
Two Career Fire Fighters Die While Making Initial Attack on a Restaurant Fire - Massachusetts
Revised on November 13, 2009 to update Cause of Death Section.
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2007-32 Date Released: November 9, 2009
SUMMARY
On August 29, 2007 a 55-year-old male career fire fighter (Victim #1) and a 52-year-old male career fire fighter (Victim #2) died while conducting an interior attack to locate, confine, and extinguish a fire located in the cockloft of a restaurant. Upon arrival, fire was showing through the roof with negligible smoke and heat conditions in the main dining area. Victim #1 was on the nozzle flowing water on the fire in the ceiling area above the exhaust hood and duct work for the stove/broiler in the kitchen. His officer and the officer from the first arriving ladder company provided back-up on the 1 ¾-inch handline. Victim #2 was in the main dining area searching for fire extension above the suspended ceiling. Approximately five minutes after the first crew arrived on the scene, a rapid fire event occurred. Victim #1 was separated from his crew and was later found on the handline under debris with trauma to his head. Victim #2 had a lapel microphone with an emergency distress button which sounded a minute after the rapid fire event, likely from fire impingement. He was found in the area of the dining room where he was operating just before the rapid fire event occurred. Key contributing factors identified in this investigation include an insufficient occupational safety and health program, ineffective incident management system at the incident, insufficient incident management training and requirements, insufficient tactics and training, ineffective communications, delay in establishing a rapid intervention team (RIT), inadequate building code enforcement and development, and inadequate turnout clothing and personal protective equipment. NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
- develop, implement, and enforce an occupational safety and health program in accordance with NFPA 1500 Standard for a Fire Department Occupational Safety and Health Program
- ensure that their members are thoroughly trained, understand, and utilize the incident management system at all emergency incidents
- develop, implement and enforce written standard operating procedures (SOPs) that identify incident management training standards and requirements for members expected to serve in command roles
- ensure that the incident commander conducts an initial size-up and risk assessment of the incident scene before beginning interior fire fighting operations and continually evaluates the conditions to determine if the operations should become defensive
- ensure that the incident commander establishes a stationary command post, maintains the role of director of fireground operations, does not become involved in firefighting efforts, and that transfer of command follows established procedures
- develop, implement and enforce written standard operating procedures (SOPs) that address the hazards and define the strategies and tactics to be used while operating at specific structures known as “taxpayers”
- ensure that all fire fighters and officers receive fundamental and annual refresher training according to NFPA 1001 Standard for Fire Fighter Professional Qualifications and NFPA 1021 Standard for Fire Officer Professional Qualifications
- ensure that the initial attack line is charged and capable of controlling the fire conditions
- ensure that staffed back-up hoselines are utilized to protect the means of egress for the primary attack and search crews
- ensure that fire fighters immediately open ceilings and other concealed spaces whenever a fire is suspected of being above them
- use thermal imaging cameras (TICs) during the initial size-up and search phases of a fire
- ensure that fire fighters understand the influence of ventilation on fire behavior and coordinate with interior fire suppression operations
- train fire fighters to communicate interior and exterior conditions to the incident commander as soon as possible and to provide regular updates
- ensure that crew integrity is maintained during fire suppression operations
- ensure that a rapid intervention crew (RIC) / rapid intervention team (RIT) is established and available to immediately respond to emergency rescue incidents
- ensure that fire fighters wear a full array of turnout clothing and personal protective equipment that is certified by NFPA and appropriate for the assigned task while participating in fire suppression and overhaul activities
Additionally, code setting organizations and municipalities should:
- require the use of automatic ventilation systems in commercial structures, especially ones that have large void spaces and other unique life-safety hazards
- require that fire alarm systems installed in commercial structures incorporate heat and smoke detectors in large void spaces to improve life-safety
- require all commercial cooking operations to have periodic inspections of their kitchen exhaust systems and require all kitchen exhaust system installers to be certified to nationally recognized standards
Additionally, the National Fire Protection Association (NFPA) should:
- consider developing more comprehensive training requirements for fire behavior to be required in NFPA 1001 Standard for Fire Fighter Professional Qualifications and NFPA 1021 Standard for Fire Officer Professional Qualifications
INTRODUCTION
On August 29, 2007 a 55-year-old male career fire fighter (Victim #1) and a 52-year-old male career fire fighter (Victim #2) died while conducting an interior attack to locate, confine, and extinguish a fire located in the cockloft of a restaurant. On August 30, 2007 the U.S. Fire Administration and the International Association of Fire Fighters (IAFF) notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On September 9-12, 2007, a Safety and Occupational Health Specialist, a General Engineer, and a Safety Engineer from the NIOSH Fire Fighter Fatality Investigation and Prevention Program traveled to Massachusetts to conduct meetings with the fire department, representatives of the IAFF, representatives of the Bureau of Alcohol, Tobacco and Firearms (ATF), the city’s building code enforcement office, and the department’s training academy. On December 2-4 two NIOSH investigators (a Safety and Occupational Health Specialist and the Safety Engineer) returned to Massachusetts to conduct interviews with the fire fighters and officers who were directly involved with this incident. The investigators reviewed the victims’ training records, the department’s training requirements, the department’s standard operating procedures (SOPs), witness statements, dispatch logs, the victims’ personal protective equipment, death certificates, and photos and sketches of the incident site.
FIRE DEPARTMENT
This career department consists of 1,600 uniformed fire fighters. The department has 35 fire stations and serves a population of about 600,000 in a geographic area of approximately 45 square miles.
PERSONAL PROTECTIVE EQUIPMENT (PPE)
Both victims were wearing a bunker coat, station pants, and safety boots. The bunker coats that were worn by the victims, and issued by the department, were reported by the manufacturer to meet the requirements of NFPA 1971.
The victims used Scott Life-Pak Fifty 4.5 Self Contained Breathing Apparatus (SCBA) equipped with integrated Pak-Alert SE Personal Alert Safety System (PASS) devices.
TRAINING and EXPERIENCE
The state has no minimum training requirements to become fire fighters. At the time of this incident, the fire department provided the training for recruits to meet the state’s suggested curriculum for NFPA Fire Fighter I and II.
Victim #1 was a fire fighter with more than 14 years of experience. He had received training on topics such as the maze drill, EMS responder, CPR/AED, and scene size-up. Victim #2 was a fire fighter with more than 19 years of experience. He had received training on topics such as the maze drill, EMS responder, CPR/AED, and ICS.
The fire department provides annual training to fire fighters according to their company functions or specialties. Both of the victims and their companies should have received annual fire training according to their functions which included “Back to Basics.” The “Back to Basics” drill consisted of companies advancing handlines and deploying ground ladders during live-fire training at the fire department’s fire academy. However, the fire department’s burn building at the academy had been condemned as being unsafe to conduct live-fire training; therefore, the fire department had suspended the “Back to Basics” training for several years prior to this incident.
STRUCTURE
The building was constructed in 1930 and was a single-story “taxpayer”a of ordinary construction. The building consisted of four commercial occupancies that were all in business at the time of the fire. The occupancy where this fatal fire occurred was the second occupancy from left to right in this building and had been a Chinese restaurant since 1955.
The dimensions of the building were 90 ft wide by 60 ft deep. The restaurant was 32 ft wide by 60 ft deep with a suspended ceiling being approximately 9 ft high. The restaurant did not have a common cockloft or basement with the other occupancies of the building. The suspended ceiling consisted of painted 12-inch cellulose tiles that were stapled to wood furring strips. There was a 17 inch void space between the suspended and the original ceilings. The original ceiling consisted of stamped sheet metal that was attached directly to the ceiling joists. Due to the slope of the roof, the void space above the original ceiling to the bottom of the roof deck varied from 17 inches in the rear to 30 inches in the front.
