
Two Career Fire Fighters Die after Falling From Elevated Aerial Platform - Texas
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2009-06 Date Released: July 13, 2009
Revised on March 24, 2014 to reword Recommendation #5 to address who should provide fall protection
SUMMARY
On January 25, 2009, two male career fire fighters, age 28 (Victim #1) and age 45 (Victim #2), died after falling from an elevated aerial platform during a training exercise in Texas. The fire fighters were participating in the exercise to familiarize fire department personnel with a newly purchased 95-foot mid-mount aerial platform truck. A group of four fire fighters were standing in the aerial platform which was raised to the roof of an eight-story dormitory building at a local college. The platform became stuck on the concrete parapet wall at the top of the building. During attempts to free the platform, the top edge of the parapet wall gave way and the aerial ladder sprung back from the top of the building, then began to whip violently back and forth. Two of the four fire fighters standing in the platform were ejected from the platform by the motion. They fell approximately 83 feet to the ground and died from their injuries.

|
|
Aerial platform positioned at dormitory building |
Key contributing factors identified in this investigation include the fire fighters being unfamiliar with the controls on the newly purchased aerial platform truck, training in a “high risk” scenario before becoming familiar with new equipment, failure to use fall restraints, the design of the platform railing and integrated doors, and the location of the lifting eyes underneath the platform which contributed to the platform snagging on the building’s parapet wall.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
- Ensure fire fighters are fully familiar with new equipment before training under “high risk scenarios.”
- Ensure fall protection is used whenever fire fighters and other personnel are working in elevated aerial platforms.
- Follow standard operating procedures (SOPs) for training, including the designation of a safety officer.
- Ensure SOPs covering the operation and use of fire apparatus (including aerial platform apparatus) are developed and followed during training exercises as well as in fire suppression activities.
- Provide fall protection belts with all aerial ladder and platform apparatus and ensure that fall protection is used in both training exercises and emergency response events.
Fire apparatus manufacturers should:
- Include the use of fall protection in both demonstration and training programs.
- Ensure that aerial platforms and other aerial devices are designed to reduce or eliminate the potential for snagging on buildings or other elevated surfaces.
- Ensure aerial platform doors or gates are designed to prevent opening in the outward direction.
INTRODUCTION
On January 25, 2009, two male career fire fighters, age 28 (Victim #1) and age 45 (Victim #2), died after falling from an elevated aerial platform during a training exercise in Texas. On January 26, 2009, the NIOSH Fire Fighter Fatality Investigation and Prevention Program (FFFIPP) became aware of the fatal incident through the national media. The U.S. Fire Administration (USFA) notified the NIOSH Division of Safety Research (DSR) of the fatalities the same day. The city and fire department restricted access to the fire apparatus following the January 25, 2009 incident. NIOSH contracted with a fire service consultant knowledgeable in fire apparatus operations, performance and equipment requirements to assist with the investigation. The City Manager requested that NIOSH coordinate the inspection of the fire apparatus with the city’s insurance carrier. On February 4, 2009, two NIOSH engineers and the consultant traveled to Texas and met with representatives of the fire department, the city’s insurance carrier, and the fire apparatus manufacturer. The fire apparatus involved in this incident was inspected, photographed and measurements of the platform were taken. The manufacturer provided NIOSH investigators with copies of their mid-mount apparatus operator’s manual, the training program provided to the fire department, and the training attendance list. The apparatus was driven to the site of the incident (by fire department personnel) and the aerial platform was raised to the roof of the dormitory building. Since the local police investigators had accurately marked the location of the apparatus at the time of the incident, the apparatus was able to be positioned almost exactly as it had been positioned at the time of the incident. Note: Some photographs used in this NIOSH report have been altered to remove names, faces, and other identifiers.
On February 12, 2009, the NIOSH engineers and the consultant returned to Texas where interviews were conducted with the fire fighters who were involved in the training incident. The NIOSH investigators reviewed copies of the fire department’s standard operating procedures (SOPs), building information, and training records for the two victims.
FIRE DEPARTMENT
The combination fire department involved in this incident serves a population of approximately 20,000 residents in an area of approximately 126 square miles. The fire department had a total of 37 paid career fire fighters and volunteer fire fighters at the time of the incident. The fire department is supervised by an Operations Chief who reports to the city Public Safety Director who oversees both the fire and police departments in the city. In addition to the 37 line fire fighters, the fire department has an administrative staff which includes the Operations Chief, a Deputy Chief who oversees training, and a Fire Marshal. The Operations Chief or the Deputy Chief serves as the safety officer at major incidents.
The fire department operates 10 fire apparatus that respond from three fire stations. At the time of the incident, one fire station was being remodeled so the fire department was temporarily operating from two stations. Twelve fire fighters are assigned to A and C shifts and 13 fire fighters are assigned to B shift (total of 37 fire fighters on 3 shifts). The fire department can operate with a minimum-staffing level of 10 members on duty each shift. The fire department provides fire fighting, basic life support (BLS) emergency medical services, vehicle rescue, and search and rescue services to the community.
