data table for Figure 1.
SOURCE: NCHS, National Health Interview Survey, 2008–2018.
Among adults aged 60 and over, receipt of shingles vaccination varied by race and Hispanic origin, but not sex.
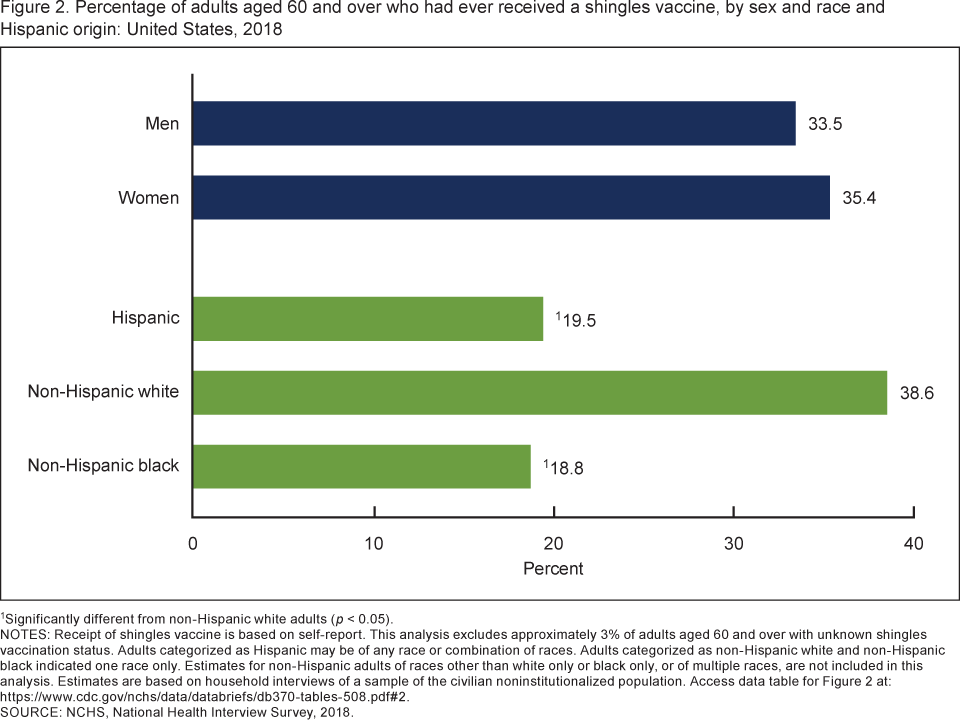
- Among adults aged 60 and over, women (35.4%) were equally as likely as men (33.5%) to have ever received a shingles vaccine (Figure 2).
- Non-Hispanic white adults (38.6%) were more likely to have ever received a shingles vaccine than both Hispanic (19.5%) and non-Hispanic black (18.8%) adults.
Figure 2. Percentage of adults aged 60 and over who had ever received a shingles vaccine, by sex and race and Hispanic origin: United States, 2018
1Significantly different from non-Hispanic white adults (p < 0.05).
NOTES: Receipt of shingles vaccine is based on self-report. This analysis excludes approximately 3% of adults aged 60 and over with unknown shingles vaccination status. Adults categorized as Hispanic may be of any race or combination of races. Adults categorized as non-Hispanic white and non-Hispanic black indicated one race only. Estimates for non-Hispanic adults of races other than white only or black only, or of multiple races, are not included in this analysis. Estimates are based on household interviews of a sample of the civilian noninstitutionalized population. Access data table for Figure 2.
SOURCE: NCHS, National Health Interview Survey, 2018.
Receipt of shingles vaccination varied by poverty status and educational attainment among adults aged 60 and over.