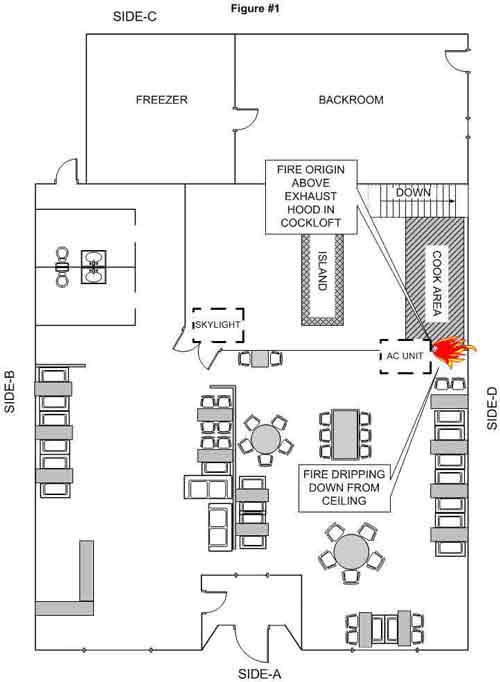
A single exterior door in the front led into a vestibule just inside the restaurant. There was another door to the left inside the vestibule which led into the dining area. The dining area was carpeted and had a maximum capacity of 80 customers. Seating consisted of fixed booths and portable tables in the center on the right hand side. The left hand side consisted of an aisle flanked with booths that led to the restrooms, kitchen, and a rear exit (Figure 1).
The kitchen was in the right rear of the restaurant and was approximately 18 ft 6 in x 16 ft 6 in. Access was through a set of swing doors. It had a fixed center food prep table that had a suspended metal rack for storing cookware and supplies. There was an addition on the rear of the kitchen which consisted of a storage room and a walk-in freezer (Figure 1).
The interior walls (demising partition) on the B-side and D-side were also of ordinary construction (brick, wood and plaster) and separated the restaurant from its exposures from the floor to the bottom of the roof deck.
The roof was sloped towards the back and had a 3 ft parapet wall on the front. It consisted of built-up rubber roofing with backer board over the original tar and gravel roof. There was a 3-ton heating, venting, and air conditioning unit (HVAC) on the roof, that weighed approximately 400 pounds. There was also a skylight that measured 3 ft 8 in x 3 ft 5 in. Both were located over the kitchen area (Figure 1).
a A commercial structure built of ordinary construction (Type-III) that is subdivided to hold various commercial occupancies. Typically one-story, but may be two-stories with apartments on the second floor.
KITCHEN EXHAUST SYSTEM and DUCTWORK
After the fatal fire, the exhaust system had been inspected by the fire department, the business owner, a fire protection equipment company, and a contracted engineering firm. The system consisted of galvanized sheet metal ranging from 26-gauge to 22-gauge thickness that is typically found in residential heating and cooling applications. It was connected with sheet metal screws and dovetail joints used in heating and cooling operations.
WEATHER CONDITIONS
The conditions were clear with the temperature averaging 70-degrees Fahrenheit. The wind was between 9 and 20 miles per hour with gusts up to 24 miles per hour from the South.
EQUIPMENT and PERSONNEL
Only the first alarm response and companies directly involved in this incident are included
Ladder 25, on-the scene at 2108 hours
Officer (initial Incident Commander), Driver/Operator, Victim #2, Fire fighter
Engine 30
Officer, Driver/Operator, Victim #1, Fire fighter
Engine 53
Officer, Driver/Operator, 2 Fire fighters
Engine 55
Officer, Driver/Operator, 2 Fire fighters
Ladder 16
Officer, Driver/Operator, 2 Fire fighters
Rescue 2
Officer, Driver/Operator, 2 Fire fighters
District 10, on the scene at 2111 hours
District Chief (Incident Commander)
Division 12
District 12
Division 2
Acting Deputy Chief
INVESTIGATION
On August 29, 2007 at 2104 hours, a restaurant employee called 911 to report a fire where he was working. At 2106 hours, the Fire Alarm Office (FAO) dispatched a first alarm assignment which included Engine 30 (E30), Engine 53 (E53), Engine 55 (E55), Ladder 25 (L25), Ladder 16 (L16), Rescue 2 (R2), and District 10 (D10). D10 acknowledged the call at 2107 hours.
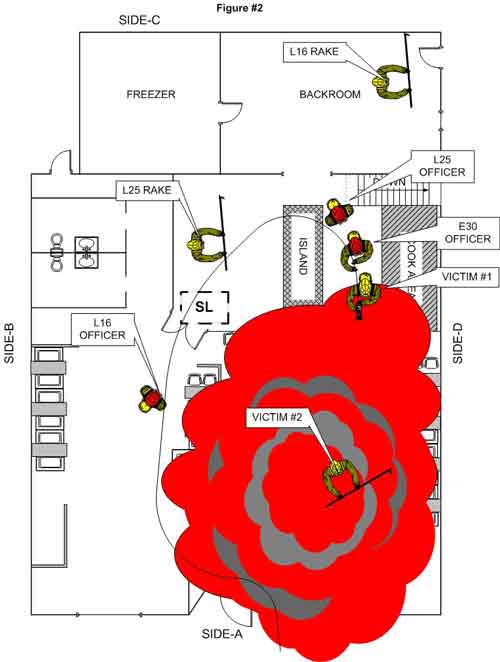
L25 was the first to arrive on-the-scene at 2108 hours, assumed incident command and reported fire showing from the roof. E30 arrived on the scene shortly thereafter and connected to a hydrant with a 4-inch supply line. The officer from L25 entered the restaurant with no smoke conditions in the front seating area. He proceeded into the kitchen in the right rear of the restaurant. He observed fire in the ceiling above the exhaust hood with light smoke conditions in the kitchen (Figure 2). L25 raised the aerial ladder to the front side of the A-B corner and the L25 driver climbed the ladder to the roof with a rake, axe, and a power saw. The roof felt spongy as the L25 driver noted heavy gray smoke pushing from the cupola. The L25 driver went to the rear of the roof to size-up the conditions. He noticed fire extending from beneath the air conditioning (AC) unit, heavy smoke from the vent nearest the AC unit, and light smoke from the far roof vent (Photo 1, Photo 2). The L25 driver could not remove the top of the vent nearest the AC unit. He started to cut a ventilation hole in the roof towards the front of the building beside the cupola. The E30 officer and E30 pipeman (Victim #1) advanced a 1 ¾-in uncharged handline into the front of the restaurant. The E30 officer and Victim #1 encountered smoke conditions in the kitchen and put on their facepieces. The officer from E30 exited the structure to request that his line be charged as the L25 open-up man entered the structure (Victim #2).
The L25 officer got information from a civilian about the possibility of pets being boarded in the basement of the B-side exposure. At 2109 hours the officer from L25 called for a second alarm to cover the exposure. The L25 officer then radioed the E30 pump operator and ordered the E30 handline to be charged. At 2111 hours D10 arrived on the scene and called the FAO and took command of the incident (IC). He did a size-up from his position at the front of the structure and noticed fire extending from the roof and a handline entering the front door to the restaurant. He only saw the E30 fire fighter hooking up the hydrant and assumed he had seven fire fighters inside the structure.
