
Volunteer Deputy Fire Chief Dies When Struck by Motorized Water Monitor that "Launched" Off Aerial Ladder Truck - Pennsylvania
Revised February 19th, 2009 to add information on a new waterway launch.
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2008-12 Date Released: February 6, 2009
Also see a NIOSH Safety Advisory concerning this hazard at
https://www.cdc.gov/niosh/fire/SafetyAdvisory06242008.html
SUMMARY
On April 8, 2008, a 24-year old male volunteer Deputy Fire Chief (the victim, serving as the Incident Commander), was killed when struck by a motorized water monitor and 30 feet of aluminum pipe that was “launched” from an elevated aerial ladder at an industrial fire in Pennsylvania. The ladder was normally transported in the rescue mode with the monitor pinned to the second section of ladder so that the waterway would not be in the way if the ladder was set up for rescue operations. At the incident scene, when the waterway was pressurized, the monitor and its support bracket, along with the last 30-foot section of pipe was launched off the aerial ladder by the force of the water in the pipe. The monitor flew approximately 75 feet and fell, striking the Incident Commander on the head, killing him instantly. Another fire fighter standing next to the victim was knocked down but not seriously injured.
 |
|
Photo 1. Aerial ladder being raised into position for master stream operation. (Photo courtesy of Matt Skrekla.)
|
After the incident, the waterway anchor pin was found on the ground, in front of the truck’s cab. The waterway did not include secondary mechanical stops to prevent the separation of the water monitor in the event the anchoring pin was not properly seated.
Key contributing factors identified in this investigation include the original equipment design (lack of secondary mechanical stops to prevent separation in the event the anchoring pin was not properly installed), inadequate staffing, the involvement of multiple individuals in setting up and operating the apparatus, and inexperience in setting up the ladder.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
- ensure that Standard Operating Procedures (SOPs) and/or Guidelines (SOGs) for setting up multi-position waterways include steps to properly position the waterway and to inspect and verify that the locking mechanism (anchoring pin(s), lever, clamps, etc.) are properly installed and functioning as designed before pressurizing the waterway
- provide training and practice for fire fighters on the correct method of securing waterways and verifying they are secured (per manufacturer’s recommendations)
- ensure critical tasks are properly supervised
- contact aerial ladder manufacturers to retrofit existing aerial ladder trucks with secondary stops or other engineering controls to prevent waterway launches in the event the waterway is improperly anchored
- ensure that adequate numbers of staff are available to effectively respond to emergency incidents
Fire apparatus manufacturers should:
- provide aerial ladder trucks with secondary stops or other mechanical means of preventing inadvertent waterway separation or launch
Standards setting organizations should:
- establish standards that include engineering safeguards to prevent inadvertent waterway separation
Business owners and property managers should:
- address fire hazards and enforce fire prevention measures
Additionally, municipalities, business owners, and authorities having jurisdiction should:
- ensure fire hydrants are inspected and tested on a regular basis
INTRODUCTION
On April 8, 2008, a 24-year old volunteer Deputy Fire Chief (the victim, acting as the Incident Commander), was killed when struck by a motorized water monitor and 30 feet of aluminum pipe that was launched from an elevated aerial ladder at an industrial fire in Pennsylvania (see Photo 1). On April 9, 2008, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR) of the fatality. The fire apparatus was impounded following the April 8, 2008 incident and secured in a private restricted-access storage facility. The NIOSH Fire Fighter Fatality Investigation and Prevention Program contracted with a fire service consultant knowledgeable in all aspects of fire apparatus operations, performance and equipment requirements to assist with the investigation. On April 21, 2008 a NIOSH safety engineer and the consultant, along with a criminal investigator with the Pennsylvania State Police, the district attorney, and representatives from two volunteer fire departments involved in the incident inspected the fire apparatus and checked the function of the aerial ladder and water delivery system. Two representatives of the local municipal fire department were also present (one was the chief of the department and one was present to operate the fire apparatus). Following the inspection of the fire apparatus, the NIOSH investigator and the consultant visited and photographed the incident scene and met with and interviewed the manufacturing plant representatives who were involved in the fire suppression activities. The NIOSH investigator and consultant also inspected an apparatus from the same manufacturer, similar in design, but 4 years newer than the incident apparatus. On April 23, 2008 the NIOSH safety engineer and consultant conducted interviews with members of the victim’s fire department who were involved in the incident. On April 24, 2008, the NIOSH investigators met with representatives of the manufacturer of the fire apparatus and again inspected the apparatus at the secure storage facility. The fire apparatus was photographed and measured. Specifications for the apparatus were obtained from the fire department and also from the manufacturer. Additional photographs were obtained from a number of sources including the state police, the fire department involved in the incident, and from fire fighters from mutual aid departments that responded to the incident. NIOSH investigators also reviewed training records, standard operating procedures, dispatch tapes, and the coroner’s report.
After collecting the preliminary information, NIOSH developed a Safety Advisory to notify the fire service of immediate actions to take to reduce the risk of fire fighters being struck by unsecured waterways or parts of the waterways. The complete Safety Advisory can be viewed at the NIOSH website https://www.cdc.gov/niosh/fire/SafetyAdvisory06242008.html.
