|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
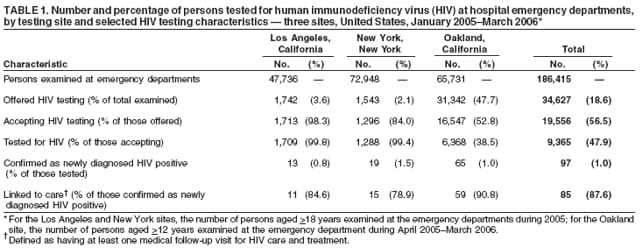
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Rapid HIV Testing in Emergency Departments --- Three U.S. Sites, January 2005--March 2006Approximately one fourth of the estimated 1 million persons living with human immunodeficiency virus (HIV) in the United States are unaware that they are infected with HIV and at risk for transmitting the virus to others (1,2). In April 2003, CDC announced a new initiative, Advancing HIV Prevention: New Strategies for a Changing Epidemic, aimed at reducing barriers to early diagnosis of HIV infection and increasing access of persons infected with HIV to medical care and prevention services (3). A priority strategy of this initiative is to make HIV testing a routine part of medical care. In April 2004, HIV testing was implemented in one emergency department (ED) in Los Angeles, California, and one in New York, New York, to determine the feasibility and acceptability of offering rapid HIV testing as a routine part of health care in EDs. In January 2005, an ED in Oakland, California, also began offering HIV testing routinely. This report summarizes the preliminary results of integrating rapid HIV testing into the health-care services routinely offered in the three EDs during January 2005--March 2006. Those results indicated that, of 9,365 persons tested, 97 (1.0%) ED patients had newly diagnosed HIV infection, and 85 (88%) of those 97 were linked after diagnosis to HIV care and treatment. EDs should consider integrating rapid HIV testing into their routine medical services to identify patients who are unaware that they are infected with HIV and link them to health and prevention services. The three demonstration projects sought to evaluate patient acceptance and the feasibility of making rapid HIV testing a routine part of health care offered in EDs and to ensure that patients with confirmed HIV infection received appropriate follow-up health care. Data from January--December 2005 were analyzed from the New York and Los Angeles EDs; data from April 2005--March 2006 were analyzed from the Oakland ED. These two periods were chosen because they provided at least 12 months of data when all three testing programs were operating at full capacity. Testing protocols at the three sites were similar. All sites placed posters and brochures in waiting rooms and registration areas advertising the availability of free rapid HIV screening. Persons who, when asked, told project staff members that they were HIV negative or did not know their HIV status and who met project consent requirements (i.e., aged >18 years in New York and Los Angeles or aged >12 years in Oakland) were offered testing on an opt-in basis (i.e., patients were offered testing and had tests performed if they agreed to be tested and provided specific written consent). In all three EDs, preliminary testing was conducted using rapid HIV test kits (OraQuick® Advance™ Rapid HIV-1/2 Antibody Tests [OraSure Technologies, Bethlehem, Pennsylvania])* with oral mucosal transudate specimens or finger-stick whole blood specimens. Patients who had positive rapid tests were given risk-reduction counseling and asked to provide a whole blood or oral specimen for confirmatory testing by Western blot. Testing procedures for the three sites differed by the location within the ED where HIV testing was offered and by the personnel responsible for testing and counseling. At the Los Angeles and New York sites, standard pretest information, HIV testing, and test results were provided exclusively by HIV counselors hired specifically to offer and provide these services in the ED. Counselors usually offered HIV testing (in a private room) to the next available patient in the ED waiting area but sometimes provided counseling and testing to patients referred to them by ED physicians. At the Oakland ED, a different model was used to increase the number of persons offered testing. At intake in the ED, the triage nurse attempted to offer testing to all eligible patients (i.e., those who, when asked, said they were HIV negative or did not know their HIV status and who met consent requirements). ED staff members (usually treatment nurses), obtained written consents from those who agreed to testing, provided pretest information (i.e., an informational handout), and administered the HIV tests, in addition to their usual responsibilities. In New York and Los Angeles, both negative and positive rapid test results were provided to patients by HIV counselors; in Oakland, negative rapid test results were provided by nurses, but positive rapid results were provided by HIV counselors (on weekdays) and ED physicians (during nights and on weekends). At all three sites, confirmatory specimens were collected immediately upon receipt of a positive rapid test result; confirmatory results were provided approximately 1 week later by HIV counselors either in the ED (Los Angeles and New York) or at hospital-affiliated clinics (Los Angeles, New York, and Oakland). At all three sites, persons with confirmed positive HIV test results were provided further HIV risk-reduction information, partner counseling and referral services, and medical care appointments. Consent forms, counseling, and other services were made available in English and Spanish. Staff members assisted patients with referrals to providers and services elsewhere if the patients were not local residents or requested services at other facilities. In New York and Los Angeles, project staff members performed chart reviews to collect follow-up data. In Oakland, information was collected through an active follow-up process involving project staff from the ED and a linkage coordinator from an affiliated HIV clinic. During the study periods, HIV testing was offered to 34,627 (18.6%) of 186,415 persons who sought care at the three participating EDs (Table 1). The proportion of ED patients offered HIV testing varied by site: 47.7% in Oakland, 3.6% in Los Angeles, and 2.1% in New York. Overall, 19,556 (56.5%) of those offered testing agreed to be tested; however, the proportion of persons accepting testing varied by site: 98.3% in Los Angeles, 84.0% in New York, and 52.8% in Oakland. The proportion of patients actually tested during the ED visit among those who agreed to testing also varied by site: 99.8% in Los Angeles, 99.4% in New York, and 38.5% in Oakland. Among the 97 patients with newly diagnosed HIV infection, 85 (88%) were then linked to health-care services, defined as having at least one medical follow-up visit for HIV care and treatment (Table 1). The proportion of tested patients with newly diagnosed HIV infection varied by site: 0.8% in Los Angeles, 1.0% in Oakland, and 1.5% in New York (Table 1). Patients tested at the three sites differed by sex, age, race/ethnicity, and HIV test result. Overall, by racial/ethnic group, among the 97 with newly diagnosed HIV infection, 50 (52%) were non-Hispanic black, 28 (29%) were Hispanic, 12 (12%) were non-Hispanic white, four (4%) were Asian/Pacific Islander, and the race/ethnicity for three patients was unknown (Table 2). Risk information was available for 95 (98%) of those with newly diagnosed HIV infection; 49 (52%) of those persons reported having at least one of the following risks for HIV transmission during the previous 12 months: male-to-male sexual contact, injection-drug use, commercial sex work, or a sexually transmitted disease (STD) diagnosis. Reported by: EE Telzak, MD, F Grumm, J Coffey, MD, Bronx Lebanon Hospital Center, New York, New York. DAE White, MD, AN Scribner, MPH, Alameda County Medical Center, Oakland; S Quan, MPH, A Martinez, Rand Schrader Health & Research Center, Los Angeles; M Esquivel, R Merrick, County of Los Angeles Dept of Health Svcs, California. B Boyett, MS, JD Heffelfinger, MD, J Schulden, MD, B Song, MS, PS Sullivan, PhD, Div of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC. Editorial Note:The findings in this report suggest that offering HIV testing as an integrated part of routine health-care services in EDs, rather than relying on a clinical- or risk-based approach to testing, is a feasible strategy for identifying persons with previously undiagnosed HIV infection who might not otherwise access HIV-testing services. The majority of patients (56.5%) offered HIV testing at the three sites agreed to be tested, indicating that opt-in testing is acceptable in ED settings. If a risk-based approach to testing (e.g., testing only those persons reporting male-to-male sexual contact, injection-drug use, commercial sex work, or STD diagnoses) had been used in these three ED demonstration projects, 48% of the persons with newly diagnosed HIV infection would not have been offered testing. Overall, 88% of persons with newly diagnosed HIV infection were linked to health-care services after diagnosis, a proportion that compares favorably with previous reports (4). Substantially higher proportions of patients were offered HIV testing and subsequently tested at the Oakland ED than at the Los Angeles and New York EDs. Using a counselor-based approach to testing resulted in >90% of patients accepting testing when offered at the Los Angeles and New York sites; however, the number of persons offered testing (<4%) in these EDs was limited by the number of available HIV