TRAINING and EXPERIENCE
In the state of Texas, specific training requirements are determined by each fire department. The combination fire department involved in this incident required both Texas Basic Fire Fighter and Emergency Medical Technician (EMT) certification plus a high school diploma or a GED in order to become a fire fighter. The state of Texas offers state fire fighter certification, roughly equivalent to National Fire Protection Association (NFPA) Level II Fire Fighter certification, through a number of accredited programs at universities and colleges across the state. Additional training provided by the fire department involved mostly hands-on training in basic fire fighting operations, tactics and procedures. This fire department’s assistant chief serves as the designated training officer.
Records provided by the fire department indicated that Victim #1 had been a fire fighter with the department since February 2008 and had completed 101 hours of training. Victim #2 had been with the fire department since July 2004 and had completed 388.5 hours of training.
On November 19, 2008, the fire department received delivery of a newly manufactured 2008 model, 95-foot mid-mount aerial platform apparatus. Each of the three duty shifts received a factory-authorized training program of approximately 8 hours, including both classroom and practical exercises on December 13, 14 and 15. The hands-on training included raising the aerial platform into the air with fire fighters in the platform. During the NIOSH interviews, some fire fighters reported that the training was interrupted by response to fire and medical calls, but the full 8 hours of training were received by each shift. Fire fighters interviewed by NIOSH reported that fall protection was not used during this training. Both victims attended the 8-hour training session on December 14, 2008 provided by the fire apparatus manufacturer, as did the fire fighter who was operating the platform controls at the time of the incident. Note: The fire fighter selected to operate the platform controls at the time of the incident was off-duty due to an injury to his hand, but attended the December 14, 2008 training provided by the apparatus manufacturer. When interviewed by NIOSH investigators, this fire fighter stated the day of the incident was the third time he had operated the aerial platform controls. Most fire fighters interviewed by NIOSH stated they felt the classroom training was adequate.
After completing the factory training, each shift practiced and drilled with the new apparatus as time permitted. Fire fighters interviewed by NIOSH investigators reported taking the apparatus out in front of the station and setting it up a number of times. They also reported taking the apparatus to the local football field, elevating the platform and flowing water on at least one occasion.
SAFETY and HEALTH REGULATIONS
Texas is one of 24 states and territories that fall under the jurisdiction of the U.S. Department of Labor, Occupational Safety and Health Administration (OSHA), i.e., Texas is not under a state-OSHA plan. Fire departments in the state of Texas are covered by the Texas Commission on Standards and Education. The commission publishes standards that are to be followed by fire departments in the state of Texas. Fire departments can adopt more stringent standard operating procedures but cannot have a standard less restrictive than the state fire commission requirements. The state fire commission has adopted some, but not all, National Fire Protection Association (NFPA) standards pertaining to fire fighting operations, equipment and programs.
FIRE APPARATUS
The apparatus involved in this incident was the first platform apparatus utilized by the fire department and was purchased to replace a straight 110′ aerial ladder truck.
Apparatus Configuration
The apparatus involved in this incident is a 2008, custom fire apparatus with a 95-foot mid-mounted aerial ladder platform. The aerial device is constructed of welded aluminum alloy extrusions assembled in four sections. The vehicle is stabilized by two sets of down jacks and one set of under-slung outriggers. All are hydraulically operated with an electronic automatic leveling system.
The aerial ladder can be operated from each of two ladder control consoles – one located at the base (right side) and one located in the platform at the ladder tip. The aerial ladder movements of raise/lower, extend/retract and rotation are powered hydraulically with electric-over-hydraulic controls located at both control consoles. This type of hydraulic control incorporates an electronic solenoid that opens and closes a hydraulic valve directing fluid to the operating pistons. An adjustable delay is incorporated in the system to reduce the shock load on the aerial ladder from the hydraulic valve operating from the fully closed to the fully open position and vise versa. Unfamiliarity with the operational delay can result in jerky or unsteady movements when inexperienced operators handle the controls.
The platform is constructed of welded aluminum extrusions and aluminum sheet with approximately 18 square feet of floor space. The platform payload is rated at 1,305 pounds without water in the system (1000 lbs. – personnel and 305 lbs. – equipment) and 805 pounds wet (water in the system – 500 lbs. personnel and 305 lbs. equipment). A 42″ high guard railing is provided around the perimeter of the platform. Two inward-opening, self-closing doors are provided at the two front corners of the platform. Six fall-protection anchor points are located in the platform, two in the front, two on the sides and two in the rear (see Photo 1 and Photo 2).