Fire Department
The volunteer fire department involved in this incident serves a population of approximately 5,000 permanent residents in an area of 2.5 square miles, consisting mostly of residential and commercial structures. A large heavy manufacturing facility with a daytime workforce of 5,500 employees doubled the daytime population of the immediate area. The fire department had 15 uniformed volunteer fire fighters at the time of the incident. The fire department operated 5 fire apparatus that responded from a centrally located fire hall. The fire department operated a progressive on-going training program with weekly training sessions that covered all aspects of emergency response, fire fighting, and rescue operations. The volunteer staff included 10 certified Emergency Medical Technicians (EMTs) and 4 fire police.
Training and Experience
The crew directly involved in this incident included the victim (Deputy Fire Chief, serving as the Incident Commander), a driver / operator, a fire fighter/EMT-Captain and a probationary fire fighter. The victim was a 24-year old male who had 6 years of fire fighting experience at this fire department and had been around the fire department since he was 14. He was serving as the Deputy Fire Chief and training officer at the time of the incident. The victim had served as an Air Force medic and was honorably discharged in August 2007. The victim had recently been hired as a full time career fire fighter for a local municipal fire department. The victim had received extensive fire service training including essentials of fire fighting, truck company operations, engine company operations, incident command, fire fighter survival, confined space rescue, forcible entry, Haz Mat operations, rapid intervention concepts, fire rescue, building construction and emergency vehicle operations. He was a state certified Emergency Medical Technician.
The driver / operator had over 20 years experience with the department and was the regular driver / operator of the aerial ladder truck involved in this incident. The fire fighter had over 5 ½ years of experience with the department and held the rank of EMT Captain. The probationary fire fighter had 3 ½ years of total fire fighting experience and had been with this department for approximately 3 months at the time of the incident. Both fire fighters stated during the NIOSH interviews that they had been trained by the victim on how to set-up the aerial ladder.
The fire department was in the process of upgrading its training procedures and requirements. The victim (training officer) and the assistant training officer were in the process of requiring all fire fighters to obtain certificates for the equipment they were trained to operate, as directed by the fire chief. Prior to this, fire fighters received hands-on training and were considered “trained” and “qualified.” Under the new process, fire fighters had to possess training certificates in order to be qualified to work on specific equipment.
Equipment and Personnel
The fire originated in a section of the county serviced by a number of volunteer fire departments operating under a mutual aid agreement with a neighboring municipal fire department. The victim served a volunteer department that was located in a neighboring jurisdiction to the location of the fire.
The following timeline lists key apparatus involved in the incident in the order of dispatch, arrival (time approximate) and key events.
1554 hours
- Initial Alarm
1555 hours
- Plant employee (also a volunteer fire fighter for a neighboring department) radios to report condition of fire and request second alarm
1557 hours
- Mutual aid department 1 – Ladder 289 [Driver / operator, Deputy Chief (Victim), fire fighter, probationary fire fighter] leaves station
1603 hours
- Mutual aid department 1 – Ladder 289 on scene
1605 hours
- Medic 1 (2 Emergency Medical Services (EMS) personnel) – on scene Rescue 288 (fire fighter and 2 probationary fire fighters) – on scene Deputy Chief of the department having jurisdiction (Deputy Chief # 2) – on scene Mutual aid department 1 Chief – on scene
1615 hours
- Fire fighter down – radio request for air ambulance helicopter
Fire Apparatus Inspection and Evaluation
The fire apparatus involved in this incident is a 1994 custom fire apparatus with a rear mounted, 3-section, 75 ft steel aerial ladder with a 1,000 GPM waterway and 1,750 GPM, single-stage fire pump. The fire apparatus or ladder truck incorporates an aerial device consisting of a 75-foot, 3-section, telescoping ladder constructed of welded steel components. The ladder is mounted to a turntable at the rear of the apparatus that allows it to rotate 360 degrees. All movements of the aerial ladder are operated hydraulically. The aerial device has a 3-section, telescoping aluminum waterway mounted under the ladder. Water is fed to the waterway by a series of swivel connections at and through the turntable. Water can be introduced into the waterway system either directly from a 4” intake at the rear of the apparatus (from a secondary source such as another apparatus) or from a discharge valve connected to the on-board fire pump supplied by hydrant water or other primary sources. The waterway under the turntable contains a pneumatically operated on/off valve that controls the water flow. This valve is controlled by a protected on/off switch on the rear of the apparatus. Directly above the valve is a waterway relief valve. This valve relieves any excess pressure to protect the waterway seals when the system is charged. In November 2007, the knuckle under the turntable failed and was replaced. This involved removing the aerial ladder, the waterway, and the turntable. Certificates were reviewed indicating the ladder truck had been re-certified to the requirements of NFPA 1911.1
The fire pump is a single-stage centrifugal fire pump rated at 1,750 GPM. The pump produces 45 psi at idle. Pump pressure is controlled by a hand throttle at the driver-side control panel that adjusts the speed of the truck’s diesel engine and a combination pressure-relief/dump valve. When the pump operator sets the desired pressure on the panel controller, the unit attempts to maintain the pressure first by re-circulating water from the discharge side of the pump back to the suction side. If the pressure still exceeds the setting, a dump valve opens relieving pressure to the atmosphere. Water can be fed to the pump from either side of the truck. Note: When interviewed by the NIOSH investigators, the driver / operator stated the preferred option was to connect the supply line to the right or officer’s side of the apparatus (opposite the main control panel). The 6” pump intake on the officer’s side pump panel has a piston intake valve, with a built-in relief valve. The valve opens by turning a hand-wheel crank to introduce water into the fire pump. The relief valve is on the incoming side of the main valve and has a plunger that opens against spring pressure to relieve excess incoming water to the atmosphere. The valve setting at the time of the incident could not be specifically determined but it was between 100 and 150 psi.