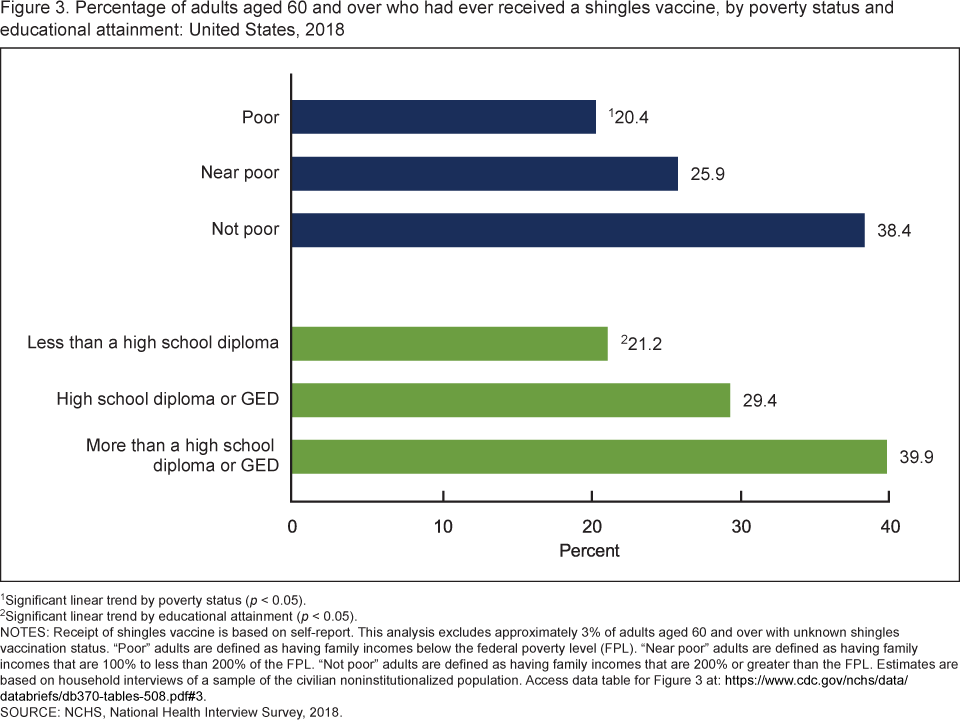
- Receipt of shingles vaccination increased with family income, from 20.4% among poor adults to 38.4% among not-poor adults (Figure 3).
- Receipt of shingles vaccination increased with educational attainment, from 21.2% among adults with less than a high school diploma to 39.9% among adults with more than a high school diploma or GED.
Figure 3. Percentage of adults aged 60 and over who had ever received a shingles vaccine, by poverty status and educational attainment: United States, 2018
1Significant linear trend by poverty status (p < 0.05).
2Significant linear trend by educational attainment (p < 0.05).
NOTES: Receipt of shingles vaccine is based on self-report. This analysis excludes approximately 3% of adults aged 60 and over with unknown shingles vaccination status. “Poor” adults are defined as having family incomes below the federal poverty level (FPL). “Near poor” adults are defined as having family incomes that are 100% to less than 200% of the FPL. “Not poor” adults are defined as having family incomes that are 200% or greater than the FPL. Estimates are based on household interviews of a sample of the civilian noninstitutionalized population. Access data table for Figure 3.
SOURCE: NCHS, National Health Interview Survey, 2018.
Among adults aged 60 and over, the percentage who had ever received a shingles vaccine ranged from 26.3% in the East South Central region to 42.8% in the West North Central region.
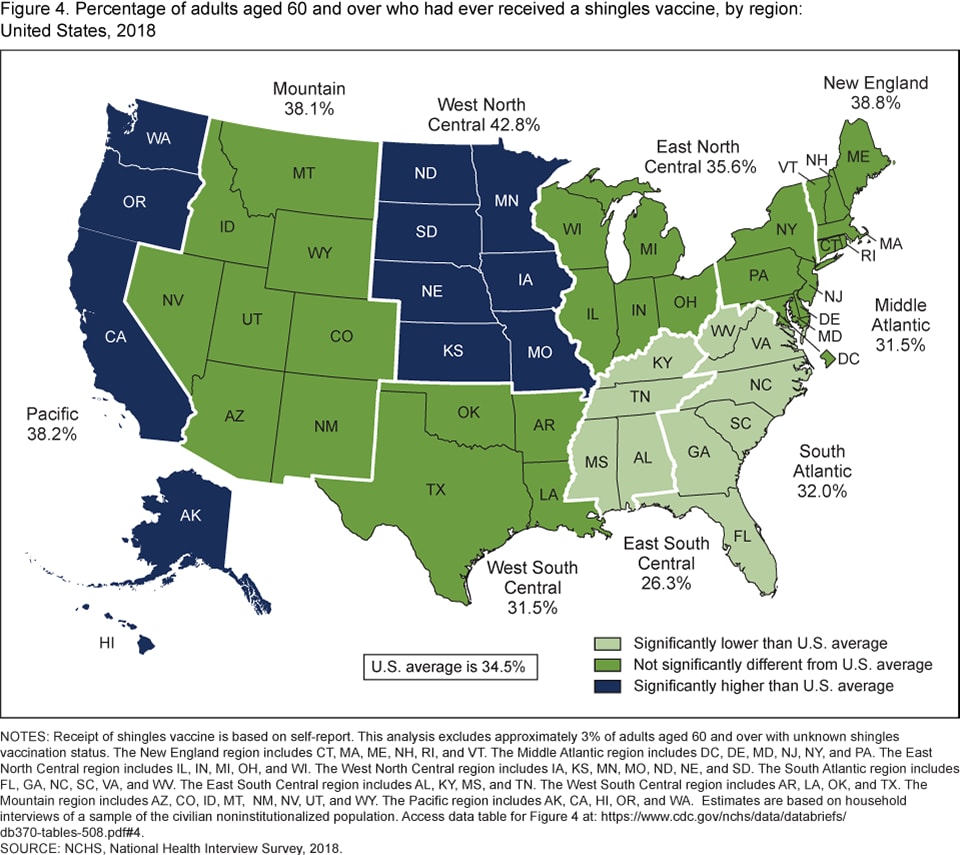
- The percentage of adults aged 60 and over who had ever received a shingles vaccine was significantly lower in the South Atlantic (32.0%) and East South Central (26.3%) regions compared with the national average (34.5%) (Figure 4).
