Responding to Rohingya Refugee Crisis
April 30, 2019

Water, sanitation, and hygiene issues pose health threats in the camp. Photo: Anu Rajasingham
Fleeing political repression and violence in Burma (Myanmar), more than 900,000 Rohingya refugees have crossed the border into Bangladesh since August 2017.
Arriving on foot to ill-equipped settlements, the Rohingya refugees face numerous health risks including malnutrition, unsafe drinking water, poor sanitation and hygiene, lack of health care, and overcrowding. These conditions leave them especially vulnerable and exposed to epidemic-prone diseases. CDC is collaborating with the government of Bangladesh and international partners to respond to this humanitarian emergency.
Within the refugee settlements, water, sanitation, and hygiene (WASH) issues are of immediate concern, especially because cholera is endemic to the area. While there are major efforts to expand access to safe drinking water and to provide access to adequate latrines for the Rohingya refugees, gaps in access still remain more than 18 months after the initial influx.
In Cox’s Bazar, where most of the refugees are located, WASH experts have determined that centralized chlorinated piped systems with community tapstands are the best long-term water provision strategy for the camps. In the short- to medium-term, humanitarian partners are distributing point-of-use household water treatment products and implementing bucket chlorination at tube wells to reduce the risk of cholera and other waterborne disease outbreaks. At these sites, an attendant puts chlorine directly into water collection vessels to ensure households are using chlorinated water. According to a WASH household survey completed in April 2018, only 13% of the households interviewed reported using household water treatment methods. Because of these results, WASH experts scaled-up bucket chlorination activities to improve chlorination during the 2018 monsoon season.
ROBUST RESPONSE TO A COMPLEX CRISIS
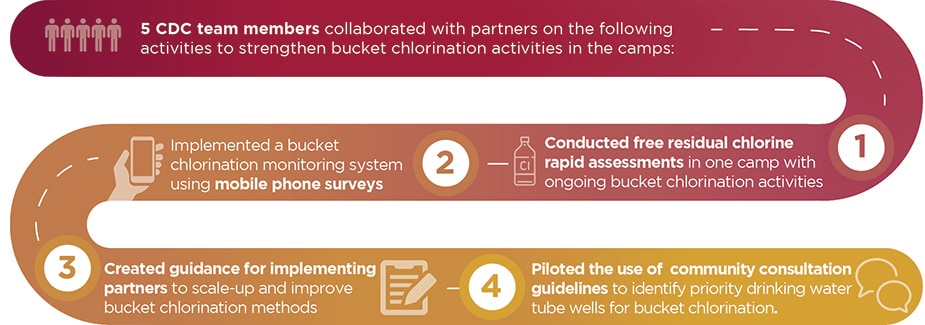
To support this work, five CDC headquarters staff collaborated with partners on the ground, including the CDC Bangladesh team, to strengthen bucket chlorination activities in the camps. They conducted free residual chlorine rapid assessments to provide a snapshot of current chlorination coverage and implemented a bucket chlorination monitoring system using mobile phone surveys to ensure presence of chlorinators, correct dosing of containers, and presence of chlorine in stored water.
The public health threats facing the Rohingya refugees are significant and require a multidimensional and multi-sectoral response. In addition to WASH activities, CDC support has played a critical role in addressing multiple health-related challenges in the community. Michael Friedman, CDC Bangladesh country director said, “In the face of a complex crisis with multiple opportunities for outbreaks, CDC’s robust response provided critical, on-the-ground epidemiological support through our technical experts to the organizations on the forefront of the response.” Working closely with international partners and local government, CDC’s epidemiologists have supported high-quality assessments and planning related to nutrition, immunization, and health information systems. Perhaps most notably, when a suspected diphtheria outbreak swept through the camps, CDC quickly sent laboratory supplies and laboratory experts to establish testing capacity in Bangladesh that confirmed c. diphtheria as the source of the outbreak.
As the Rohingya crisis persists and the refugees continue to face numerous health threats, CDC efforts remain relevant to mitigate the risk of outbreaks and improve quality of life until a solution is found. As Friedman said, “The Rohingya crisis response teaches us that an emergency of such magnitude and complexity requires multi-pronged and multi-level collaborations, locally and regionally. When we address the needs of refugee communities, everyone benefits—including the host country and beyond.”