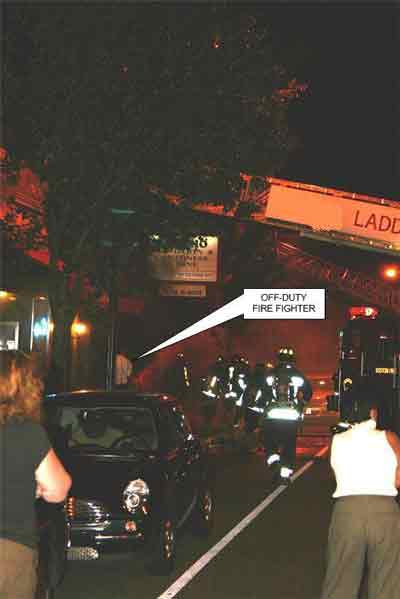
During this time, L16 arrived on the scene and the officer and a L16 open-up man entered the restaurant. The L16 officer ordered the L16 rakeman to assist Engine 53 (E53). The L25 officer and a L25 rakeman followed the crew from L16 and entered the restaurant. They proceeded to the rear of the dining room. The L25 officer and the L16 open-up man removed the left side of the swinging doors leading into the kitchen area. Note: The L16 officer noticed fire dripping down from the ceiling on the D-side wall adjacent to the kitchen area (see Figure #1). He described it as appearing to be dripping plastic or grease from the void space above the drop ceiling. He noticed that the fire was burning through the wood roof joists. The L25 open-up man (Victim #2) was off towards the D-side in the dining area. At approximately the same time, the E30 officer had re-entered and was backing up Victim #1 on the nozzle flowing water on the fire from inside the kitchen. The L25 officer was behind the E30 officer on the handline. The E30 fire fighter moved to the other side (C-side) of a center island in the kitchen to get a better angle on the fire located in the C-D corner of the kitchen. After removing the swing door, the L16 fire fighter saw that the kitchen was congested and exited to check for extension into the B-side exposure. When he turned to exit he noticed in the ceiling area what appeared to be “red lines” glowing. They were running from front to back. During this time, an off-duty fire fighter arrived on the scene. D10 had the off-duty fire fighter vent the front windows (Photo 3, Photo 4). Note: It is believed that the L16 fire fighter saw the wood furring strips that the ceiling tiles were attached to glowing with fire. When the L16 fire fighter exited, he also noticed that the window on the left side of the front door had been removed. It was intact when he entered. The L16 officer requested another handline from D10 to the first floor front.
During this time the L16 fire fighter was on the roof assisting the L25 fire fighter cut the ventilation hole. The L25 fire fighter made four cuts and his saw stalled. Engine 53 was ordered by D10 to stretch a 2½-in handline into the B-side exposure. The L25 driver told the L16 rakeman to open up any doors in the rear of the structure.
At approximately 2112 hours, the L25 officer told the L25 rakeman to stay with the handline as he went to look for an exit in the rear of the structure. The E30 officer and Victim #1 started to hear popping from the ceiling as it was coming down upon them. The smoke and heat conditions intensified forcing them to the floor. The L16 officer moved from the C-side of the dining room over to E30’s handline due to the deteriorating conditions. The smoke conditions were now banking to the floor and the heat forced the L16 officer to his knees. At approximately 2113 hours, as he awaited for the additional handline, he heard a loud crack and within a minute heard a loud rush. He described it as sounding like a “freight train” as a rapid fire event took place blowing down the ceiling tiles and a fireball blew out of the front of the structure (Photo 5, Photo 6). He described that the dining room turned orange. He felt hot water falling on him from the E30 handline in the kitchen (Figure 2).
The L25 officer returned to the kitchen. He could not find an exit due to the heavy smoke conditions. The smoke and heat conditions in the kitchen area were significantly worse. The smoke was banked to the floor with zero visibility and intense heat conditions. The L25 officer could hear Victim #1 flowing water. He followed the sound and told the E30 officer and Victim #1 to exit the structure. They all turned and started to exit the kitchen. They became tangled up in the debris that was falling from the kitchen as they attempted to get their bearings. The L25 and E30 officers found the double kitchen doors and knew they had a straight line to the front. They thought that Victim #1 was with them. They exited as the L25 officer was out of air and the E30 officer’s low-air alarm was sounding. Note: It is believed that Victim #1 attempted to follow the handline which led him towards the rear of the structure (Photo 7). The L25 rakeman got separated from the officers and remained in the kitchen.
At 2114 hours Victim #2’s emergency distress signal was received by the FAO. At this time, the L16 open-up man was back at the front of the restaurant after checking for extension in the B-side exposure. He was removing the front window to the right side of the door. Note: This was after the fire event and there weren’t any flames, only smoke coming from the window to the left of the front door (Photo 8). The L25 and E30 officers exited stating that there were fire fighters still inside. The E30 hydrant man followed the handline through the front door. Visibility was zero with extreme heat conditions coming from the right side of the dining room area and into the kitchen. The E30 hydrant man ran into the L25 rakeman in the kitchen while looking for the E30 crew. The L25 rakeman did not know the location of the E30 crew. The E30 hydrant man followed the handline until he encountered the center workstation in the kitchen and his low-air alarm was sounding. He was forced to turn around and follow the handline, and he and the L25 rakeman backed out of the building.
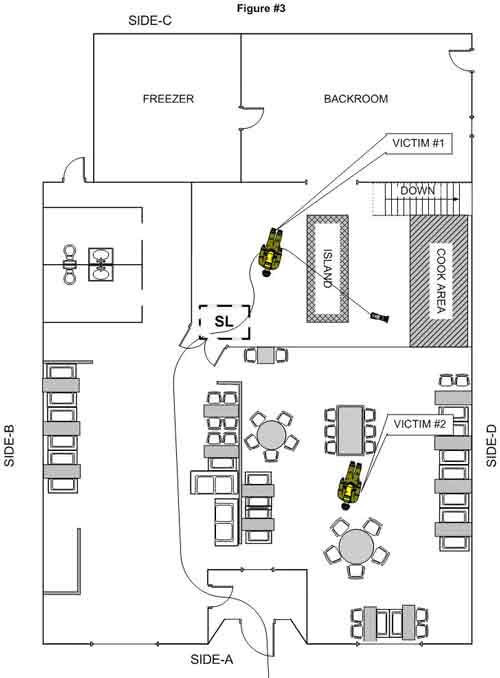
At 2115 hours the FAO called the IC to inform him that they had received Victim #2’s emergency distress signal. Note: The FAO continued to call Victim #2 on all of the channels with no response. District 12 was informed by the IC that there were two fire fighters missing; the IC then went to the rear of the structure to initiate a search with the Rescue 2 (R2) officer and two additional members from R2 who had just arrived on the scene. At 2118 hours District 12 arrived, called the FAO, and requested an engine company to provide protection for R2 while they conducted their search. R2 members heard a PASS device and found Victim #1 with his handline. He was face down, his helmet and facepiece were off, and he was covered with debris (Figure 3, Photo 7). The members had difficulty removing Victim #1 due to him being entangled in debris and wires. After he was removed, emergency medical treatment was initiated enroute to the local hospital where he was pronounced dead. Note: Victim #1 had trauma to his head at the hairline level. It was reported by his crew members that he was on air when he was operating the handline before the rapid fire event. It is believed that the trauma happened after the rapid fire event and possibly contributed to him removing his facepiece.