A ManSaverT Aerial Bara encloses the rear ladder opening. The bottom side of the platform is equipped with a water curtain nozzle designed to provide a fine water spray below the platform to protect the platform and occupants from flame impingement.
 |
 |
|
Photos 1 and 2. Photo 1 shows anchor point on left side of platform (1 of 6 inside platform). Photo 2 shows the ManSaverT Aerial Bar located to separate the platform from the ladder. Also note anchor point at rear of platform to left of the ManSaverT Aerial Bar in Photo 2.
NIOSH photos. |
|
NFPA Standards Compliance
The NFPA Standard that governed the construction of the aerial apparatus in 2008 was NFPA 1901 Standard for Automotive Fire Apparatus, 2003 Edition.2
The following NFPA requirements dealing with the construction of the platform that are pertinent in this incident were:
20.7.6.1.1
- Minimum floor area in platform, 14 square feet.
20.7.6.1.2
- A continuous guard railing, a minimum of 42 in. high on all sides.
20.7.6.2.2.1
- A minimum of two gates to provide access to the platform.
20.7.6.2.2.2
- Each gate provided with a self-engaging latch.
20.7.6.2.2.3
- Inward opening, self-closing gates or doors for access to and from the platform permitted to meet the continuous railing requirement.
20.7.6.8.1
- Provisions shall be made so that personnel working on the platform can attach fall protection harness.
The following NFPA requirements dealing with the apparatus that are pertinent in this incident were not met:
8.8.1
- The equipment listed in 8.8.2 and 8.8.3 shall be available on the aerial fire apparatus before the apparatus is placed in service.
8.8.2b
- Aerial fire apparatus shall be equipped with at least the following equipment: (1 through 17.) (18) Four ladder belts meeting the requirements of NFPA 1983, Standard on Fire Service Life Safety Rope and System Components.3 (19 through 27.)
8.8.3c
- If the aerial fire apparatus is equipped with a fire pump, the requirements of 8.8.3.1 through 8.8.3.3 shall apply
Note: At the time of the incident, NFPA 1901 had not been adopted by the Texas Commission on Standards and Education.
a ManSaverT is a registered trademark of Fire Research Corp. The Aerial Bar is a variation on the standard ManSaverT. The Aerial Bar is a safety bar that can be mounted at the end of the ladder across the opening to the bucket. Like the standard ManSaverT, it is spring loaded so an operator does not have to remember to close or latch it. This uncovered bar has a stainless steel U-shaped tube welded to it to cover more area and to help prevent a person from slipping underneath the bar. It is designed for use at the top of an aerial device, at the back of the “bucket” where the ladder leads down to the elevated turntable. The ladder is often at precarious angles, and an accidental fall from the bucket during operations could cause serious injury.1
b NFPA 1901, Chapter 8.8.2 identifies the required number and type of various hand tools, portable lights, portable fire extinguishers, SCBA, spare SCBA cylinders, wheel chocks, plastic traffic cones, personal protective equipment, safety equipment, and miscellaneous items required to be carried on aerial fire apparatus.
c NFPA 1901, Chapter 8.8.3.1 through 8.8.3.3 identifies specific hose connections, adaptors and related tools required.
STRUCTURE
The structure involved in this incident was an eight-story college dormitory building that was reported to be the highest structure in the city.
WEATHER
At the time of the incident, the weather conditions in the area were overcast with an approximate temperature of 46 degrees Fahrenheit, 61 percent relative humidity, visibility 10 miles, and east / northeast winds at approximately 5.8 miles per hour.4
INVESTIGATION
Three days before the incident, on January 22, 2009, the on-duty shift was receiving training in an unrelated subject from the Operations Chief when they were informed by the Chief that they should be doing additional training with the new aerial platform truck. That same night, the municipal fire department responded to a working structure fire at a local restaurant. Crews responded with the newly acquired Ladder One (L-1). L-1 had not yet been fully outfitted with all the necessary support equipment, so an engine was also dispatched so that the fire fighters would have access to all necessary tools and equipment. L-1 was used for master stream operations at the restaurant fire. During fire suppression operations, the electric motors that powered the monitor failed to operate so the monitor had to be operated manually. Following the fire, it was decided by the Operations Chief that additional hands-on training was needed to familiarize fire fighters with the operation of L-1, so a training exercise was planned by the shift supervisor and company officers to give all fire fighters on the shift more hands-on experience with L-1. The next work shift was a Sunday which meant there would be minimal traffic and activity at the local college. The fire department decided to take advantage of the light Sunday schedule and planned the training exercise for the eight-story college dormitory building that represented the highest building in the city.
On Sunday, January 25, 2009, all on-duty members of the fire department (ten fire fighters were on-duty) assembled at the college dormitory building at 1:00 PM for the scheduled training. A captain was serving as the acting battalion chief and a driver / engineer was serving as the acting captain to back-fill for the acting battalion chief.
