|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
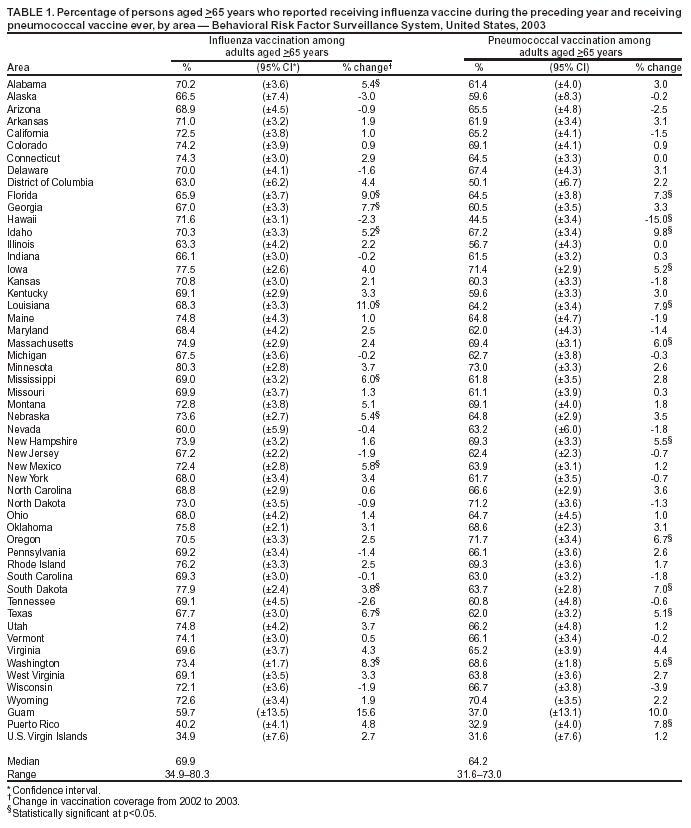
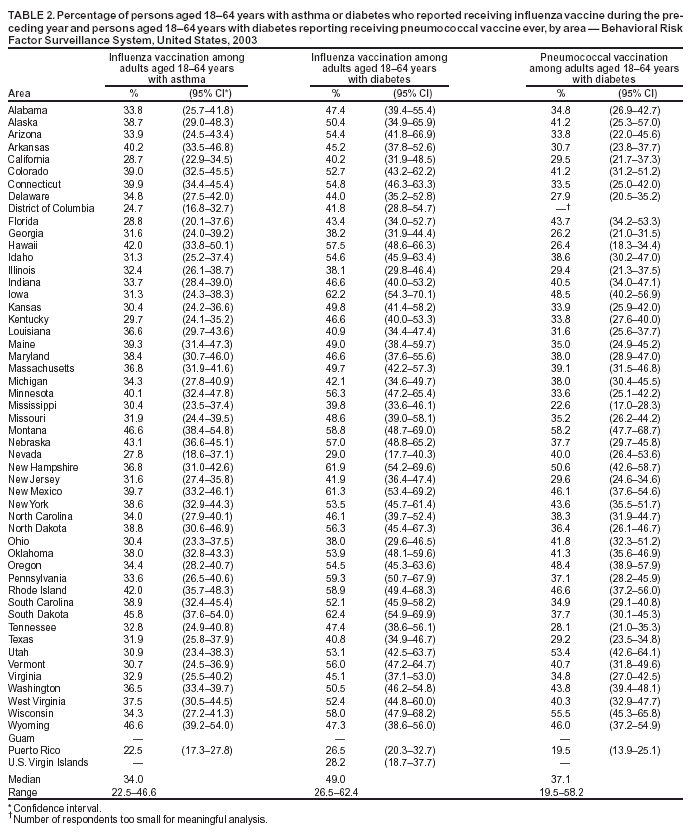
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Influenza and Pneumococcal Vaccination Coverage Among Persons Aged >65 Years and Persons Aged 18--64 Years with Diabetes or Asthma --- United States, 2003Please note: An erratum has been published for this article. To view the erratum, please click here.Vaccination of persons at risk for complications from influenza and pneumococcal disease is a key public health strategy for preventing associated morbidity and mortality in the United States. Risk factors include older age and medical conditions that increase the risk for complications from infections. During the 1990--1999 influenza seasons, more than 32,000 deaths each year among persons aged >65 years were attributed to complications from influenza infection (1). National health objectives for 2010 call for 90% influenza and pneumococcal vaccination coverage among noninstitutionalized persons aged >65 years and 60% coverage among noninstitutionalized persons aged 18--64 years who have risk factors (e.g., diabetes or asthma) for complications from infections (2) (objective nos. 14.29a--d). To estimate influenza and pneumococcal vaccination coverage among these populations, CDC analyzed data from the 2003 Behavioral Risk Factor Surveillance System (BRFSS) survey*. This report summarizes the results of that analysis, which indicated that 1) influenza vaccination levels among adults aged 18--64 with diabetes or asthma, 2) pneumococcal vaccination levels among adults aged 18--64 years with diabetes, and 3) influenza and pneumococcal vaccination levels among adults aged >65 years all were below levels targeted in the national health objectives for 2010. Moreover, vaccination coverage levels varied among states for both vaccines and both age groups. Innovative approaches and adequate, reliable supplies of vaccine are needed to increase vaccination coverage, particularly among adults with high-risk conditions. BRFSS is a state-based, random-digit--dialed telephone survey of the U.S. civilian, noninstitutionalized population aged >18 years. All 50 states, the District of Columbia (DC), and three U.S. territories participate in the survey. Respondents were asked, "During the past 12 months, have you had a flu shot?" and "Have you ever had a pneumonia shot?" Persons with diabetes were defined as respondents who answered "yes" to the question, "Have you ever been told by a doctor that you have diabetes?" Women who were told that they had diabetes only during pregnancy were not defined as having diabetes. Participants were also asked, "Have you ever been told by a doctor, nurse, or other health professional that you had asthma?" Those who responded "yes" were then asked, "Do you still have asthma?" Respondents who answered affirmatively to both questions were classified as having asthma. For the 2003 BRFSS, the median state/area response rate was determined to be 53.2% (range: 34.4%--80.5%) by using the CASRO method. A total of 266,346 persons responded, of whom 207,735 (83.0%) were aged 18--64 years and 56,547 (17.0%) were aged >65 years. Among respondents aged 18--64 years, 17,084 (7.8%) reported having asthma and 12,412 (5.7%) reported having diabetes. Respondents with unknown influenza (0.3%) or pneumococcal (7.0%) vaccination status were excluded from the analysis. Vaccination levels were estimated for the 50 