- The percentage of adults aged 60 and over who had ever received a shingles vaccine was significantly higher in the West North Central (42.8%) and Pacific (38.2%) regions compared with the national average.
- The percentage of adults aged 60 and over who had ever received a shingles vaccine in the Mountain (38.1%), West South Central (31.5%), East North Central (35.6%), Middle Atlantic (31.5%), and New England (38.8%) regions was not significantly different from the national average.
Figure 4. Percentage of adults aged 60 and over who had ever received a shingles vaccine, by region: United States, 2018
NOTES: Receipt of shingles vaccine is based on self-report. This analysis excludes approximately 3% of adults aged 60 and over with unknown shingles vaccination status. The New England region includes CT, MA, ME, NH, RI, and VT. The Middle Atlantic region includes DC, DE, MD, NJ, NY, and PA. The East North Central region includes IL, IN, MI, OH, and WI. The West North Central region includes IA, KS, MN, MO, ND, NE, and SD. The South Atlantic region includes FL, GA, NC, SC, VA, and WV. The East South Central region includes AL, KY, MS, and TN. The West South Central region includes AR, LA, OK, and TX. The Mountain region includes AZ, CO, ID, MT, NM, NV, UT, and WY. The Pacific region includes AK, CA, HI, OR, and WA. Estimates are based on household interviews of a sample of the civilian noninstitutionalized population. Access data table for Figure 4.
SOURCE: NCHS, National Health Interview Survey, 2018.
Summary
Shingles vaccination among adults aged 60 and over increased from 6.7% in 2008 to 34.5% in 2018. Vaccination increased among both adults aged 60–69 and adults aged 70 and over. While there has been a shingles vaccine available since 2006, a new vaccine was introduced in late 2017, and uptake in the market may have occurred differentially in 2018. The discontinuation of Zostavax®, the shingles vaccine singly available prior to 2018, starting in 2020 may further alter shingles vaccination patterns (4). Also in 2017, ACIP expanded their recommendation for shingles vaccination to adults aged 50 and over (3). Prior to this change (starting in 2008), shingles vaccination was only recommended for those aged 60 and over.
Shingles vaccination did not differ by sex, but non-Hispanic white adults were more likely to have ever received this vaccine compared with Hispanic and non-Hispanic black adults. Shingles vaccination increased with educational attainment, as well as with increasing family income. Additionally, regional differences were observed in receipt of shingles vaccination. This report’s findings are consistent with previous research regarding disparities in shingles vaccination by demographic and geographic characteristics (5,6). However, this report uses more recent data from a large, nationally representative data source to update these estimates and describe these disparities.
Definitions
Poverty status: Categories were calculated using National Health Interview Survey (NHIS) imputed income files and were based on family income and family size, using the U.S. Census Bureau’s poverty thresholds. “Poor” persons are defined as those with incomes below the federal poverty level (FPL); “near poor” persons have incomes of 100% to less than 200% of the FPL; and “not poor” persons have incomes of 200% of the FPL or greater.
Race and Hispanic origin: Adults categorized as Hispanic may be of any race or combination of races. Adults categorized as non-Hispanic white and non-Hispanic black indicated one race only. Estimates for non-Hispanic adults of races other than white only or black only, or of multiple races, are not included in this analysis.