The fire pump includes an electronically-controlled valve plumbed into the waterway at the rear of the apparatus under the turntable. The operation of this valve was tested with an average time of 7.5 seconds to move from fully closed to fully open. This valve can be “throttled” between open and closed, to control the amount of flow to the waterway. The rear panel of the truck includes an aerial waterway flow meter and pressure gauge. Another aerial flow meter is located on the main pump panel (driver’s side).
The discharge end of the waterway includes a “slider” assembly that holds an electronically controlled motor-driven monitor and electronically controlled 150-1,250 GPM automatic nozzle. The motorized monitor allows the nozzle stream to be directed side-to-side and up-and-down. The nozzle is of the automatic type which has a variable orifice controlled by spring pressure that maintains a 100 psi nozzle pressure over the rated flow of the nozzle. When the pressure is low, the orifice is nearly closed and as the pressure increases it opens up. This maintains a workable fire stream under all conditions. The nozzle also has a motor-driven control to change the pattern from straight stream to a wider spray pattern.
 |
|
Photo 2. Waterway that “launched” during incident. Arrows depict Nylatron® pads that are greased to aid movement as the ladder extends and retracts. (NIOSH photo.) |
A spring loaded cable reel is mounted to the right side of the aerial bed section (first section of ladder off the turntable) with a captive four-roller guide mounted to the tip of the second section. An electrical cable is deployed from the reel, through the guide to the control box on the right side of the monitor assembly to provide remote control of the monitor position and the nozzle spray pattern.
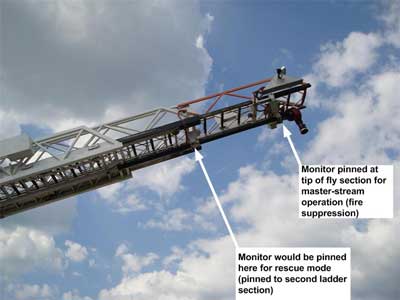
The slider assembly is a heavy steel structure built by the aerial manufacturer to support the end of the 3rd section of the waterway, the monitor assembly and the nozzle. It is suspended under the ladder by four (4) “C” shaped hangers that capture the lower rail of the fly section of the ladder. Nylatron® pads are installed on the hangers to reduce friction and to allow the ladder to slide through the hangers (see Photo # 2). At the rear of the slider is located a flat pin receiver plate with two reinforced holes in it. When the ladder is bedded, these holes line up with corresponding holes in the fly section and the second section of the aerial ladder. If the fire department wants to keep the waterway at the second ladder section, to allow the fly section to remain clear for rescue purposes (reference Photos # 3 and # 4), a heavy steel pin with detent ball is inserted in the rear or lower hole (reference Photo # 4). Note: The “lower hole” refers to the hole in the middle ladder section. If pinned at the tip, the waterway is pinned to the top or upper ladder section. If pinned for rescue mode, the waterway is pinned to the middle or second ladder section. As the ladder is extended the fly section passes through the four hangers leaving the monitor at the second section. This allows the tip of the ladder to be positioned for rescue operations at windows, rooftops, ledges, etc. without interference from the monitor. If the operation is to supply an aerial master stream from the tip of the fly section (Reference Photo # 3), the fire fighter would remove the pin from the lower hole and insert it in the upper one. The pin would capture the fly section and the slider assembly and the aerial would move as one unit. The pin MUST be inserted in one hole or the other. The fire department routinely responded with it in the lower position (set-up for immediate rescue operation).
NFPA Standards Compliance
The NFPA Standard that governed the construction of aerial apparatus in 1994, the year the fire apparatus was built, was NFPA 1904, Standard for Aerial Ladder and Elevating Platform Apparatus, 1991 Edition.2 In 1996, NFPA 1904 was combined with NFPA 1901. The NFPA 1904 standard was its own separate standard for only one revision cycle and no longer exists.
An examination of the apparatus indicated that the components of the aerial water delivery system were in compliance with the NFPA 1904 Standard (1994 Edition). The waterway requirements were:
- 1,000 GPM monitor
- 1,000 GPM nozzle
- A relief valve in the waterway
- A flow meter
- A 1-1/2” drain valve
The pump section of the same standard required that any discharge outlet valve that is 3” or larger have an operating mechanism that will not permit changing the position of the flow regulating element from fully-closed to fully-open, or vice versa, in less than 3 seconds. These items were all compliant on the subject apparatus.
Conditions Found on Inspection
After the incident, the apparatus was taken to an impound facility along with the waterway which was transported and stored on a trailer. It was secured and access restricted to only personnel authorized by the District Attorney.