L-1 was positioned in the parking lot in front of the dormitory building (see Diagram 1 and Photos 3 and Photo 4). The training exercise involved setting up the apparatus for operation (extending and setting the outriggers and leveling the apparatus) and then raising the platform to the roof of the eight-story structure. The first group of three fire fighters entered the aerial platform and raised the platform to the roof (using the controls located in the platform) where the fire fighters got out of the platform and briefly walked around on the roof, noting construction features, utilities, and other information that might be useful in the event the fire department had to respond to a fire call at the dormitory. The fire fighters re-entered the platform and lowered the platform to the nested position on the back of the apparatus. Two of the fire fighters exited the platform while the operator remained in the platform to demonstrate the operation of the controls to the next group of three fire fighters who entered the platform. The second group (4 fire fighters) raised the platform to roof level and stepped out of the platform onto the roof. After briefly surveying the roof, the second group of fire fighters re-entered the platform and began lowering it. They decided to set the platform on the ground to simulate a rescue procedure. The apparatus was positioned too close to the building to set the platform down on the grassy area in front of the dormitory so the aerial ladder was rotated 180 degrees and the platform was set down in the parking lot on the officer’s side of the apparatus where all four fire fighters stepped out of the platform.
 |
 |
|
Photos 3 and 4. Photo 3 shows an overhead view of the location of Ladder One. This is almost the exact position as at the time of incident. Note |
|
The remaining four fire fighters who had not previously been in the platform entered the platform. The four fire fighters decided which one of them would operate the controls and the aerial ladder was elevated and rotated to the right until the platform approached the wall of the dormitory building.
The platform operator attempted to see if he could perform more than one function simultaneously (elevate, rotate and extend the ladder) and found that he could not. He was informed by intercom from the ground that he was at full extension. The operator observed that the inclinometer in the platform indicated the ladder was at approximately 71 degrees of elevation as he rotated the platform to the right over the parapet wall. The operator told the other three fire fighters that the platform was too high above the roof for them to safely step out so he wanted to lower the platform. Fire fighters located on the ground as well as the survivors located in the platform reported hearing a sound like “metal scraping on concrete” followed by a sound described as a loud metallic “bang” or “thud” as the platform was lowered over the parapet wall. Note: It is theorized that these sounds were caused by the lifting eye scraping across the top of the parapet wall, followed by the platform dropping down onto the parapet wall after the lifting eyes cleared the top surface. After lowering the platform, the operator observed that the platform was resting on top of the parapet wall and told the other three fire fighters in the bucket to stay in the bucket as he wanted to lift the bucket off the parapet wall. The platform operator reported that the platform did not move as he featheredd the elevation control in an attempt to lift the platform. The operator attempted to feather the control again, but the platform did not move. Thinking the platform was slow in responding due to the inherent delay, the operator held steady pressure on the control. Note: The operator did not realize that the lifting eye located to his left on the underside of the platform was caught on the inner surface of the parapet wall and that attempts to elevate the platform were causing the lifting eye to be forced tighter against the inner surface of the parapet wall. Following the incident, scrape marks were evident on the aluminum lifting eye mounted under the platform on the left (passenger) side (see Photos 5 through Photo 7) The marks were both on the bottom and on the back side, suggesting that the lifting eye scraped along the top then dropped over the parapet wall. Immediately after the incident, aluminum fragments were recovered from a gouge in the parapet wall by police detectives (see Photo 8). Chunks of concrete matching the broken portion of the parapet wall were also found on the roof of the building by police detectives immediately after the incident (see Photo 9). Concrete debris was also observed on the water curtain spray nozzle located underneath the platform (see Photo 10). At this point, the platform operator was standing in the center of the bucket at the control panel, leaning outward and looking down to see what was restricting the platform from moving. Victim #1 was standing near the platform door to the operator’s right and Victim #2 was standing near the platform door to the operator’s left. The fourth fire fighter (acting captain) was standing behind and slightly to the left of Victim #1 (see Diagram 2).
On the third attempt to raise the platform off the parapet wall, the top inside edge of the parapet wall that was holding the lifting eye suddenly and without warning broke (see Photo 9), causing the platform to spring away from the building and then whip back and forth violently (see Photo 11).
Five fire fighters were standing on the apparatus near the turntable and were observing the operation of the aerial ladder as well as discussing the operation of the aerial base controls. Three of these fire fighters reported hearing the scraping sound and the loud thud. Fire fighters also observed the aluminum ladder bowing upward and twisting severely to the left. Note: The conditions described are consistent with having the platform caught on the building’s parapet wall and the elevating cylinders pressing up under the ladder attempting to raise the platform. One of the fire fighters standing on the ground observed the driver-side outrigger jacks (on the side closest to the building) lift off the ground. Other fire fighters standing on the apparatus felt the apparatus rock away from the building. One of these fire fighters yelled for another to shut off power to the platform control panel. A fire fighter standing on the ladder reached to his right and shut off the control power switches de-energizing both the base control and the platform control consoles, but the platform had already broken free of the parapet wall.