During this time, the L16 open-up man entered through the front door and had difficulty entering due to debris that was covering the floor. E55 repositioned their handline through the right window on the A-side and advanced approximately 10-15 feet inside the dining area. All three members of E55 received burns to their knees because the floor was extremely hot as they fought fire in zero visibility conditions. The L16 open-up man crawled over tables and piles of debris with visibility inside the dining area near zero due to the dark smoke. He was hit by a hose stream and it knocked off his helmet. He found his helmet and then saw a red light. He went to the red light and found Victim #2 sitting up facing the kitchen with his facepiece on and his helmet off (Figure 3). Note: The red light was from Victim #2’s radio. He yelled for help as he tried to free Victim #2 who was caught under debris. Members from E55 arrived and assisted with the removal of Victim #2’s SBCA in order to free him from the debris. Note: None of the members assisting with finding and removing Victim #2 remembered hearing his PASS device. He was then removed through the front right window. Emergency medical treatment was initiated enroute to the local hospital where he was pronounced dead.
CAUSE OF DEATH
The death certificate listed the causes of death for Victim #1 and Victim #2 as thermal injuries and asphyxia. Note: There have been media reports of alleged substance abuse that were discovered during the toxicological screening of both victims. NIOSH requested a copy of the autopsy reports from several different sources, including the fire department, fire commissioner, medical examiner’s office, and the district attorney’s office, but was not able to obtain any official toxicology information; therefore, NIOSH is not able to comment on the alleged condition of the victims.
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:
- Insufficient occupational safety and health program.
- Ineffective incident management system at the incident.
- Insufficient incident management training and requirements.
- Insufficient tactics and training.
- Ineffective communications.
- Delay in establishing a rapid intervention team.
- Inadequate building code enforcement and development.
- Inadequate turnout clothing and personal protective equipment.
RECOMMENDATIONS
Recommendation #1: Fire departments should develop, implement and enforce an occupational safety and health program in accordance with NFPA 1500 Standard for a Fire Department Occupational Safety and Health Program.
Discussion: The risk for fatal injury among fire fighters is high compared to other occupations.1 There is an increasing body of scientific literature demonstrating that organizational practices that demonstrate top level management commitment to safety, establish and foster compliance with safety policies and practices, and involve workers in identifying safety hazards and promoting solutions are effective in reducing worker injuries.2-7 Many of these concepts are embodied in NFPA 1500, Standard for a Fire Department Occupational Safety and Health Program.8 Implementation of a strong fire department occupational safety and health program following written procedures and policies such as those outlined by NFPA 1500 can foster and improve the overall safety climate of a fire department, as well as improve specific safety and health areas, such as respiratory protection, risk management, training and competency in fireground operations, tactics, and equipment and apparatus use. NIOSH investigators reviewed the department’s SOPs which are standard methods or rules in which an organization or a fire department operates to carry out a routine function. The department’s SOPs did not effectively cover areas such as risk management, competency in fireground operations, fitness for duty, and training. Operational procedures should be standardized, clearly written, and mandated to each department member. This will establish accountability and increase command and control effectiveness. 9 The benefits of having clear, concise, and practiced SOPs are numerous. For example, they can become a training outline and a tool to guide fire department members. Above all, well applied and training on SOPs improve departmental safety. 10
Recommendation #2: Fire departments should ensure that their members are thoroughly trained, understand, and utilize the incident management system at all emergency incidents.
Discussion: NFPA 1500 Standard on Fire Department Occupational Safety and Health Program8 and NFPA 1561 Standard on Emergency Services Incident Management System11 both state that an incident management system (IMS) should be utilized at all emergency incidents (including but not limited to training exercises). NFPA 1561, Chapter 5.3.6 states, “SOPs shall define the circumstances and procedures for transferring command to another on-scene officer/member and shall specify to whom command shall be transferred.”
Annex A states “the fire department of the emergency services organization (ESO) should establish a protocol of command authority based on rank structure, assignments, and qualifications to define a hierarchy for transferring command. The qualifications required to perform as incident commander should increase with the size and complexity of the incident. SOPs should define the circumstances under which an officer at a higher level should respond to an incident and whether the transfer of command to an officer at a higher level is mandatory or discretionary.”
The fire department in this incident had a standard operating procedure covering the implementation of the IMS but it was not followed and proved to be ineffective at this incident. The IMS should include written plans that address the requirements of different types of incidents that can be anticipated in each fire department’s or ESO’s jurisdiction. The IMS should address both routine and unusual incidents of differing types, sizes and complexities. The IMS covers more than just fireground operations. The IMS must cover incident command, accountability, risk management, communications, rapid intervention teams (RIT), roles and responsibilities of the incident safety officer (ISO), and inter-operability with multiple agencies (police, emergency medical services, state and federal government, etc.) and surrounding jurisdictions (mutual aid responders).
NIOSH investigators identified several examples in this incident in which recognized guidelines for IMS were not followed. Specific examples include: incident command was not established by the first arriving officer, incident command was never formally transferred, lack of an established accountability system to track fire fighters on scene, no safety officer was assigned, and a RIT was not established before conducting interior operations.
Recommendation #3: Fire departments should develop, implement and enforce written standard operating procedures (SOPs) that identify incident management training standards and requirements for members expected to serve in command roles.
Discussion: NFPA 1561 Standard on Emergency Services Incident Management System, Chapter 4.8.3 states “responders who are expected to perform as incident commanders or to be assigned to supervisory levels within the command structure shall be trained in and familiar with the incident management system and the particular levels at which they are expected to perform.” 11 NFPA 1001 Standard for Firefighter Professional Qualifications,12 NFPA 1021 Standard for Fire Officer Professional Qualifications,13 NFPA 1500 Standard on Fire Department Occupational Safety and Health Program 8 and 1521 Standard for Fire Department Safety Officer 14 are just a few examples of recognized standards addressing fire fighter and officer qualifications.
One of the fire officer’s primary responsibilities is safety both on the fireground and during normal operations. A partial list of officer qualifications (knowledge, skills, and abilities) necessary to accomplish the primary responsibility of fireground safety identified in these standards include: fire behavior; building construction; conducting pre-incident planning; applicable codes, ordinances, and standards; identification of fire and life safety hazards; supervising emergency operations; and deploying assigned resources in accordance with the local emergency plan. NIOSH investigators reviewed the department’s training requirements for fire fighters and first line supervisors. IMS was not included in any of the training requirements at any level within the fire department or at the department’s fire academy.
Recommendation #4: Fire departments should ensure that the incident commander conducts an initial size-up and risk assessment of the incident scene before beginning interior fire fighting operations and continually evaluates the conditions to determine if the operations should become defensive.
Discussion: Among the most important duties of the first officer on the scene is conducting an initial size-up of the incident. This information lays the foundation for the entire operation. It determines the number of fire fighters and the amount of apparatus and equipment needed to control the blaze, assists in determining the most effective point of fire extinguishment attack, the most effective method of venting heat and smoke, and whether the attack should be offensive or defensive. A proper size-up begins from the moment the alarm is received and it continues until the fire is under control. The size-up should also include assessments of risk versus gain during incident operations. 9, 15-19 Retired Chief Alan Brunacini recommends that the arriving IC drive partially or completely around the structure whenever possible to get a complete view of the structure. While this may delay the IC’s arrival by a few seconds, this drive-by may provide significant details not visible from the command post.17 The size-up should include an evaluation of factors such as the fire size and location, length of time the fire has been burning, conditions on arrival, occupancy, fuel load and presence of combustible or hazardous materials, exposures, time of day, and weather conditions. Information on the structure itself to include size, construction type, age, condition (evidence of deterioration, weathering, etc), evidence of renovations, lightweight construction, loads on roof and walls (air conditioning units, ventilation ductwork, utility entrances, etc.), and available pre-plan information are all key information which can effect whether an offensive or defensive strategy is employed. The size-up and risk assessment should continue throughout the incident.