An inspection of the apparatus components pertaining to the incident was as follows:
- A piston intake valve, with pressure relief, was located on the right side steamer connection. The valve was in the closed position. Note: The valve had been opened during the incident. It is unknown when the valve was closed.
- The pump pressure control (relief valve) was set between 250 and 300 psi.
- The electrically controlled waterway supply valve on the pump panel was closed (closed by the operator during the incident).
- The pneumatic waterway supply valve at the rear of the apparatus was open.
- Waterway drain valve was closed.
- The waterway (stored on a flatbed trailer) displayed the following characteristics:
- The nozzle at the tip was aimed to the right of center and up.
- The nozzle at the tip was broken. The orifice plunger was in pieces and held as evidence by the State Police.
- The monitor housing was cracked.
- The waterway pipe was curved to the right and up when the unit was placed in a normal position. It appears that this may have been caused when the monitor control cable reached the end of its travel and pulled the pipe up and to the right.
- The waterway pin was secured by the State Police and showed no evidence of damage or deformation (other than the pull ring which several witnesses stated was always in that condition).
- The holes in the slider assembly and in the two ladder sections showed no evidence of damage or deformation.
Structure
The structure involved in this incident was a plastics manufacturing facility that operated out of a single 500,000 square foot building that housed production, warehouse, and office facilities. The facility was involved with injection molding of plastics, structural foams, and also produced a proprietary line of plastic pallets.
The fire started outside the structure near the loading dock in an area containing wooden and plastic pallets (Reference Photos # 7 through # 9). State fire marshal investigators determined the fire was unintentional in nature and caused by employees smoking on the loading dock. The company had a no-smoking policy in effect at the time of the incident. The fire rapidly grew on the loading dock consuming the pallets stored there. The fire extended up the exterior wall with minimal extension into the interior. The structure was equipped with an automatic sprinkler system which activated on two levels.
Weather
At the time of the incident, the weather conditions were clear with an approximate temperature of 59 degrees Fahrenheit, 58 percent relative humidity, and north / northeast winds at approximately 10 miles per hour.
INVESTIGATION
On April 8, 2008 at approximately 1553 hours, an employee at the plastics manufacturing facility called 911 and reported a fire on the loading dock that was threatening the building. Two of the plant employees were volunteer fire fighters at neighboring fire departments, one being the Chief of his department. One of the employees (the Deputy Chief of a neighboring department) had his turnout gear and personal protective equipment including a self-contained breathing apparatus (SCBA) in his truck; he donned his gear to assist with the fire suppression activities. The Deputy Chief of the neighboring department assumed incident command (IC) until the fire department arrived.
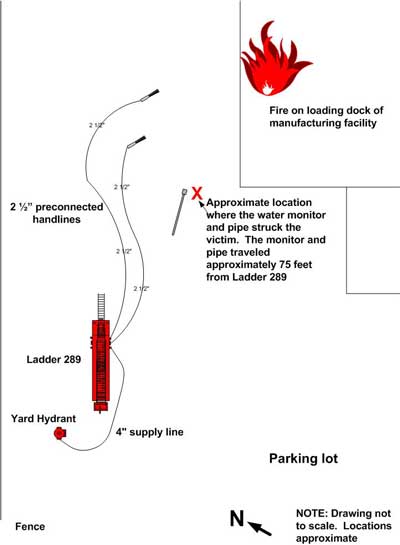
The volunteer fire department involved in this incident regularly had volunteer fire fighters at the station during daytime hours so they became the first responding crew in-service following the dispatch. This fire department was one of four local mutual aid fire departments dispatched at 1554 to the manufacturing facility. Fire fighters arrived at the station, quickly got their gear ready and were enroute at 1557 hours on Ladder Truck 289 (L-289). The crew consisted of a driver / operator, the Deputy Fire Chief (victim – riding in the officer’s seat) and two fire fighters. L-289 was the first apparatus to arrive on scene at 1603 hours, even though the manufacturing facility was outside their jurisdiction. L-289 initially stopped at the main entrance to the plant to connect to a hydrant along the roadway, but was directed by plant employees to enter the parking lot and connect to a yard hydrant on the north side of the structure (reference Diagram 1).
Once L-289 pulled past the yard hydrant and stopped, the Deputy Fire Chief (victim) asked the fire fighter if she could make the connection to the hydrant, and he asked the probationary fire fighter if he could set-up the aerial for master-stream operation. Both fire fighters replied “yes,” and moved to complete their respective tasks. The Deputy Fire Chief assumed Incident Command.
The two plant employees who were volunteer fire fighters approached L-289 and transferred incident command to the Deputy Fire Chief who just arrived on L-289. They asked the Deputy Fire Chief if he wanted them to pull a handline. The Deputy Fire Chief said “yes,” and a 2 ½” preconnected handline was stretched to the loading dock. The employee with turnout gear took the nozzle. The Deputy Fire Chief directed the L-289 driver / operator to charge the handline. The handline was charged with tank water. The probationary fire fighter went up to the monitor to switch the anchoring pin for master stream operation. After that, the Deputy Fire Chief directed the probationary fire fighter to help on the 2 ½” handline so the probationary fire fighter donned his SCBA and followed the handline to the nozzle to assist the plant employee.