states, DC, Guam, Puerto Rico, and the U.S. Virgin Islands (USVI). Data were weighted by age, sex, and, in certain states/areas, race/ethnicity to reflect the estimated adult population. Statistical software was used to calculate point estimates and 95% confidence intervals. In 2003, of respondents aged >65 years, influenza vaccination coverage levels during the preceding 12 months ranged from 34.9% (USVI) to 80.3% (Minnesota), with a median of 69.9% (Table 1). Among respondents aged >65 years, the proportion reporting ever having received pneumococcal vaccine ranged from 31.6% (USVI) to 73.0% (Minnesota), with a median of 64.2%. Compared with 2002, a total of 41 and 38 states/areas experienced increases in influenza and pneumococcal coverage among those aged >65 years, respectively; 11 of these increases were statistically significant for each vaccine. Among adults aged 18--64 years with asthma or diabetes, substantial variation in vaccination coverage by area also was observed. For respondents with asthma, median influenza coverage was 34.0% and ranged from 22.5% (Puerto Rico) to 46.6% (Wyoming) (Table 2). Influenza vaccination rates among persons with asthma were higher among persons aged 50--64 years (median: 53.4%; range: 27.6%--74.9%) than among persons aged 18--49 years (median: 27.7%; range: 16.6%--41.1%). For respondents with diabetes, median influenza coverage was 49.0% and ranged from 26.5% (Puerto Rico) to 62.4% (South Dakota); the median pneumococcal coverage was 37.1% and ranged from 19.5% (Puerto Rico) to 58.2% (Montana). For persons with diabetes, vaccination rates were higher among those aged 50--64 years (for influenza, median: 56.5%; range: 23.7%--73.1% and for pneumococcal, median: 42.6%; range: 19.7%--68.1%) than among persons aged 18--49 years (for influenza, median: 37.8%; range: 22.2%--59.9% and for pneumococcal, median: 28.3%; range: 13.3%--56.7%). Reported by: BH Bardenheier, MPH, MA, PM Wortley, MD, Immunization Svcs Div; G Euler, DrPH, Epidemiology and Surveillance Div, National Immunization Program, CDC. Editorial Note:The findings in this report indicate an increase in influenza and pneumococcal vaccination coverage for the majority of areas from 2002 to 2003 among adults aged >65 years; however, coverage among persons indicated for these vaccinations remains below the national health objectives for 2010. In addition, almost half of the states reported >50% influenza coverage levels for participants aged 18--64 years with diabetes; however, the median coverage level of influenza vaccination among participants with asthma and the median coverage level of pneumococcal vaccines among participants with diabetes were below the 2010 target of 60% for noninstitutionalized adults at high risk. Among respondents with asthma and diabetes, those aged 18--49 years had substantially lower vaccination coverage than those aged 50--64 years. Lack of awareness of the need for vaccination is common among adults aged <65 years with high-risk conditions, such as diabetes or asthma. In a 2003 survey, approximately 75% of unvaccinated persons aged 18--64 years with diabetes reported that they were unaware of the need for influenza vaccine (CDC, unpublished data, 2003). Although use of preventive health services by adults with diabetes has increased since 1995 (3), a substantial proportion of generalist and subspecialist physicians did not strongly recommend influenza and pneumococcal vaccinations to their patients who are elderly or