Fires in commercial structures are typically more dangerous than residential building fires. Retired Assistant Chief Vince Dunn states that defensive operations should be used more often at special occupancy and commercial buildings. Chief Dunn cites statistics that 4 fire fighters die for every 100,000 residential fires compared to 9 fire fighter deaths for every 100,000 commercial structure fires.20
Interior size-up is just as important as exterior size-up. Since the IC is staged at the command post (outside), the interior conditions should be communicated to the IC as soon as possible. Interior conditions could change the IC’s strategy or tactics. For example, if heavy smoke is emitting from the exterior roof system, but fire fighters cannot find any fire in the interior, it is a good possibility that the fire is above them in the roof system. Other warning signs that should be relayed to the IC include dense black smoke, turbulent smoke, smoke puffing around doorframes, discolored glass, and a reverse flow of smoke back inside the building. It is important for the IC to immediately obtain this type of information to help make the proper decisions. Departments should ensure that the first officer or fire fighter inside the structure evaluates interior conditions and reports them immediately to the IC.
In this incident, a 360 degree size-up was never conducted. There was no pre-planning information available on the construction features or any other potential hazards associated with the occupancy of this structure. Smoke showing from the roof upon arrival, failure to conduct vertical ventilation, inability to hit the seat of the fire, and the rapid decrease in visibility coupled with a rapid rise in temperature were all indicators that could have prompted consideration of switching from offensive to defensive strategies.
Recommendation #5: Fire departments should ensure that the incident commander establishes a stationary command post, maintains the role of director of fireground operations, does not become involved in firefighting efforts, and that transfer of command follows established procedures.
Discussion: According to NFPA 1561 Standard on Emergency Services Incident Management System, §5.3.1, “the incident commander shall have overall authority for management of the incident.” 11 In addition to conducting an initial size-up, the incident commander must establish and maintain a command post outside of the structure to assign companies and delegate functions, and continually evaluate the risk versus gain of continued fire fighting efforts. In establishing a command post, the incident commander shall ensure the following (NFPA 1561, §5.3.7.2):
- The command post is located in or tied to a vehicle to establish presence and visibility.
- The command post includes radio capability to monitor and communicate with assigned tactical operations, command, and designated emergency traffic channels for that incident.
- The location of the command post is communicated to the communications center.
- The incident commander, or his or her designee, is present at the command post.
- The command post should be located in the incident cold zone.
The use of a tactical worksheet can assist the IC in keeping track of various task assignments on the fireground. It can be used along with pre-plan information and other relevant data to integrate information management, fire evaluation and decision making. The tactical worksheet should record unit status, benchmark times, and include a diagram of the fireground, occupancy information, activities checklist(s), and other relevant information. This can also aid the incident commander in continually conducting a situation evaluation and maintaining accountability. 17 To effectively coordinate and direct fire fighting operations on the scene, it is essential that the IC does not become involved in fire fighting efforts. A delay in establishing an effective command post may result in confusion of assignments and lack of personnel and apparatus coordination which may contribute to rapid fire progression. The involvement of the initial IC in fire fighting also hampers the collection and communication of essential information as command is transferred to later arriving officers.
In this incident, a stationary command post was never established and separate and uncoordinated activities were taking place in multiple locations. This contributed to a failure to size-up the overall incident scene, properly evaluate risk versus gain, communicate and evaluate fireground operations, transfer command, and maintain accountability on the fireground.
Recommendation #6: Fire departments should develop, implement and enforce written standard operating procedures (SOPs) that address the hazards and define the strategies and tactics to be used while operating at specific structures known as “taxpayers.”
Discussion: The term “taxpayer” is not a classification or term recognized by the national building codes. It is a term commonly used to describe a commercial structure that is one or two stories in height of ordinary or Class III construction. The term originated in the early 1900s when real estate investors built structures for income to offset the cost of taxes. Minimal money was invested in construction of these properties and they were built without regard to fire retarding features.21 Taxpayer construction presents a serious challenge for fire fighting. They have many unique construction features that can contribute to rapid fire spread and instability. Many of these structures have been modified over the years to accommodate numerous occupants or to change the aesthetics. The construction features and modifications may not be obvious during fire fighting operations because they are either obscured by smoke or are covered by finishing materials. It is imperative that the SOPs address the various construction methods, materials, and modifications in these structures, the effects fire can have on them, and what to expect on the fireground. The SOPs should address the tactics to be used to accomplish fire control and fire fighter safety. The standard evolution of attack on a taxpayer fire is:
- Forcible entry
- Ventilation
- Pull ceilings
- Advance handline and extinguishment21
In this incident, the single-story taxpayer had a cockloft, which is the space above the finished ceiling and the underside of the roof. It tapered in height from 30 inches in the front to 17 inches in the back for the slope of the roof. There was a drop ceiling of combustible tiles below the original finished ceiling of stamped tin creating another void space that was 17 inches in height. These void spaces hid a large amount of combustible material and created a plenum for fire travel and the build-up of fire gases. This area also concealed the accumulation of grease from the years of operating as a restaurant with a deficient kitchen exhaust system. The ceiling was not pulled to search for fire and vertical ventilation was not completed prior to the initial attack team making entry.
Recommendation #7: Fire departments should ensure that all fire fighters and officers receive fundamental and annual refresher training according to NFPA 1001 Standard for Fire Fighter Professional Qualifications and NFPA 1021 Standard for Fire Officer Professional Qualifications.
Discussion: Initial and continual training provides an opportunity to ensure that all fire fighters and officers are proficient in their knowledge and skills in recognizing and mitigating hazards. Training on structural fire fighting should include, but not be limited to, departmental standard operating procedures, fire fighter safety, building construction, and fireground tactics. NFPA 1500 Standard for a Fire Department Occupational Safety and Health Program, Chapter 5, requires that the fire department provide an annual skills check to verify minimum professional qualifications of its members.8 NFPA 1001 Standard for Fire Fighter Professional Qualifications was established to facilitate the development of nationally applicable performance standards for uniformed fire service personnel.12 NFPA 1021 Standard for Fire Officer Professional Qualifications was developed in the same way to determine that an individual possesses the skills and knowledge to perform as a fire officer.13 The intent of these standards is to develop clear and concise job performance requirements (JPRs) that can be used to determine that an individual, when measured to the standard, possesses the skills and knowledge to perform as a fire fighter or a fire officer, and that these JPRs can be used by any fire department in the country.
Training is an ongoing process, whether held daily, weekly or monthly, it allows members to maintain proficiency at their present levels, meet certification requirements, learn new procedures, and keep up with emerging technology. Prior to this incident, the department provided their own training and requirements to recruits and members. The basic training provided by the fire department at the time of this incident did not meet NFPA Fire Fighter I requirements, and the department did not have a process to verify minimum professional qualifications.
Recommendation #8: Fire departments should ensure that the initial attack line is charged and capable of controlling the fire conditions.