When the platform suddenly sprung free of the parapet wall, the aerial ladder and platform were propelled away from the building and the four fire fighters were thrown about within the platform. The platform operator felt himself slipping over the control panel and the railing as the platform whipped backward. He thrust his right knee under the control panel to keep himself from falling out. Note: The operator’s uniform hat was later found on top of the dormitory roof. When the aerial ladder reached its limit of motion away from the building, the fire fighters were tossed backward. The operator reported that his back struck against the ManSaverT Aerial Bar located at the rear of the platform. The aerial ladder then whipped forward (back toward the building), tossing the fire fighters in the platform forward. The operator was thrown against the control panel, striking his pelvis and again felt himself falling over the railing. As he struggled to remain in the platform by bracing his knee under the control panel, he observed Victim #1 falling through the right platform door, then he noticed a flash of blue in his peripheral vision to his left which he immediately realized was another fire fighter (Victim #2) falling through the left platform door. As the acting captain was tossed forward in the platform, he observed Victim #1 falling out of the platform through the right platform door. Just as Victim #1 was falling through the door, it appears the acting captain’s chest struck the intercom speaker at the right side of the control panel, knocking the acting captain straight down onto the floor of the platform with his head and shoulders hanging outward through the open doorway (see Photos 12 and 13 showing damage to ManSaverT Aerial Bar and the speaker). The operator pulled the acting captain back into the platform, and the two survivors huddled together on the floor of the platform as the aerial ladder continued to rock back and forth several times. They both observed that the platform doors were sprung outward (the doors are designed to only swing inward into the platform). When the aerial ladder came to rest, it was estimated by the fire fighters on the ground as well as the two survivors in the platform, that the platform was approximately 10 to 15 feet away from the building. Note: The platform doors showed relatively minor damage after the incident. The door edge restraint strip was bent inward at the bottom of both doors indicating a force (applied from within the platform) had pushed the doors past the normal stopping point. The restraint strips are approximately 1 ½ inches wide and marks on the front railing show where the strips contacted against the door frame in the normally-closed position prior to the incident (see Photos 14 through 16).
When examined by NIOSH investigators after the incident, it was possible to move the front railing (containing the door frame) approximately one-half inch without exerting much pressure on the railing. It is possible that when the operator struck the control panel and fell partially over the front railing as he was tossed about inside the bucket, this force moved the door frames on both sides to flex away from the door restraint strip, allowing both doors to be individually forced outward when struck by the two victims in rapid succession.
The fire fighter standing on top of the cab of L-1 jumped to the ground to render assistance when he realized the two victims were falling to the ground. He fractured his left heel when he landed on the asphalt parking lot. The other fire fighters rushed to aid the two victims who had fallen from the platform. They immediately administered first aid to control bleeding and then began cardiopulmonary resuscitation (CPR) on both victims. Medical assistance was summoned via radio and both victims were transported to the local hospital where they were pronounced dead. The fire fighter who fractured his heel assisted with rendering aid to the two victims and was later transported to the local hospital where he was admitted and received surgery to repair his heel.
NIOSH investigators reviewed a PowerPoint presentation of the 8-hour training program that was provided to NIOSH by the manufacturer. This PowerPoint presentation did not mention the need for personnel to use fall protection while working in an elevated platform. NIOSH investigators also reviewed the operators’ manual provided by the apparatus manufacturer and noted several areas where the 302-page manual stated the need for personnel to use protective safety belts. The most obvious was a “Warning” box located in the Aerial Safety section which stated “Do not allow personnel on the end of a moving aerial unless they are secured to the aerial with a personal protective safety belt.”
d “Feather” is a term used to describe operating hydraulic controls by slowly opening or closing the valve in an attempt to control the desired operation by limiting the flow of hydraulic fluid through the valve.
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatalities:
- Unfamiliarity with the controls of a new fire apparatus
- Training in a high risk situation without adequate familiarization with the fire apparatus
- No fall restraint devices in use during training at height
- Design of the lifting eyes (one of which snagged the parapet wall) and platform doors which sprung outward during the incident.
CAUSE OF DEATH
The pathologist reports listed the immediate cause of death for both victims as “blunt force injuries” resulting from an accident.
RECOMMENDATIONS
Recommendation #1: Fire departments should ensure fire fighters are fully familiar with new equipment before training under “high risk scenarios.”
