|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
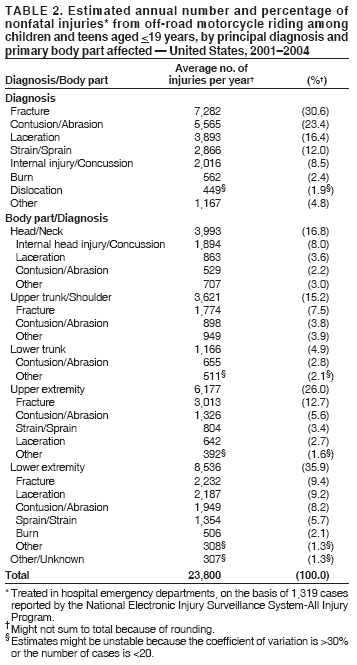
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Nonfatal Injuries from Off-Road Motorcycle Riding Among Children and Teens --- United States, 2001--2004Motorcycle crashes are a substantial public health problem for children and teens. During 2003, among persons aged <19 years, at least 245 died and an estimated 56,870 were treated in U.S. hospital emergency departments (EDs) for injuries sustained while riding a motorcycle (1). National surveillance has focused primarily on monitoring and characterizing fatal and nonfatal injuries from motorcycle crashes occurring on public roads (2). However, during 2003, at least 13 motorcycle riders aged <19 years died in nontraffic incidents in places other than on public roads.* This report focuses on injuries associated with off-road motorcycle riding, an increasingly popular recreational activity among youths. To characterize nonfatal injuries among young off-road motorcycle riders in the United States, CDC analyzed data from the National Electronic Injury Surveillance System-All Injury Program (NEISS-AIP) during 2001--2004. Those data indicated that an estimated 23,800 off-road motorcyclists aged <19 years were treated for nonfatal injuries in U.S. hospital EDs each year. Programs and policies directed at reducing the number of injuries from off-road motorcycle riding need to be strengthened; requiring minimum ages for off-road motorcycle riding might help prevent such injuries among children and teens. Operated by the Consumer Product Safety Commission (CPSC), NEISS-AIP collects data regarding initial patient visits to U.S. EDs for all types and causes of injuries, approximately 500,000 each year (2). NEISS-AIP data are drawn from a nationally representative subsample of 66 of 100 NEISS-AIP hospitals selected as a stratified probability sample of the estimated 5,400 hospitals with EDs in the United States and its territories. Data are weighted to represent the total number of initial injury-related visits each year in the United States, and estimates are adjusted for hospital nonresponse and changes in the number of ED visits from year to year. For this study, NEISS-AIP cases of nonfatal injuries from off-road motorcycle riding were identified from narratives describing injury incidents that were abstracted from medical records and consumer product codes assigned by trained NEISS hospital coders. A motorcycle was defined as any road bike, dirt bike (or trail bike), moped, motor scooter, or minibike. Excluded were incidents involving three-wheeled and four-wheeled all-terrain vehicles (ATVs). Cases were defined as injuries among patients aged <19 years who were injured while riding off-road as the driver or passenger on a motorcycle; patients not riding on a motorcycle when injured (e.g., those injured while working on a motorcycle) were excluded. Cases were defined as off-road if the incident did not occur on a paved road or highway and the location of the incident was specified (e.g., woods, field, trail, backyard of home, or motocross arena). In addition, 20.4% of motorcycle injury incidents had no location specified and, therefore, were excluded from the study. Location was further classified as a motocross area if this was specified in the narrative or if the activity involved racing or jumping with motorcycles in an unspecified off-road location. National estimates were based on weighted data for 1,319 cases in which patients aged <19 years were treated for off-road motorcyclist injuries at NEISS-AIP hospital EDs during 2001--2004. Each case was assigned a sample weight based on the inverse probability of selection; these weights were summed to provide national estimates. Rates were calculated using U.S. Census bridged-race population estimates for 2001--2004 (3). A direct variance estimation procedure was used to calculate 95% confidence intervals and to account for the complex sample design. During 2001--2004, an estimated 23,800 (32.6 per 100,000 population) children and teens aged <19 years were treated at U.S. EDs for off-road motorcycle injuries each year (Table 1). The injury rate increased 33.7%, from 26.4 per 100,000 population in 2001 to 35.3 in 2004; however, this difference was not statistically significant (p = 0.31). Patients aged 12--15 years had the highest nonfatal injury rate (62.1 per 100,000). Patients aged <16 years accounted for 69.9% of those injured; 88.4% of those injured were males, and 97.1% were driving the motorcycle. Overall, 7.5% of those injured were hospitalized. By location, 20.0% of the injuries occurred in motocross areas, and 70.2% of those injured were reported as riding dirt bikes/trail bikes when they incurred their injuries. Those injured in motocross areas were more likely to be hospitalized than those injured in other off-road locations (14.9% versus 5.6%; p = 0.01). According to the narratives abstracted from ED charts, 8.9% of the injuries were sustained during a motorcycle jump, and 5.3% resulted from hitting another motorcycle or other off-road vehicle. Among jump-related injuries, 74.3% occurred in a motocross area. Serious injuries (i.e., fractures or internal injuries) accounted for 39.1% of the principal diagnoses (Table 2). The primary