Rescue 288 arrived on scene with a crew consisting of a fire fighter and two probationary fire fighters. The Deputy Chief directed the fire fighter to don his personal protective equipment and assist on the handline. The two probationary fire fighters were directed to stand by the ambulance and assist with EMS activities if needed.
The L-289 fire fighter stretched a 4” supply line to the hydrant and helped the driver / operator chock the wheels and set the outriggers so that the aerial ladder could be elevated. She attempted to connect the supply line to the hydrant, but had difficulty in removing the hydrant cap. The driver /operator and the fire fighter both tried hitting the hydrant wrench with a rubber mallet and also stood on the wrench handle but were unable to loosen the hydrant cap. By this time, the tank water was down to half-full (two lights showing on the indicator panel). The L-289 driver /operator radioed the Deputy Fire Chief (IC) that the hydrant cap could not be removed and requested to have the next due apparatus lay a supply line from the hydrant along the road near the plant entrance. He removed the 4” supply line from the pump intake on L-289 so that the next supply line could be connected and then went back to work on opening the yard hydrant.
The Fire Chief (chief of the department) arrived on-scene a few minutes after L-289 and Rescue 288. He asked the Deputy Fire Chief what was needed to assist in the fire suppression efforts. The Deputy Fire Chief asked the Chief to operate the aerial ladder for master stream operations (reference Photo 5). The L-289 driver /operator asked the Chief to check and make sure the 4” supply line was re-connected on the officer’s side of the truck. After verifying the connection was made, the hydrant was opened and the driver / operator adjusted the intake pressure and began filling the tank as the tank water level was down to one-quarter by this time. The Chief then climbed up on the rear of L-289 to operate the aerial ladder. He noticed that the turntable railing safety chain on the driver side was down. Note: The L-289 probationary fire fighter had already gone to the monitor to switch the anchoring pin and left the safety chain down. The Chief raised the aerial ladder to 60 degrees elevation and extended the tip to 67 feet. The Chief, the driver /operator, and the L-289 fire fighter all observed that the monitor remained at the second section. The driver / operator and the L-289 fire fighter questioned why the monitor was not at the tip of the fly section. The Chief stated he felt they were close enough to the building to hit the fire with the monitor in the second position and he did not want to take the time to lower the ladder and reposition the monitor. Note: The Chief was unaware of the actions to move the anchoring pin and thought the monitor was still pinned to the second section. L-289 was in high-idle “lock-out” mode (pump mode) which caused the hydraulic system that raises and positions the aerial ladder to operate slowly.
 |
|
Photo 5. Photo taken just seconds before fatal launch. Note the water monitor is still in the rescue position. |
The Chief radioed the Deputy Chief (Incident Commander – the victim) and asked him if he was ready for water and he (the victim) replied to wait. The Chief adjusted the monitor nozzle position to the right and up in anticipation of an attack on the fire. Note: At this point, the victim was standing between L-289 and the loading dock approximately 75 feet in front of L-289 and was talking face-to-face with the Deputy Chief of the department who had jurisdiction over the manufacturing plant location (Deputy Chief 2). They were discussing the fire conditions and the victim was in the process of transferring Incident Command to Deputy Chief 2. The victim was positioned with his back to the building and L-289 off his left shoulder. Deputy Chief 2 was positioned facing the victim (facing the building) with L-289 off his right shoulder.
The Deputy Chief (the victim) radioed to charge the master stream. Witnesses reported hearing the “hiss” of air escaping through the nozzle and the sound of water rising through the waterway pipe as the system was pressurized. When the waterway was pressurized, the monitor and its support bracket, along with the last 30-foot section of pipe, was launched from the aerial ladder by the force of the water in the pipe. The monitor and waterway (with an estimated weight of over 200 pounds) flew approximately 75 feet and fell, striking the victim on the head. The Deputy Chief of the second department (Deputy Chief 2) was knocked down but was not seriously injured (reference Photo # 6). Fire fighters and EMS personnel on-scene rushed to aid the victim. His Chief radioed dispatch and requested air ambulance services for a fire fighter down at 1615 hours. The air ambulance was on the scene at 1629 hours but was not used. The victim was transported via ground ambulance to a local trauma emergency room. The air ambulance crew accompanied the victim in the ground ambulance. The victim was pronounced dead at a local hospital at 1656 hours.
After the incident, the anchor pin was found on the ground, in front of the truck’s cab. When the water column collided with the restriction in the monitor and partially closed automatic nozzle, the waterway pipe became a large hydraulic piston. With no secondary stops to contain the unsecured slider, it was propelled up the ladder rails at an estimated 30 mph towards the tip.
 |
|
Photo 6. Waterway is in foreground near the location where it struck the victim. Photo shows distance the waterway traveled after it was “launched.” Note ladder truck L-289 at top right. (Photo courtesy of Matt Skrekla.) |
CONTRIBUTING FACTORS
Since the pin intended to anchor the monitor assembly to the ladder was found on the ground in front of the truck after the incident, the NIOSH investigators concluded that it had not been properly installed.