counselors. Nonetheless, the use of dedicated counselors in EDs enabled the Los Angeles and New York sites to increase the number of patients tested for HIV infection from 21 in 2003 to 1,709 in 2005 and from 415 in 2003 to 1,288 in 2005, respectively. In Oakland, use of existing staff members to offer testing resulted in approximately half of ED patients offered testing; however, only 52.8% of those offered testing accepted it, and only 38.5% of those who accepted testing were actually tested, largely because of limited staff. Persons who agreed to testing but could not be tested during their ED visit in Oakland were referred to other hospital departments, clinics, or community-based organizations for testing. Despite the low acceptance of testing, the Oakland testing approach was most feasible for maximizing the number of patients tested. The number of ED patients tested for HIV infection increased from 307 in 2004 to 6,368 during April 2005--March 2006. Revised CDC recommendations for HIV testing in health-care settings were published in September 2006 (5), 5 months after the end of the study period described in this report. The revised recommendations call for HIV testing to become a routine part of medical services using a voluntary, opt-out approach to ensure that persons with HIV infection are identified and linked to care and prevention services early in the course of their infection and to foster improved long-term prognosis and reduced transmission to others (5). Under the opt-out approach recommended in the revised guidelines, patients are notified that HIV testing is a routine part of services offered to all patients aged 13--64 years and will be performed unless the patient declines to be tested. Such an approach has been accepted and effective among pregnant women (6). Several analyses have supported the cost-effectiveness of routine testing in clinical settings, even in communities with a low prevalence of HIV infection (7,8). In addition, routine testing might reduce the stigma associated with identifying persons for testing on the basis of actual or perceived risk behaviors (9,10). Although this report describes HIV testing offered to patients in EDs on a voluntary opt-in basis, it provides insight into methods that could be used to implement testing using an opt-out approach. The findings in this report are subject to at least two limitations. First, HIV testing was not offered to all patients or to a statistical sample of patients visiting the participating sites; therefore, those who were tested might not be representative of all persons seeking medical care at these or other EDs. Second, data on linkage to follow-up health care might not include information for some patients who sought care outside of the three EDs described in this report. Additionally, some patients might not have sought care until after data for these projects were collected. Therefore, the reported proportion of persons with newly identified HIV infection who were linked to care is a minimum estimate. Although the results from these projects are preliminary, they demonstrate that integrating HIV testing into the routine care provided in EDs can identify persons with previously undiagnosed HIV infection. Routine testing might increase the linkage of HIV-positive persons to health and prevention services earlier in the course of infection, which might result in improved long-term prognosis and reduced HIV transmission. The two testing protocols described in this report had advantages and disadvantages. Use of a counselor-based approach to HIV testing (Los Angeles and New York) enabled in-depth assessment of risk behaviors and discussion of prevention strategies with patients but limited the number of patients who could be tested. Use of existing staff members (Oakland) enabled offering HIV testing to more patients but resulted in lower acceptance. A combined approach, using dedicated HIV testing personnel in collaboration with existing staff members, might increase testing capacities in EDs, maintain a high rate of acceptance of HIV testing, and facilitate implementation of the opt-out testing approach outlined in the revised CDC recommendations for HIV testing in health-care settings (5). References
* Information regarding sensitivity (99.3%) and specificity (99.8%) for the OraQuick Advance test is available at http://www.orasure.com/uploaded/398.pdf. The OraQuick Advance rapid test requires 20 minutes to process a specimen. Test results must be read after the 20-minute processing period has elapsed, but not more than 40 minutes after the test was initiated. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 6/21/2007 |
|||||||||
|