Discussion: Taxpayer fires can be difficult to control and extinguish, especially when they have advanced into recessed areas such as a cockloft. If heavy to medium fire conditions are encountered upon arrival, the initial attack lines should be 2 ½ inch handlines. The volume and striking power of the larger handline can prevent the fire from intensifying and reaching an advanced stage on the initial deployment. 21 According to Dunn, the most important fire fighting operation at a structure fire is stretching the first attack hoseline to the fire. 15, 16 A properly positioned and functional fire attack line saves the most lives during a fire. 16 “It confines the fire and reduces property damage. Searches will proceed quickly, rescues will be accomplished under less threat, sufficient personnel will be available for laddering, ventilation will be effective, and overhaul above the fire room will be unimpeded.” 15
In this incident, the initial crew stretched an uncharged 1 ¾ inch handline into the kitchen. The delay in charging the hoseline and the reduced reach, volume, and penetration of the initial 1 ¾ inch handline was not sufficient to control the fire which was seated in the void spaces of the cockloft.9 The fire conditions continued to grow rapidly and build up smoke and fire gases within the cockloft area which was over 8,000 cubic feet. As hot smoke radiates it heats other combustibles, increases pyrolysis and adds more flammable fuel to the gas layer. 9 The larger 2 ½ inch handline may have been able to penetrate into the void spaces with adequate volume to cool down the hot gas layer, reducing the chance of these gases igniting or a rapid fire event occurring.
Recommendation #9: Fire departments should ensure that staffed back-up hoselines are utilized to protect the means of egress for the primary attack and search crews.
Discussion: Back-up lines are not used to attack fire in another area or for exposure control. They are deployed, charged, and on stand-by in the same general area to back-up an attack line.22 In this incident a 2 ½ inch line was not pulled and directed into the exposure. As the fire conditions in the cockloft intensified, the hot layer of smoke began to extend down to the floor level. At this time, there was no way to control the fire spread and allow fire fighters a safe egress path. If a back-up line had been in place, it is possible that the fire build up could have been mitigated by penetrating through the suspended ceiling and cooling down the hot gas layer. The back-up hoseline could have also maintained an egress for fire fighters who were operating with the primary attack line.
Recommendation #10: Fire departments should ensure that fire fighters immediately open ceilings and other concealed spaces whenever a fire is suspected of being above them.
Discussion: Fire fighters may have difficulty in finding the exact location of fire in a building, even though heavy smoke makes it clear that fire is present. Fire or heavy smoke from the roof suggests that the fire could be in concealed areas of the roof system. The cockloft area provides a void space that hides large amounts of exposed wood, multiple ceilings, piping, wiring, and air handling ductwork. 21 The factors of a large area with heavy fire loading can result in rapid fire spread.23 The enclosure of the void space allows for the hot gases to accumulate which may flash when oxygen is introduced.21, 24 When the fire is suspected to be above a ceiling, fire fighters should use a pike pole or other tools to open up the ceiling immediately and check for extension. Any ceiling below a void should be pulled and examined by fire fighters while standing near a doorway for rapid escape or in case of total failure. When opening ceilings or other concealed spaces, it is important to have charged hoseline(s) ready.24 If there is a fire barrier in the void, the same procedure should take place on the opposite side. If the fire emerges behind the fire fighter, egress may be cut off, leading to the possibility of entrapment. Fire fighters need to be aware of their location in relation to the nearest exit and also be aware of the location of other fire fighters in the area. The incident commander must consider and provide for alternative egress routes from locations where fire fighters are operating. 24, 25
Recommendation #11: Fire departments should use thermal imaging cameras (TICs) during the initial size-up and search phases of a fire.
Discussion: Thermal imaging cameras (TICs) can be a useful tool for initial size up and for locating the seat of a fire. Infrared thermal cameras can assist fire fighters in quickly getting crucial information about the location of the source (seat) of the fire from the exterior of the structure which can help plan an effective and rapid response. Knowing the location of the most dangerous and hottest part of the fire may help fire fighters determine a safer approach and avoid exposure to structural damage in a building that might have otherwise been undetectable. Ceilings and floors that have become dangerously weakened by fire damage and are threatening to collapse may be spotted with a thermal imaging camera. A fire fighter about to enter a room filled with flames and smoke can use a TIC to assist in judging whether or not it will be safe from falling beams, walls, or other dangers. The use of a TIC may provide additional information the incident commander can use during the initial size-up. TICs should be used in a timely manner, and fire fighters should be properly trained in their use and be aware of their limitations.26
The use of a TIC during initial size-up and entry into the structure might have confirmed the extent of hot smoke and gases in the concealed space above the suspended ceiling, the location of the seat of the fire, and possibly the best area for attack.
Recommendation #12: Fire departments should ensure that fire fighters understand the influence of ventilation on fire behavior and coordinate with interior fire suppression operations.
Discussion: Ventilation is the systematic removal and replacement of heated air, smoke, and gases from inside a structure with cooler air. It is critical that fire fighters understand the influence of ventilation on fire behavior and the fire environment. Increasing ventilation to a ventilation controlled fire will result in an increased heat release rate, and may result in extreme fire behavior such as ventilation induced flashover or backdraft. However, effective tactical ventilation closely coordinated with fire attack can significantly reduce the potential for extreme fire behavior and increase tenability. Close coordination means the hoseline is in place and ready to operate so that when ventilation occurs, the hoseline can overcome the increase in combustion likely to occur. If a ventilation opening is made directly above a fire, fire spread may be reduced, allowing fire fighters the opportunity to extinguish the fire. If the opening is made elsewhere, the chimney effect may actually contribute to the spread of the fire.9, 27
In this incident, vertical ventilation was never completed. The initial attack team and the initial IC were inside the structure fighting fire in the cockloft area that was open in the kitchen. The fire conditions worsened in the dining room area as thick black smoke began to bank down to the floor. Horizontal ventilation was performed on the front windows, which flanked the point of egress for the crews working inside. This provided oxygen to the fire and lead to a rapid fire event.
Venting can be a very effective life safety procedure. When venting for life safety purposes, the principle is to pull the fire, heat, smoke and toxic gases away from victims, stairs, and other egress routes. A vent opening made between the fire fighter or victims and their path of egress could be fatal if the fire is pulled to their location or cuts off their path of egress.27
Recommendation #13: Fire departments should train fire fighters to communicate interior and exterior conditions to the incident commander as soon as possible and to provide regular updates.
Discussion: Proper size-up and risk versus gain analysis requires that the incident commander have a number of key pieces of information and keep informed of the constantly changing conditions on the fireground. New decisions must be made and old ones revised based upon increased data and improved information. Decisions can be no better than the information on which they are based. The incident commander (IC) must use an evaluation system that considers and accounts for changing fireground conditions in order to stay ahead of the fire. If this is not done, the attack plan will be out of sequence with the phase of the fire and the IC will be constantly surprised by changing conditions17, 19, 28 Interior size-up is just as important as exterior size-up . Since the IC is staged at the command post (outside), the interior conditions should be communicated by interior crews as soon as possible to the IC. Interior conditions could change the IC’s strategy or tactics. Interior crews can aid the IC in this process by providing reports of the interior conditions as soon as they enter the fire building and by providing regular updates. According to Chief Dunn, one such example would be whenever a suspended ceiling is discovered in a commercial structure, this information should be immediately communicated to the IC.28
Upon arrival the initial IC reported to the FAO that fire and smoke was showing from the roof. The smoke in the dining room was negligible when the initial attack team made entry, but they had fire overhead in the kitchen. During NIOSH interviews, fire fighters and officers who had operated inside the structure and fire fighters who worked on the roof reported signs of deteriorating conditions to the NIOSH investigators. However, no interior condition reports were broadcast over the radio, nor were there any condition reports or progress requests regarding vertical ventilation (to or from the chief officers or other fire fighters) made during this incident. Information concerning the delay conducting vertical ventilation, interior conditions, roof conditions, and fire location could have been used to consider changing from a fast attack mode to a more cautious defensive operation.