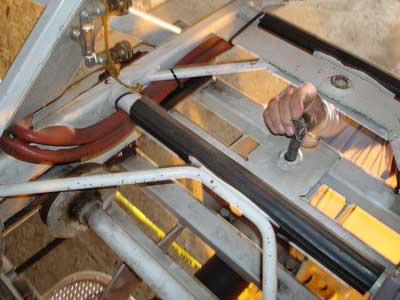
Several fire fighters interviewed by NIOSH indicated that the pin was generally difficult to remove and replace in the holes due to the misalignment of the moving components. Some told of hitting the pin with the rubber mallet to seat it, and others said that they were trained to take the “lady finger” pry bar up on the aerial. The flat end was used to pry the pin out of one hole and the pointed end of the bar was inserted into the other hole to align the ladder and slider holes, allowing the pin to be inserted through them. Alignment issues could not be verified since the water monitor / slider assembly was no longer attached to the aerial ladder. The pin fit easily into the holes in the slider assembly as well as the holes located on the ladder. The holes in the slider assembly and in the two ladder sections showed no evidence of damage or deformation. The pin did not contain any deep scratches or gouge marks, although the retaining ring on top of the pin was distorted. The probationary fire fighter told NIOSH investigators that the pin came out and went in without a problem.
When this truck was built, most manufacturers secured their pinable waterways by the same method with a single pin. Some have since gone to a lever type device that secures the slider to either the fly or the second section. Although this appears to be a safer method of securing the device, it is not fail-safe and there are many pin-style units in use in the field today.
Considering that the single pin design could easily result in human error when setting up the waterway, the NIOSH investigator and consultant questioned why there were no stops at the end of the fly section to prevent the slider from coming off. Three aerial ladder apparatus manufacturers that were contacted indicated that they felt that the waterway traveling at high speed up the aerial, striking a rigid stop, might cause serious damage to the aerial device, possibly leading to a failure of the ladder, or causing a fire fighter standing on the ladder to be knocked or thrown off. Two manufacturers indicated that they add stop blocks, but the result of hitting them with the slider under pressure was unknown.
The following factors could have contributed to the fatal incident:
- The original equipment design (lack of secondary mechanical stops to prevent separation in the event the anchoring pin was not properly installed).
- The delay in responding to the incident, the knowledge that they were responding to a verified fire, and the delay getting water to the apparatus due to the frozen hydrant cap, could have added to the stress of the members operating around the apparatus.
- Five different individuals took part in setting up and operating the apparatus for master stream operation. The critical task of setting up the waterway for master stream operation (which included pinning the waterway) was assigned to a probationary fire fighter with little experience at the task and the task was performed unsupervised. When the aerial ladder operator arrived on the scene, he was unaware that anyone had touched the pin and assumed that the monitor was secured in the travel mode at the second section.
- Inadequate staffing contributed to the need for multiple fire fighters to be involved in setting up the aerial ladder.
- The slow motion of the aerial ladder due to the high-idle pump interlock may have discouraged the operator from lowering the aerial to the bedded position to change the position of the pin.
- The yard hydrant delivered water at an unusually high pressure, 150 psi, which in addition to the 45 psi developed initially by the pump at idle, meant that an estimated pressure of 150 to 195 psi was delivered to the waterway when the valve was opened (some pressure was diverted to refill the apparatus’ water tank).
History of Waterway Incidents
During this investigation, NIOSH became aware of at least 10 similar incidents involving waterways.
Date Location Incident Description
02 / 2009 Indiana Waterway launched 40 ft into parking lot – no injuries
05 / 2008 Virginia Waterway launched 80 ft into woods during drill – no injuries
05 / 2008 Minnesota Waterway charged, broke thru stops and launched – no injuries
12 / 2007 California 4th alarm fire – waterway launched off tip of ladder – no injuries
Unknown New Jersey Waterway launched – no injuries
Unknown Ontario Waterway unlatched improperly – damage to aerial ladder
Unknown Texas Waterway unlatched improperly – damage to aerial ladder
Unknown Texas Waterway unlatched improperly – damage to aerial ladder
Unknown Michigan Operating at fire – waterway launched into fire building – no injuries
Unknown New Jersey Operating at fire – waterway launched into stops – damaging ladder
Unknown Missouri Waterway moved while in operation – fire fighter injured hand
Apparatus from at least four different manufacturers were involved in these incidents.
CAUSE OF DEATH
The coroner’s report listed the immediate cause of death as “blunt force trauma to the head with multiple injuries due to (as a consequence of) a firefighting accident.”
RECOMMENDATIONS
Recommendation #1: Fire departments should ensure that Standard Operating Procedures (SOPs) and/or Guidelines (SOGs) for setting up multi-position waterways include steps to properly position the waterway and to inspect and verify that the locking mechanism (anchoring pin(s), lever, clamps, etc.) are properly installed and functioning as designed before pressurizing the waterway.
Discussion: Standard Operating Procedures (SOPs) and Standard Operating Guidelines (SOGs) provide accountability and control. SOPs and SOGs are general plans that identify who does what, when, and how.3 SOPs and SOGs are written documents that provide a basis for ensuring that tasks are completed in a consistent manner time after time. Operational procedures that are standardized, clearly written and mandated to each department member establish accountability and increase command and control effectiveness. When all fire fighters follow departmental SOPs, confusion is reduced. Fire fighters will understand their duties and require a minimum of direction. SOPs also help prevent duplication of effort and uncoordinated operations because all positions are assigned and covered.3 In this incident, the fire department had an SOP for Ladder Truck Operations but the SOP did not describe the process for moving the anchoring pin to secure the monitor or any type of inspection / verification to ensure proper set-up.