Discussion: Modern fire apparatus are complex equipment. Fire fighters require considerable knowledge, skills and abilities in order to properly and safely operate fire apparatus. NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications, Chapter 5 lists the requisite knowledge and skills necessary to safely operate fire apparatus equipped with fire pumps.5 In this incident, the fire department received delivery of a newly manufactured 2008 model, 95-foot mid-mount aerial platform apparatus. Each of the three duty shifts received a factory-authorized training program of approximately eight (8) hours, including both classroom and practical exercises. The hands-on training included raising the aerial platform into the air with fire fighters in the platform. After completing the factory training, each shift practiced and drilled with the new apparatus as time permitted. Fire fighters interviewed by NIOSH investigators reported taking the apparatus out in front of the station and setting it up a number of times. They also reported taking the apparatus to the local football field, elevating the platform and flowing water on at least one occasion. This was the first platform apparatus utilized by the fire department and was purchased to replace a straight 110′ aerial ladder truck. The electronic-over-hydraulic controls were completely different than other fire apparatus at the department. In general, training should reinforce safe practices until they become automatic. Training on the proper method of operating an aerial platform should be done in low risk settings. In this incident, the fire department initiated additional training following a structure fire so that fire fighters could gain additional experience in setting up and operating the newly-purchased aerial platform apparatus. A number of fire fighters interviewed by NIOSH investigators reported jerky and unsteady movement of the ladder and platform while operating the controls. The use of a spotter stationed on the roof of the dormitory may have aided in guiding the platform operator while the platform approached the building.
Recommendation #2: Fire departments should ensure fall protection is used whenever fire fighters and other personnel are working in elevated aerial platforms.
Discussion: The National Fire Protection Association NFPA 1901 Standard for Automotive Fire Apparatus, 2003 Edition requires the apparatus to be equipped with four (4) ladder belts before the apparatus is placed in service .2 NFPA 1901 details the requirements of the apparatus and equipment only. The use of safety belts is required by the NFPA Safety Standard, NFPA 1500, Chapter 8, Section 8.5.22,6 which states “When members are operating from aerial devices, they shall be secured to the aerial device with a system in compliance with NFPA 1983, Standard on Life Safety Rope and Equipment for Emergency Services.” Specific ladder belt requirements in NFPA 1983 are found in Chapter 6, Section 6.4.3 While other occupations and industries require full body harnesses as fall protection, fire fighters wearing full turnout clothing and SCBA may find the use of full body harnesses impractical. Fire fighters working in elevated aerial platforms should always wear a ladder belt that is attached to the appropriate anchoring point within the platform to protect against inadvertent falls.7 As part of this investigation, the apparatus manufacturer provided NIOSH with a copy of the PowerPoint presentation used in the 8-hour training program that was provided to the fire department. This PowerPoint presentation did not mention the need for personnel to use fall protection while working in an elevated platform. NIOSH investigators also reviewed the operators manual provided by the apparatus manufacturer and noted several areas where the 302-page manual stated the need for personnel to use protective safety belts. The most obvious was a “Warning” box located in the Aerial Safety section which stated “Do not allow personnel on the end of a moving aerial unless they are secured to the aerial with a personal protective safety belt.”
Recommendation #3: Fire departments should follow standard operating procedures (SOPs) for training, including the designation of a safety officer.
Discussion: In this incident, the entire duty shift reported to the college dormitory for hands-on training to familiarize fire fighters with the operation of the new ladder truck. The fire department was in the process of writing a new standard operating procedure (SOP) for the ladder truck but it had not been completed. Hands-on training provided by the manufacturer prior to the incident was conducted without the use of fall protection. Fire fighters interviewed by NIOSH reported that informal practice with the new aerial platform was also conducted without the use of fall protection. A designated safety officer at the training exercise may have positively influenced the use of fall protection during the training exercise.
Recommendation #4: Fire departments should ensure SOPs covering the operation and use of fire apparatus (including aerial platform apparatus) are developed and followed during training exercises as well as in fire suppression activities.
Discussion: In this incident, the fire department was in the process of developing a new SOP to cover the operation and use of the newly-purchased aerial platform apparatus. A copy of the draft SOP was provided to the NIOSH investigators. This apparatus was the first aerial platform apparatus used by the fire department and was purchased to replace a straight aerial ladder apparatus. The fire department was using the manufacturer’s mid-mount apparatus operators manual as the basis for developing the new SOP. At the time of the incident, the new SOP had not been completed. NIOSH investigators reviewed the operators manual provided by the apparatus manufacturer and noted several areas where the 302-page manual stated the need for personnel to use protective safety belts. The most obvious was a “Warning” box located in the Aerial Safety section which stated “Do not allow personnel on the end of a moving aerial unless they are secured to the aerial with a personal protective safety belt.” However, the PowerPoint presentation used in the 8-hour classroom training did not mention the need for personnel to use fall protection while working in an elevated platform.
Recommendation #5: Fire departments and authorities having jurisdiction should provide fall protection belts with all aerial ladder and platform apparatus and ensure that fall protection is used in both training exercises and emergency response events. Fire apparatus manufacturers should include the use of fall protection in both demonstration and training programs.