Regions: Categories were slightly modified from the nine U.S. Census Bureau-designated divisions by moving Delaware, the District of Columbia, and Maryland into the Middle Atlantic region (7). Divisions include: New England—Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, Vermont; Middle Atlantic—Delaware, District of Columbia, Maryland, New Jersey, New York, Pennsylvania; East North Central—Illinois, Indiana, Michigan, Ohio, Wisconsin; West North Central—Iowa, Kansas, Minnesota, Missouri, Nebraska, North Dakota, South Dakota; South Atlantic—Florida, Georgia, North Carolina, South Carolina, Virginia, West Virginia; East South Central—Alabama, Kentucky, Mississippi, Tennessee; West South Central— Arkansas, Louisiana, Oklahoma, Texas; Mountain—Arizona, Colorado, Idaho, Montana, Nevada, New Mexico, Utah, Wyoming; and Pacific—Alaska, California, Hawaii, Oregon, Washington.
Shingles vaccination: From 2008 through 2017, this information was collected based on the survey question, “Shingles is an outbreak of a rash or blisters on the skin that may be associated with severe pain. The pain is generally on one side of the body or face. Shingles is caused by the chicken pox virus. A vaccine for shingles has been available since May 2006. Have you ever had the Zoster or Shingles vaccine, also called Zostavax®?” In 2018, the wording of this question was changed to, “Shingles is an illness that results in a rash or blisters on the skin and is usually painful. There are two vaccines now available for shingles; Zostavax®, which requires 1 shot, and Shingrix®, a new vaccine which requires 2 shots. Have you had a vaccine for shingles?” Receipt of a shingles vaccination was based on a positive response to these questions.
Data source and methods
Data from the 2008–2018 NHIS were used for this analysis. NHIS is a nationally representative household survey of the civilian noninstitutionalized U.S. population. It is conducted continuously throughout the year by the National Center for Health Statistics (NCHS). Interviews are conducted in respondents’ homes, but follow-ups to complete interviews may be conducted over the telephone. For more information about NHIS, visit: https://www.cdc.gov/nchs/nhis.htm.
Point estimates and the corresponding confidence intervals for this analysis were calculated using SUDAAN software (8) to account for the complex sample design of NHIS. Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. Trends by age group were evaluated using JoinPoint software and confirmed using orthogonal polynomials in logistic regression. Trends by poverty status and educational attainment were evaluated using orthogonal polynomials in logistic regression. All estimates in this report meet NCHS data presentation standards for proportions (9).
About the authors
Emily P. Terlizzi and Lindsey I. Black are with the National Center for Health Statistics, Division of Health Interview Statistics.
References
- National Center for Immunization and Respiratory Diseases. Shingles (herpes zoster).
- National Center for Immunization and Respiratory Diseases. Complications of shingles.
- Dooling KL, Guo A, Patel M, Lee GM, Moore K, Belongia EA, Harpaz R. Recommendations of the Advisory Committee on Immunization Practices for use of herpes zoster vaccines. MMWR Morb Mortal Wkly Rep 67(3):103–8. 2018.
- National Center for Immunization and Respiratory Diseases. Shingles (herpes zoster).
- National Center for Immunization and Respiratory Diseases. Vaccination coverage among adults in the United States, National Health Interview Survey, 2016.
- Lu P, O’Halloran A, Williams WW, Harpaz R. National and state-specific shingles vaccination among adults aged ≥ 60 years. AM J Prev Med 52(3): 362–72. 2017.
- Holahan J, Buettgens M, Carroll C, Dorn S. The cost and coverage implications of the ACA Medicaid expansion: National and state-by-state analysis. Kaiser Commission on Medicaid and the Uninsured. 2012.
- RTI International. SUDAAN (Release 11.0.3) [computer software]. 2018.
- Parker JD, Talih M, Malec DJ, Beresovsky V, Carroll M, Gonzalez Jr. JF, et al. National Center for Health Statistics data presentation standards for proportions. National Center for Health Statistics. Vital Health Stat 2(175). 2017.
Suggested citation
Terlizzi EP, Black LI. Shingles vaccination among adults aged 60 and over: United States, 2018. NCHS Data Brief, no 370. Hyattsville, MD: National Center for Health Statistics. 2020.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Brian C. Moyer, Ph.D., Director
Amy M. Branum, Ph.D., Acting Associate Director for Science
Division of Health Interview Statistics
Stephen J. Blumberg, Ph.D., Director
Anjel Vahratian, Ph.D., M.P.H., Associate Director for Science