at high risk (4). Low vaccination rates among persons with high-risk conditions might reflect the challenge of targeting patients for vaccinations on the basis of high-risk conditions instead of age (1). Although a majority of patients seen by subspecialists might be those who most need vaccination, subspecialists might not perceive the provision of preventive services as their role. Primary care physicians and subspecialists should work together to ensure that persons at high risk receive appropriate vaccinations. In addition, strategies to increase awareness among young adults of the need for vaccinations could be emphasized by diabetes- and asthma-care programs (3,5). The Diabetes Quality Improvement Project, a collaborative effort between public and private organizations to improve preventive care for persons with diabetes, has been ongoing since 1995 (6); this effort is one possible reason for the higher influenza vaccination rates among those with diabetes compared with those with asthma. The findings in this report are subject to at least three limitations. First, vaccination status (influenza and pneumococcal) was based on self-report and not validated. The validity of self-reported pneumococcal vaccination is lower than that of influenza vaccination (7). Second, the median BRFSS response rate (53.2%) in this survey was low. BRFSS results have been compared with results from the National Health Interview Survey (NHIS), a household-based, face-to-face interview survey with higher response rates. Comparisons demonstrate similar trends and subgroup differences; however, BRFSS vaccination estimates are consistently higher than NHIS estimates (8). Finally, because BRFSS does not systematically assess other medical conditions for which influenza and pneumococcal vaccines are recommended, vaccine coverage for all persons with high-risk conditions was not examined. The variation in influenza and pneumococcal vaccination coverage observed among areas suggests that vaccination coverage can be improved. Previous studies have indicated that organizational changes, such as nurse standing orders, combined with teamwork and collaboration, are effective intervention measures for increasing adult vaccination services (9). Effective measures to promote the use of such measures are needed for vaccination rates to increase. Because of the 2004 influenza vaccine shortage, vaccine providers have been asked to direct available inactivated influenza vaccine to persons with chronic conditions, such as diabetes and asthma, and other priority groups. Further analysis of influenza vaccine coverage data will be needed to assess the impact of this shortage on influenza vaccine coverage and efforts to redirect vaccine to persons at greatest risk for influenza complications. Ensuring adequate amounts of influenza vaccine is critical if vaccination rates of persons at high risk are to continue improving. Pneumococcal vaccine supplies appear to be adequate to meet expected demand. Pneumococcal vaccination should be encouraged for populations at high risk, both to reduce the risk for invasive pneumococcal disease itself and to reduce complications of influenza infection. References
* Conditions ascertained by BRFSS that are indicated for vaccination include asthma (indicated for influenza vaccine) and diabetes (indicated for influenza and pneumococcal vaccines).
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/4/2004 |
|||||||||
This page last reviewed 11/4/2004
|