Recommendation #2: Fire departments should provide training and practice for fire fighters on the correct method of securing waterways and verifying they are secured (per manufacturer’s recommendations).
Discussion: The National Fire Protection Association (NFPA) 1500 Standard on Fire Department Occupational Safety and Health Program, 2007 Edition requires that all personnel who may engage in structural fire fighting be adequately trained to do so.4 NFPA 1002 Standard on Fire Apparatus Driver / Operator Training specifies minimum training requirements for fire apparatus driver / operators.5 For example, NFPA 1002 states the requirements of Fire Fighter 1 as specified in NFPA 1001 and job performance requirements defined in Sections 6.1 and 6.2 (of NFPA 1002) shall be met prior to qualifying as an aerial apparatus driver / operator. NFPA 1002 focuses on requisite knowledge and skills recommended for various driving tasks with less discussion on operation of the aerial device. Section 4.3.7 specifies knowledge of the manufacturer’s specifications and operating procedures, and policies and procedures of the authority having jurisdiction as a requisite for operating all fixed systems and equipment on the vehicle not specifically addressed elsewhere in NFPA 1002, so that each system or piece of equipment is operated in accordance with the applicable instructions and policies. This section would apply to the process involving inspecting, moving the anchoring pin (if necessary) and verifying the proper set-up of the moveable waterway.
In general, training should reinforce safe practices until they become automatic. Training on the proper method of securing a waterway needs to include a step to inspect and verify the proper set-up before the aerial ladder is put into operation. This training should reinforce the manufacturer’s recommended set-up procedures. In this incident, five different fire fighters were involved in the set-up and operation of the ladder truck and two were directly involved in setting up the aerial ladder. The critical task of setting up the aerial ladder for master stream operation (moving the anchoring pin from the second fly (rescue mode position) to the tip) was assigned to a probationary fire fighter with limited experience and training in performing this task. This required that the anchoring pin be moved from the rear position to the forward position. Additionally, there was no verification that the aerial ladder was properly set up for master stream operation before the waterway was pressurized.
Recommendation #3: Fire departments should ensure that critical tasks are properly supervised.
Discussion: Fireground tasks can vary from being simple and routine to very complex. Many fireground tasks are critical to a successful outcome and successful completion of these critical tasks may depend on a combination of proper training and supervision. Supervision of fireground tasks should be based on the knowledge, skills, and abilities of the fire fighter assigned to each task. Fire fighters with demonstrated training and experience will require less supervision than those fire fighters having less training and experience. In this incident, the critical task of setting up the aerial ladder for master stream operation (involving moving the water monitor anchoring pin from the rear or lower hole to the forward (upper) hole on the aerial ladder top fly section) was assigned to a fire fighter with little experience and training in performing this task. The task was un-supervised, possibly due to limited staffing and the company officer acting as the initial Incident Commander.
Recommendation #4: Fire departments should contact aerial manufacturers to retrofit existing aerial ladder trucks with secondary stops or other engineering controls to prevent waterway launches in the event the waterway is improperly anchored.
Discussion: Following this incident, the manufacturer of the fire apparatus involved sent a letter to all customers offering a free retrofit program to add secondary mechanical stops on all aerial ladders manufactured prior to 2004.6 NIOSH recommends that all fire departments utilizing aerial ladders with moveable waterways contact the manufacturer(s) of their aerial ladders concerning the installation of secondary mechanical stops or other engineering controls to minimize or prevent the possibility of a waterway launch.
Recommendation # 5: Fire departments should ensure that adequate numbers of staff are available to effectively respond to emergency incidents
Discussion: NFPA 1720 Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Volunteer Fire Departments (2004 Edition) contains recommended guidelines for minimum staffing of volunteer fire departments.7 Chapter 4.1 states that fire suppression operations shall be organized to ensure that the fire department’s fire suppression capability includes sufficient personnel, equipment, and other resources to deploy fire suppression resources efficiently, effectively, and safely. In this incident, limited personnel were available to respond to the structure fire due to the time of day. The volunteer fire department responded with two units that included four fully qualified fire fighters and three probationary fire fighters. Additional staffing may have allowed fully qualified fire fighters to perform critical tasks such as setting up and operating the aerial ladder and allowed for closer supervision of less experienced fire fighters.
Recommendation #6: Fire apparatus manufacturers should provide aerial ladder trucks with secondary stops or other mechanical means of preventing waterway separation or launch.
Discussion: As part of this investigation, a number of fire apparatus manufacturers were contacted about the use of mechanical stops at the end of the fly section to prevent the slider from coming off. Three aerial manufacturers indicated that they felt that the waterway traveling at high speed up the ladder, then striking a rigid stop, might cause serious damage to the aerial device, possibly leading to a failure of the ladder, or causing a fire fighter standing on the ladder to be knocked or thrown off. Two manufacturers indicated that they do add stop blocks but the result of hitting them with the slider under pressure is unknown. The presence of mechanical stops on aerial ladders may prevent waterway separation or launching.
Recommendation # 7: Standard setting organizations should establish standards that include engineering safeguards to prevent inadvertent waterway separation.