Recommendation #14: Fire departments should ensure that crew integrity is maintained during fire suppression operations.
Discussion: Fire fighters should always work and remain in teams whenever they are operating in a hazardous environment.9 Team integrity means team members knowing who is on their team and who is the team leader; team members staying within visual contact at all times (if visibility is low, teams must stay within touch or voice distance of each other); team members communicating needs and observations to the team leader; and team members rotating together to rehabilitation, staging as a team, and watching out for each other (practicing a strong buddy system). Following these basic rules helps prevent serious injury or even death by providing personnel with the added safety net of fellow team members. Teams that enter a hazardous environment together should leave together to ensure that team continuity is maintained.15 In this incident, there were numerous instances where fire fighters and officers were working independently and entering and exiting the structure alone.
Recommendation #15: Fire departments should ensure that a rapid intervention crew (RIC) / rapid intervention team (RIT) is established and available to immediately respond to emergency rescue incidents.
Discussion: A rapid intervention crew (RIC) or team (RIT) should be designated and available to respond before interior attack operations begin at all fireground operations. 8, 9, 11 The team should report to the officer in command and remain at the command post until an intervention is required to rescue a fire fighter(s) or civilians. The RIC/RIT should have all tools necessary to complete the job (e.g., a search rope, first-aid kit, and a resuscitator) if a fire fighter becomes injured. Many fire fighters who die from smoke inhalation, from a flashover, or from being caught or trapped by fire actually become disoriented first. They are lost in smoke and their SCBAs run out of air, or they cannot find their way out through the smoke, become trapped, and then fire or smoke kills them. The primary contributing factor, however, is disorientation. The RIC/RIT’s only assignment should be to prepare for a rapid deployment to complete any emergency search or rescue when ordered by the IC. The RIC allows the suppression crews the opportunity to regroup and take a roll call instead of performing rescue operations. A RIC/RIT should preplan a rescue operation by finding out fire structure information (i.e., construction materials, layout, entry/egress routes, etc.), crew location and assignments, and monitoring radio traffic. When the RIC/RIT enters to perform a search and rescue, they should have full cylinders on their SCBAs and be physically prepared. When a RIC/RIT is used in an emergency situation, an additional RIC/RIT should be put into place in case an additional emergency situation arises.8
This department’s procedures designated the fourth due engine as RIC/RIT. However, the fourth due engine (Rescue 2) wasn’t prepared to engage as a RIC/RIT until several minutes after the rapid fire event occurred.
Recommendation #16: Fire departments should ensure that fire fighters wear a full array of turnout clothing and personal protective equipment that is certified by NFPA and appropriate for the assigned task while participating in fire suppression and overhaul activities.
Discussion: NFPA 1500 Standard on Fire Department Occupational Safety and Health Program, Chapter 7 contains the general recommendations for fire fighter protective clothing and protective equipment.8 Chapter 7.1.1 specifies that “the fire department shall provide each member with protective clothing and protective equipment that is designed to provide protection from the hazards to which the member is likely to be exposed and is suitable for the tasks that the member is expected to perform.” Chapter 7.1.2 states “protective clothing and protective equipment shall be used whenever the member is exposed or potentially exposed to the hazards for which it is provided.” Chapter 7.2.1 states “members who engage in or are exposed to the hazards of structural fire fighting shall be provided with and shall use a protective ensemble that shall meet the applicable requirements of NFPA 1971 Standard on Protective Ensembles for Structural Fire Fighting and Proximity Fire Fighting.” 29
At the time of this incident, the department was following a special order which did not require their members to wear the complete protective ensemble as outlined in their SOPs and required by NFPA 1971. Fire department members could choose from three options.
- Bunker coat, bunker pants, bunker boots
- Bunker coat, station pants, safety boots (Steel shank/Steel toe)
- Bunker coat, station pants, ¾ length fire boot
This special order was implemented by the fire department to assist in the health and safety of members with regards to physical stress caused by heat and limited range of motion. The fire department also did not require their members to wear flash hoods. The fire department could better provide for the health and physical safety of its members by adopting the requirements of the voluntary consensus standards pertaining to personal protective equipment, a safety and health program, and medical requirements. Recommended requirements for medical evaluations and fitness for duty for structural fire fighting can be found in NFPA 1582, Standard on Comprehensive Occupational Medical Program for Fire Departments 30 and in the International Association of Fire Fighters (IAFF)/International Association of Fire Chiefs (IAFC) Fire Service Joint Labor Management Wellness/Fitness Initiative.31 According to these recommendations, the fire department should have an officially-designated physician who is responsible for guiding, directing, and advising fire department members with regard to their health, fitness, and suitability for duty as required by NFPA 1500, Standard on Fire Department Occupational Safety and Health Program.8 Fire departments should conduct the medical evaluations annually and also develop criteria to ensure that members are physically able to safely and effectively complete the critical tasks associated with fire fighting such as wearing the full array of protective clothing.
Both victims were wearing the #2 option of bunker coat, station pants, and safety boots at the time of the fire. The bunker gear is reported by the manufacturer to meet the requirements of NFPA 1971, though it is not certified by NFPA.
It is important to note that the 2007 revision to NFPA 1982 Standard on Personal Alert Safety Systems (PASS) includes new heat and flame resistance requirements resulting from documented reports where PASS devices were not heard during fatal fireground incidents.32 Laboratory testing conducted by NIST determined that exposure to high temperature environments caused the loudness of the tested PASS alarm signal to be reduced. This reduction in loudness can cause the alarm signal to become indistinguishable from background noise at an emergency scene. Initial laboratory testing by NIST highlighted that this sound reduction may begin to occur at temperatures as low as 300°F. Thus the use of PASS devices meeting NFPA 1982, 2007 Edition requirements is highly recommended. The PPE worn by both victims were viewed by the NIOSH investigators. The PASS device worn by Victim #1 appeared to have been thermally damaged beyond working condition by the rapid fire event.
Recommendation #17: Code setting organizations and municipalities should require the use of automatic ventilation systems in commercial structures, especially ones that have large void spaces and other unique life-safety hazards.
Discussion: The use of automatic ventilation systems in roofs and enclosed void spaces that would open in the event of a fire and allow smoke, hot fire gases and heat to escape could aid fire fighters by helping control fire spread. Smoke venting through these openings would also give incident commanders and fire fighters very useful information related to the fire’s size, location and stage of growth. Many European standards such as the UK legislation requirements of BS7346 part 1 (European National (EN) 12101) & BS 5588 part 5 require automatic roof ventilation systems that automatically open to ensure rapid dispersal of smoke, heat and toxic gases.33 In this incident, the fire originated in the void space from improperly designed and installed duct work for the kitchen exhaust system. The fire suppression system for the cooking equipment did not activate when the fire started because the fire was in the void space above in the cockloft.
Recommendation #18: Code setting organizations and municipalities should require that fire alarm systems installed in commercial structures incorporate heat and smoke detectors in large void spaces to improve life-safety.
Discussion: NFPA 72, National Fire Alarm Code, paragraph 4.2 states “The purpose of fire alarm systems shall be primarily to provide notification of fire alarm, supervisory, and trouble conditions; to alert the occupants; to summon aid; and to control fire safety functions.” 34 In this case, the fire originated in the cockloft void space and was undetected by the alarm system. Code setting organizations and municipalities should require heat and smoke detectors in elevated or unusual fire hazards and life safety situations, such as the large void spaces found in taxpayers.