injury was to an extremity in 61.9% of patients, and 35.6% of extremity injuries were fractures. The head or neck was the primary body part affected in 16.8% of cases, of which 47.4% involved an internal head injury. Reported by: JM Conn, MS, JL Annest, PhD, Office of Statistics and Programming; LJ Paulozzi, MD, Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control, CDC. Editorial Note:This report characterizes nonfatal injuries from off-road riding of all types of motorcycles during 2001--2004. Motorcycles that are designed specifically for off-road riding (commonly referred to as dirt bikes or trail bikes) are increasing in popularity in the United States. Approximately 300,000 off-road motorcycles were sold in the United States during 2003, nearly twice the sales figure for 1999. The activity is most popular among persons who are male, aged <30 years, white, residents of nonmetropolitan areas, and have less than a college education (4). During 1994--1996, approximately 10,000 persons aged <15 years sought care in EDs each year for injuries related to off-road motorcycles (5). The results described in this report indicate that the number of such injuries among persons in this age group might have grown, with approximately 16,600 children aged <16 years treated each year in U.S. EDs during 2001--2004. The increase by one third in the nonfatal injury rate from 2001 to 2004 observed in this study, although not significant, parallels the trend from 2001 to 2003 in injuries involving ATVs among children aged <16 years (6). Although young off-road motorcyclists generally travel at lower speeds than motorcyclists on public roads and have little risk of collision with automobiles, they face other hazards, including irregularities in terrain and obstacles (e.g., trees and fences). Motocross races (i.e., organized racing of motorcycles on off-road circuits) present fewer stationary obstructions but involve risk for collision with competing motorcycles and hazards associated with jumps. Patients with injuries from off-road motorcycle riding who were treated in U.S. EDs were more likely to require hospitalization (7.5%) than those injured while bicycling (3.7%) (1). The findings in this report are subject to at least four limitations. First, NEISS-AIP is designed to provide national estimates and does not provide regional, state, or local estimates. Second, the NEISS-AIP data in this report likely underestimate the number of off-road motorcycle riding injuries in children and teens because 1) they do not include persons treated in physician offices or other health-care facilities or persons who received no treatment, and 2) they do not include 20.4% of motorcycle injury incidents for which the location was not specified. Third, nonfatal injury rates were calculated using U.S. population estimates as denominators rather than the number of off-road motorcycle riders. Estimates of the number of these riders in the United States and the extent of their exposure (e.g., frequency and duration of riding) are not available. Finally, factors associated with off-road motorcycle riding injuries cannot be characterized more completely because no NEISS-AIP data were available on variables such as helmet use, motorcycle speed at the time of injury, alcohol use, or riding experience. Off-road motorcycle riding, like operating motor vehicles on roadways, requires physical skills and judgment that children and young teens do not possess. In 2000, the American Academy of Pediatrics recommended that parents not allow children and teens aged <16 years to ride off-road motorcycles or ATVs and that states prohibit the use of such vehicles by children and teens in that age group (5). Studies of ATV use indicate that state laws with age restrictions for off-road vehicle use can be effective in decreasing the proportion of riders under the minimum age and that requiring riders of off-road vehicles to wear helmets can reduce the risk for fatal injury (7,8). However, only 19 states require off-road motorcyclists aged <18 years to wear helmets, and only eight states† set minimum ages (range: 8--14 years) for operation of off-road motorcycles, according to the American Motorcycle Association (9). Health-care providers should counsel parents regarding the risks associated with children and teens riding any type of motorcycle and the benefits of helmet use (10). This intervention and promotion of minimum age restrictions and helmet laws might help curtail the increase in off-road motorcycle injuries among children and teens. Acknowledgments This report is based, in part, on data contributed by T Schroeder, MS, C Irish, and other staff of the Div of Hazard and Injury Data Systems, Consumer Product Safety Commission; and statistical assistance from T Haileyesus, MS, G Ryan, PhD, and K Thomas, MPH, Office of Statistics and Programming, National Center for Injury Prevention and Control, CDC. References
* Data from National Vital Statistics System; available at http://www.cdc.gov/nchs/nvss.htm. † States and their minimum ages for operation of off-road motorcycles are as follows: Connecticut, 12 years; Iowa, 12; Maine, 10; Maryland, 12; Massachusetts, 10; New Jersey, 14; Pennsylvania, 10; and Utah, 8.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 6/7/2006 |
|||||||||
|