Discussion: The current applicable NFPA standard covering all types of motorized fire apparatus including those equipped with aerial ladders is NFPA 1901 Standard for Automotive Fire Apparatus 2003 Edition.8 This standard does not include specifications on how moveable waterways are to be anchored. NFPA 1901 does not specify the need for indicator lights or other means of verifying the position of moveable waterways. The presence of a visual indicator at the pump panel could provide operators of aerial ladders with an additional means to verify that the monitor is properly anchored. The presence of an electrical interlock switch that would not allow the aerial ladder to be operated unless the pin or other locking mechanisms are properly installed or locked is another means of ensuring safe and proper set-up before the aerial ladder can be operated.
Recommendation # 8: Business owners and property managers should address fire hazards and enforce fire prevention measures.
Discussion: Business owners and property managers can reduce the risk of injury and fatality to civilians, employees and fire fighters by addressing fire hazards and enforcing fire prevention measures. In this incident, the plastics manufacturing facility had a no smoking policy. State fire marshal investigators determined the fire was started by employees smoking in the loading dock area. The loading dock area contained a heavy fuel load consisting of wooden and plastic pallets and other flammable materials (Reference Photos # 7 through # 9). Enforcement of the no smoking policy would have prevented the fire which ultimately resulted in the fire fighter fatality.
Recommendation # 9: Municipalities, business owners, and authorities having jurisdiction should ensure fire hydrants are inspected and tested on a regular basis.
Discussion: Fire hydrants are the primary source of water supply for fire suppression operations in most municipal and residential settings across the country. It is imperative that fire hydrants function properly when needed. In this incident, fire fighters encountered difficulty in removing the cap from a yard hydrant located in the manufacturing plant’s parking lot. While this may not have directly contributed to the fatality, the difficulties encountered in connecting the supply hose from the hydrant to the aerial ladder truck undoubtedly raised the stress level of the fire fighters involved. Periodic inspection and testing of hydrants should take place on a regular basis to ensure proper function when needed.9 In this incident, the hydrant which was used to supply water to Ladder 287 was a yard hydrant located within the property of the manufacturing facility. NFPA 25 Standard for the Inspection, Testing, and Maintenance of Water-Based Fire Protection Systems, Chapter 7 provides the minimum requirements for the routine inspection, testing, and maintenance of private fire service mains and their appurtenances.9 NFPA 25, Chapter 7, Table 7.1 (Summary of Private Fire Service Main Inspection, Testing, and Maintenance) states hydrants should be inspected annually and after each use, and also flow tested annually. Tightness of outlet caps and worn outlet threads are included with the examples of conditions requiring corrective action.
REFERENCES
- NFPA [2007a]. NFPA 1911, Standard for the Inspection, Maintenance, Testing, and Retirement of In-Service Automotive Fire Apparatus, 2007 Edition. National Fire Protection Association, Quincy, MA.
- NFPA [1991]. NFPA 1904, Standard for Aerial Ladder and Elevating Platform Apparatus, 1991 Edition. National Fire Protection Association, Quincy, MA.
- Dunn [1999]. Command and Control of Fires and Emergencies. Saddlebrook, NJ: Fire Engineering Books & Videos, A Division of PennWell Books.
- NFPA [2007]. NFPA 1500, Standard on Fire Department Occupational Safety and Health Program, 2007 Edition. National Fire Protection Association, Quincy, MA.
- NFPA [2009]. NFPA 1002: Standard for Fire Apparatus Driver/Operator Professional Qualifications, 2009 Edition. National Fire Protection Association, Quincy, MA.
- Manufacturer letter to owners of aerial ladders with pinnable waterways. May 12, 2008.
- NFPA [2004]. NFPA 1720, Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Volunteer Fire Departments, 2004 Edition. National Fire Protection Association, Quincy, MA.
- NFPA [2003]. NFPA 1901: Standard for Automotive Fire Apparatus, 2003 Edition. National Fire Protection Association, Quincy, MA.
- NFPA [2008]. NFPA 25: Standard for the Inspection, Testing, and Maintenance of Water-Based Fire Protection Systems. 2008 Edition. National Fire Protection Association, Quincy, MA.
INVESTIGATOR INFORMATION
This investigation was conducted by Tim Merinar, Safety Engineer, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH and William Peters, of Peters Associates, Fire Apparatus Consulting Services, Inc. Mr. Peters is a retired Battalion Chief with over 28 years experience with the Jersey City, New Jersey Fire Department and is active in the National Fire Protection Association (NFPA) consensus standards process. This report was authored by Tim Merinar and William Peters. An expert technical review was conducted by Kevin Roche, Assistant Fire Marshal, Phoenix Fire Department and Jerry Halpin, President, Fire Apparatus Manufacturers’ Association (FAMA).
photos and diagrams
 |
 |
|
Photo 7. Loading dock area immediately after fire. Note the fuel load present on the loading dock consisting of wooden and molded-plastic pallets. |
 |
|
Photo 8. Plastic pallets and other plastic materials on the loading dock immediately after fire. |
 |
|
Photo 9. Photo shows the remains of the fuel load on the loading dock following the fire. . |
|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. To request additional copies of this report (specify the case number shown in the shield above), for other fatality investigation reports, or further information, visit the Program Website at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 02/06/09.