Discussion: In this incident, the newly purchased fire apparatus was delivered without fall protection included. Fall protection belts from the original ladder truck were available and new fall protection belts for the new platform apparatus were on order but had not been delivered to the fire department at the time of the incident. Fire fighters interviewed by NIOSH investigators reported that fall protection was not used during training provided by the manufacturer. NIOSH investigators reviewed a PowerPoint presentation of the 8-hour training program that was provided to NIOSH by the manufacturer. This PowerPoint presentation did not mention the need for personnel to use fall protection while working in an elevated platform. As noted above, the 302-page operator’s manual did mention the need for personnel to use fall protection.
Since fall protection devices and systems are components of an individual fire fighter’s integrated personal protective equipment ensemble and not a part of the aerial apparatus, fire departments need to ensure that the appropriate fall protection is used at all times. The fire department or authority having jurisdiction should ensure that personnel are never allowed to operate in or on the aerial device without proper fall protection.
Fall protection must be easy and quick to don and doff, effective, but not hinder the movement of the fire fighter using the fall protection. Manufacturers of personal protective equipment should consider these needs when designing and producing effective fall protection systems for fire service use, and apparatus manufacturers should consider these needs when locating fall protection anchors on aerial devices.
Recommendation #6: Fire apparatus manufacturers should ensure that aerial platforms and other aerial devices are designed to reduce or eliminate the potential for snagging on buildings or other elevated surfaces
Discussion: By design, aerial platform devices may be required to be maneuvered in close proximity to buildings and structures of different design and construction materials. By necessity, aerial platforms should be designed to reduce or eliminate the potential to snag or catch on buildings or other structures as the aerial platform is being maneuvered. In this incident, the lifting eyes attached to the waterway underneath the aerial platform snagged on the parapet wall as the platform was being positioned so that fire fighters in the platform could access the dormitory building roof. The aerial platform operator leaned out over the front railing in an attempt to determine why the platform would not move, but could not see the lifting eyes from his location at the control panel. Reducing the potential for snagging the aerial platform on an elevated surface may have resulted in a different outcome in this incident. For example, the lifting eyes under the aerial platform were attached to the water manifold to the water monitor. The lifting eyes could have been located where they did not extend below the water manifold piping. It is noted that the operator’s manual did include a statement in the Aerial Safety section which read “Use the aerial assembly in a cantilevered position only. Do not power the aerial down on windows or roofs. Position the aerial device approximately 6-12″ above a structure, and allow the weight of personnel to deflect the aerial near the structure.” The Aerial Safety section also included a “Warning” box which read “Do not make contact with any structure using the aerial assembly.”
Recommendation #7: Fire apparatus manufacturers should ensure that aerial platform doors or gates are designed to prevent opening in the outward direction.
Discussion: In this incident, the platform doors included retaining strips that were intended to keep the doors from swinging outward past the integral guard rail surrounding the platform (see Photo # 11 and Photo # 12). During this incident, both platform doors were sprung outward past their intended stopping point, resulting in the two victims falling through the openings in the platform guard rail. The retaining strips on both doors were visibly bent after the incident (see Photo # 13). The doors, as designed, met the requirement of NFPA 1901, Chapter 20.7.6.2.2.3, for inward opening, self-closing gates or doors for access to and from the platform. The doors were designed with retaining strips extended from the door latch upward to near the top of the door. There was no retaining strip below the door latch (see Photos 11 through 13 for a visual description of the doors and retaining strips). Wider retaining strips at the top, and/or additional retraining strips below the door latch may have served to keep the doors from moving past their intended stopping point. The platform doors were equipped with simple spring-loaded latches. The use of a different type of door latch, such as one requiring a turning or twisting motion to open the latch may also have prevented the doors from opening inadvertently.
REFERENCES
- Fire Research Corporationexternal icon [2009]. http://www.fireresearch.com/product.php?id=msa400 ManSaverT Aerial Bar. Date accessed: April 2, 2009.
- NFPA [2003]. NFPA 1901: Standard for Automotive Fire Apparatus, 2003 Edition. National Fire Protection Association, Quincy, MA.
- NFPA [2006]. NFPA 1983: Standard on Fire Service Life Safety Rope and System Components, 2006 Edition. National Fire Protection Association. Quincy, MA.
- Weather Undergroundexternal icon [2009]. http://www.wunderground.com/history/airport/KGGG/2009/1/25/DailyHistory.html?req_city=Kilgore&req_state=TX&req_statename=Texas. Date accessed: April 2, 2009.
- NFPA [2009]. NFPA 1002: Standard for Fire Apparatus Driver/Operator Professional Qualifications, 2009 Edition. National Fire Protection Association, Quincy, MA.
- NFPA [2007]. NFPA 1500, Standard on Fire Department Occupational Safety and Health Program, 2007 Edition. National Fire Protection Association, Quincy, MA.
- IFSTA [2000]. Aerial Apparatus Driver/Operator Handbook, First Edition. International Fire Service Training Association. Fire Protection Publications. Oklahoma State University. Stillwater Oklahoma.
