|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
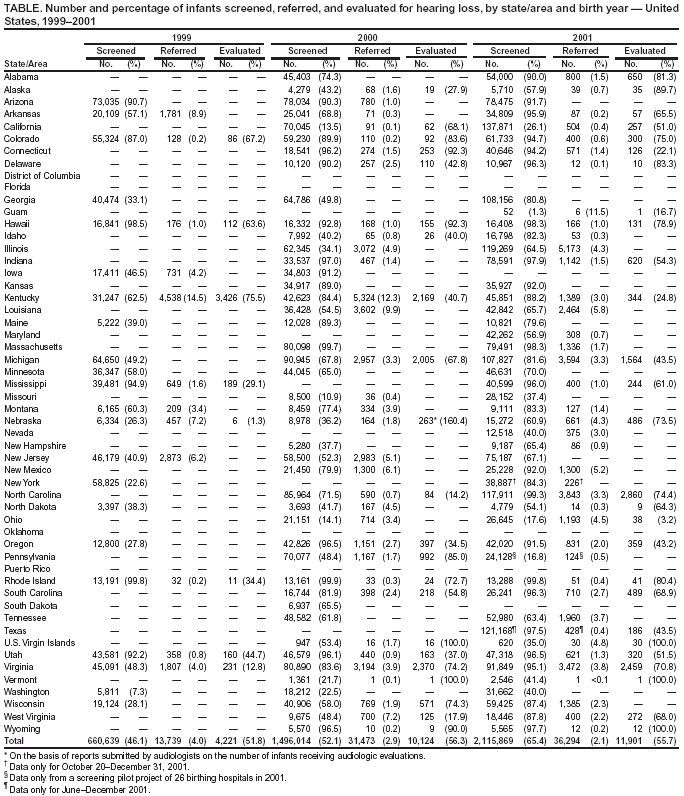
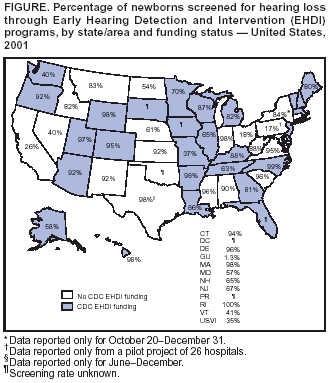
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Infants Tested for Hearing Loss --- United States, 1999--2001Please note: An erratum has been published for this article. To view the erratum, please click here. Hearing loss (HL) occurs in one to three of 1,000 live births annually (1,2) and, when left undetected, can result in developmental delays (3,4). To promote communication from birth, Early Hearing Detection and Intervention (EHDI) programs support early identification of infants with HL. Without EHDI programs, the average age of identification for HL is age 1.5--3.0 years (2,5,6), which is past the start of the critical period for optimal language acquisition (7,8). In 2001, a total of 48 states/areas with EHDI tracking and surveillance systems (30 funded by CDC) reported the percentage of newborns screened for HL (Figure). This report summarizes the results of an analysis of surveillance data for 1999--2001, which indicate that more infants were screened for HL, received diagnostic audiologic evaluations, and were enrolled in early intervention services in 2001 than in 1999 and 2000. Continued development of EHDI surveillance systems should assist states/areas in providing needed services to children with HL. Benchmarks for the key components of the EHDI process include hearing screening before age 1 month, diagnostic audiologic evaluation before age 3 months for infants who do not pass the screening, and enrollment of infants identified with HL in early intervention services before age 6 months. These benchmarks form the basis of the "1-3-6" plan that state/area EHDI programs are implementing. States/areas with EHDI programs are collecting data on the numbers of infants screened, evaluated, and enrolled in intervention services. In collaboration with Directors of Speech and Hearing Programs in State Health and Welfare Agencies, CDC requested data for 1999--2001 from the 50 states, the District of Columbia, Guam, Puerto Rico, and the U.S. Virgin Islands. Responses were received from 22 states/areas in 1999, from 46 in 2000, and from 52 in 2001. In 1999, a total of 726 (49%) hospitals and birthing centers in the 22 reporting states/areas were classified as universal newborn hearing screening (UNHS) facilities (i.e., facilities in which the majority of infants were screened). The percentage of infants screened needed to achieve UNHS classification varied. The 22 states/areas reported that 660,639 (46.1%; range: 7.3%--99.8%) of 1,433,780 newborns were screened for HL (Table). In addition, 12 jurisdictions reported referral rates (i.e., percentage of screened newborns referred for audiologic evaluation). An average of 4.0% (range: 0.2%--14.5%) of screened infants were reported to have been referred for audiologic evaluation; eight states/areas reported that 4,221 (51.8%; range: 1.3%--75.5%) of 8,145 referred infants received an audiologic evaluation. In 2000, a total of 46 states/areas reported that 1,976 (59.7%) of 3,312 hospitals and birthing centers were classified as UNHS facilities, and 44 reported that 1,496,014 (52.1%; range: 10.9%--99.9%) of 2,872,869 newborns were screened for HL (Table). In 2001, a total of 52 states/areas reported that 2,656 (73.2%) of 3,628 hospitals and birthing centers were classified as UNHS facilities, 48 reported that 2,115,869 (65.4%; (range: 1.3%--99.8%) of 3,232,914 newborns were screened for HL, 40 reported an average referral rate of 2.1% (range: 0.4%--11.5%), and 27 reported that 11,901 (55.7%; range: 3.2%--100%) of 21,377 newborns referred for screening received an audiologic evaluation (Table). In the 21 states/areas that reported screening data for both 1999 and 2001, the number of newborns who received a hearing screening during this period increased by an estimated 35%. For the 10 states/areas that reported data on infants referred for audiologic evaluation for 1999 and 2001, referral rates were low*, decreasing from 4.0% in 1999 to 2.0% in 2001. These rates are consistent with the National EHDI and Joint Committee on Infant Hearing goal of referring <4.0% (objective nos. 1.7 [9] and 5[a]2 [10]) of children tested. Eight states/areas reported audiologic evaluation data in both 1999 and 2001; the number of infants receiving an evaluation