INVESTIGATOR INFORMATION
This investigation was conducted by Tim Merinar, Safety Engineer, and Matt Bowyer, General Engineer, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH and William Peters, of Peters Associates, Fire Apparatus Consulting Services, Inc. Mr. Peters is a retired Battalion Chief with over 28 years experience with the Jersey City, New Jersey Fire Department and is active in the National Fire Protection Association (NFPA) consensus standards process. This report was authored by Tim Merinar and William Peters. An expert technical review was conducted by Kevin Roche, Assistant Fire Marshal, Phoenix Fire Department.
DISCLAIMER
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
PHOTOS AND DIAGRAMS
|
|
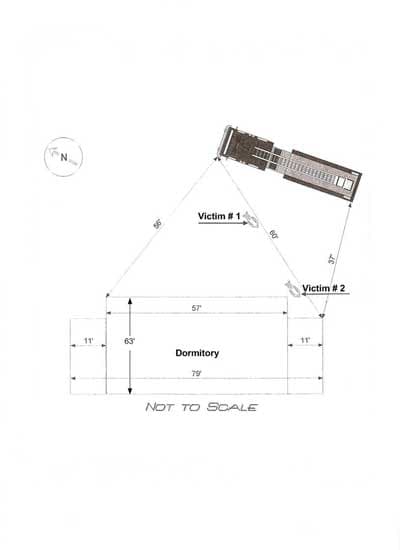
Diagram 1. Simplified layout of incident scene. For reference only. Note that diagram depicts a rear-mount ladder apparatus rather than a mid-mount apparatus as was involved in the incident. |
|
|
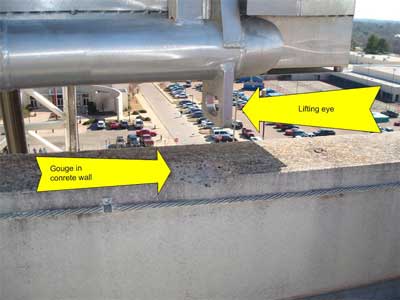
Photo 5. Photo shows location where the lifting eye caught on the top of the parapet wall. The gouge in the concrete wall resulted when the inner surface broke as pressure was applied to the lifting jack to raise the platform off the parapet wall. NIOSH photo. |

|
|
Photo 6. Note damage to inner bottom edge of lifting eye matches up with top edge of parapet wall. This demonstrates the lifting eye was caught on the inner edge of the wall. Police investigators removed samples of aluminum shavings from the site immediately after the incident. |

|
|
Photo 7. Close-up of scratches and burrs on the inner bottom |

|

|
|
Photo 9. Photo shows chunks of concrete on top of parapet wall beside the gouge where the lifting eye was caught. The concrete chunks were found on the roof by police detectives immediately after the incident. |

|

|
|
Photo 11. Red arrow indicates location of lifting eye under platform that caught on inside edge of parapet wall. Pressure was applied to the lifting pistons in an attempt to raise the platform off the parapet wall. When the concrete surface gave way, the ladder sprung away from the building, then rocked back and forth several times. The yellow arrows depict the rocking motion that propelled the victims out of the platform. |
|
|
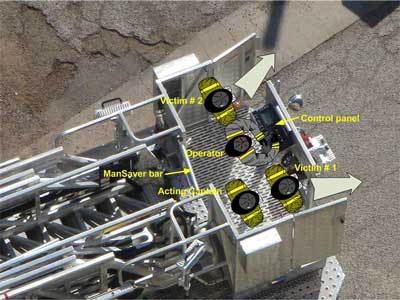
Diagram 2. Approximate location of crew in platform at time of incident. Note that this diagram shows the platform nested at rear of the apparatus and not elevated. Also note that both platform doors are sprung outward past their intended stopping points. Both doors are designed to swing inward (into the platform) only. |

|
|
Photo 12. Note how the ManSaver™ Aerial Bar mounting base is bent back toward ladder (indicated by yellow arrow) indicating one or more of the fire fighters struck the bar with force as the crew was tossed about the platform. Red arrow indicates separation between bar mounting base and support bracket where bar is mounted. |

|
|
Photo 13. Note intercom speaker in center of photo is bent. |

|
|
Photo 14. Left platform door. Note door latch and retaining strip designed to keep the door from swinging outward and how door is sprung outward. The door is designed to swing into the platform and when closed, the door is designed to be an integral part of the guard rail system required by NFPA 1901, Chapter 20.7.6.1.2. |

|
|
Photo 15. Right platform door. Note the retaining strip to keep the door from swinging outward is located above the door latch only. There is no retaining strip below the door latch. |

|
|
Photo 16. Photo shows the retaining strip on the right platform door is bent inward. One possible cause would be a force applied to the door from within the platform when one of the fire fighters came in contact with the door, causing the door retaining strip to |
|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit the program website at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 03/24/2014.