increased by approximately 9% during this period. For 1999, five states/areas reported that 179 infants were identified with HL; 108 (60.3%) were enrolled in early intervention programs by age 6 months. In 2001, 25 states/areas reported that 1,354 infants were identified with HL; 879 (64.9%) were enrolled in early intervention programs. Of these 879 enrolled infants, 627 (71.3%) reportedly were enrolled by age 6 months. Reported by: M Gaffney, M Gamble, MPH, P Costa, MS, J Holstrum, PhD, C Boyle, PhD, Div of Human Development and Disability, National Center on Birth Defects and Developmental Disabilities, CDC. Editorial Note:In 2001, approximately three times as many infants were reported to have been screened for HL and to have received audiologic evaluations than were reported in 1999. However, the number of infants evaluated and enrolled in intervention services was low. In 2001, nearly half of the infants referred for audiologic evaluation reportedly did not receive an audiologic evaluation, and approximately one third of infants identified with HL were not reported to be enrolled in intervention services. Although this finding is attributable in part to loss to follow-up and differing reporting requirements, the data indicate the need to strengthen EHDI programs. Continuing to develop tracking and surveillance systems, ensuring that such systems are linked to diagnostic and intervention services, including medical home, and implementing consistent methods for reporting by health-care providers should enable states/areas to capture EHDI-related data for all newborns. The variation in reported rates is attributable to several factors. States/areas began implementing EHDI programs at different times. Certain states/areas have mandated screening, but requirements vary. Although 22 states/areas indicated that newborn hearing screening legislation was passed or implemented by 2000, not all require reporting of data to the respective EHDI program. In addition, in 20 (40%) of 50 states/areas reporting in 2001, >10% of hospitals and birthing facilities were not designated as UNHS facilities, which affected the number of children screened. The reasons for not screening all newborns include financial constraints and policy issues (e.g., hospitals with fewer annual births not being required to screen). In addition, large annual birth populations, geographic barriers, and differing eligibility requirements for receiving services might affect the ability to provide EHDI-related services. The findings in this report are subject to at least five limitations. First, certain states/areas (31 in 1999, seven in 2000, and two in 2001) did not have the requested data or did not respond. Second, some states/areas that reported data were unable to determine if infants had been screened or evaluated before the recommended age intervals. Third, three states/areas in 2001 were able to report only partial data or data from a limited number of hospitals. Fourth, data for the 3 reporting years were too limited to report the age of identification, severity of HL, or whether the HL was detected in one or both ears. Finally, although states/areas were requested to provide actual data, some might have submitted estimates. The findings in this report underscore the need for EHDI programs to ensure that infants with HL are detected rapidly and enrolled in early intervention services. Surveillance data can help in assessing polices and procedures and ensuring that infants with HL are identified as early as possible and enrolled in appropriate intervention programs. These activities will help children with HL develop communication skills commensurate with their cognitive abilities. Acknowledgments This report is based on data provided by Directors of Speech and Hearing Programs in State and Health Welfare Agencies in Alabama, Alaska, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Guam, Hawaii, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, U.S. Virgin Islands, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, and Wyoming. References
* Low referral rates are an indication that screenings are being performed correctly and are important in maintaining both public and professional confidence in the accuracy of screening results.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 10/16/2003 |
|||||||||
This page last reviewed 10/16/2003
|