Recommendation #19: Code setting organizations and municipalities should require all commercial cooking operations to have periodic inspections of their kitchen exhaust systems and require all kitchen exhaust system installers to be certified to nationally recognized standards.
Discussion: The NFPA Fire Protection Handbook states “throughout history there have been building regulations for preventing fire and restricting its spread. Over the years these regulations have evolved into the codes and standards developed by committees concerned with fire protection. The requirements contained in building codes are generally based upon the known properties of materials, the hazards presented by various occupancies, and the lessons learned from previous experiences, such as fire and natural disasters.” 35 The restaurant where the incident occurred was constructed and in operation prior to the city adopting the requirements of NFPA 96, Standard for Ventilation Control and Fire Protection of Commercial Cooking Operations36 into their building codes. After the fire, it was determined that there were multiple violations regarding the installation, materials, and maintenance used in the kitchen exhaust system. Some of the materials and installation discrepancies include: improper ductwork materials, improper/inadequate ductwork connections, penetration in ductwork, inadequate clearance to combustibles, lack of access for cleaning and inspecting, and the absence of ductwork enclosures. Ductwork should be 16 or 18-gauge stainless steel to withstand the intensity of a fire and provide for corrosive protection.36, 37 The seams should be liquid tight and the duct work should have the proper clearance to combustibles or be enclosed. It should also have access points for adequate cleaning and inspecting. The ductwork in this incident was galvanized sheet metal typically used for residential heating/cooling applications. The ductwork was connected with sheet metal screws and dovetail joints associated with that type of application. It had corroded and provided a large opening for the grease from the cooking operations to exit into the cockloft area (Photo 9).
Although municipalities have adopted specific codes and standards for the design and construction of buildings, structures erected prior to the enactment of these building codes may not be compliant. Also, the building may change occupancy or complete renovations and additions that should trigger an inspection (as in this incident), 38, 39 but there weren’t any records for associated permits for this business. During the investigation, it was found that unsafe conditions and code violations had been noted before the fatal fire by city inspectors. One violation regarding housekeeping was reviewed by the NIOSH investigators. The restaurant was cited for placing aluminum foil over a food preparation table to catch smoldering grease drippings as they fell from the ceiling (Photo 10). Although the establishment had corrected all prior code violations and maintenance requirements, both the code enforcement and maintenance services failed to recognize the inadequate exhaust system installation and materials, and abatement was not required. Another way cities and municipalities may be able to monitor commercial cooking operations is to require those occupancies who have been in business prior to the adoption of nationally accepted building codes and standards to have inspections of their exhaust systems and other life-safety systems prior to renewing their license. Municipalities and code officials should use available publications such as the Kitchen Ventilation Systems and Food Service Equipment Fabrication and Installation Guidelines37 to compare and ensure that the contractors used in installing these systems are aware of proper installation requirements. Such new and improved codes and publications can provide a clear understanding and the ability to analyze the systems and installations to ensure compliance with fire and health standards and improve the safety of existing structures.36
Recommendation #20: The National Fire Protection Association (NFPA) should consider developing more comprehensive training requirements for fire behavior to be required in NFPA 1001 Standard for Fire Fighter Professional Qualifications and NFPA 1021 Standard for Fire Officer Professional Qualifications.
Structural fires frequently display indicators and warning signs of rapid fire development such as flashover, backdraft, and fire gas ignition for which many fire fighters and officers may not have been sufficiently trained to recognize or understand. It is imperative that fire fighters and officers develop the understanding and skills necessary to identify and interpret the indicators so that they can anticipate the potential for extreme fire behavior and communicate their findings to the incident commander immediately. 9, 40 This requires comprehensive training in fire behavior (theory) and practical application inclusive of realistic live fire training 9, 41, 42
NFPA 1001 Standard for Fire Fighter Professional Qualifications 12 and NFPA 1021 Standard for Fire Officer Professional Qualifications 13 were developed to ensure that fire fighters and officers have the skills necessary to perform their job. Currently these qualifications do not include the need for a sound understanding of the physical, chemical, and thermal behavior of fire and do not make a connection between fire dynamics and the influence of tactical operations (positive pressure ventilation) and external factors (wind). Standard setting agencies, states, municipalities, and authorities having jurisdiction should develop curriculum so that fire fighters and officers receive training on how to recognize and interpret fire behavior indicators and anticipate fire development. An example of a recognized course in fire behavior is the United States Fire Academy (USFA) course “Fire Behavior in a Single-Family Occupancy”. 43 The National Institute of Standards and Technology (NIST) also conducts an annual fire conference which includes seminars and presentations that cover various aspects of fire dynamics.44 These courses provide information that may lead to better tactical decision making on the fireground.
REFERENCES
- Clarke C, Zak MJ [1999]. Fatalities to law enforcement officers and firefighters, 1992-1997. Compensation and Working Conditions, 1999.
- Arocena P, Nunez I, Villanueva M [2008]. The impact of prevention measures and organizational factors on occupational injuries. Safety Science 46: 1369-1384.
- Aksom T, Hadikusumo [2008]. Critical success factors influencing safety program performance in Thai construction projects. Safety Science 46: 709-727.
- Mearns K, Whitaker SM, Flin R [2003]. Safety climate, safety management practice and safety performance in offshore environments. Safety Science 41: 641-680.
- Shannon HS, Robson LS, Sale JM [2001]. Creating safer and healthier workplaces: role of organizational factors and injury rates. American Journal of Industrial Medicine 40: 319-334.
- Vredenburgh A [2002]. Organizational safety: which management practices are most effective in reducing employee injury rates? J Safety Research 33: 259-276.
- Shannon HS, Mayr J, Haines T [1997]. Overview of the relationship between organizational and workplace factors and injury rates. Safety Science 26: 201-217.
- NFPA [2007]. NFPA 1500: Standard on Fire Department Occupational Safety and Health Program. Quincy, MA: National Fire Protection Association.
- IFSTA [2008]. Essentials of fire fighting, 5th ed. Oklahoma State University. Stillwater, OK: Fire Protection Publications, International Fire Service Training Association.
- Dodson D [2007]. Fire Department Incident Safety Officer. 2nd Edition. New York: Thomson Delmar Learning.
- NFPA [2008]. NFPA 1561 Standard on Emergency Services Incident Management System, 2008 Edition. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1001: Standard for Firefighter Professional Qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- . NFPA [2008]. NFPA 1021: Standard for Fire Officer Professional Qualifications. 2003 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1521. Standard for Fire Department Safety Officer. 2008 Edition. Quincy, MA: National Fire Protection Association.
- Dunn V [1992]. Safety and Survival on the Fireground. Saddle Brook NJ: Fire Engineering Books and Videos.
- Dunn V [2000]. Command and Control of Fires and Emergencies. Saddle Brook NJ: Fire Engineering Book and Videos.
- Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
- Dunn V [1998]. Risk management and lightweight truss construction. New York: WNYF, Official training publication of the New York City Fire Department, 1st issue.
- NIOSH [1999]. NIOSH Alert: Request for assistance in preventing injuries and deaths of fire fighters due to structural collapse. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. (NIOSH) Publication No. 99-146.
- Dunn, V. [2007]. Strategy of Firefighting. Saddlebrook NJ: Penn Well Publishing Co. p- 162.
- New York Fire Department [1993]. Taxpayer Fires. New York, NY: New York Fire Department.
- NFPA [2008]. Engine company fireground operations. Quincy, MA: National Fire Protection Association.
- Brannigan FL [1999]. Building construction for the fire service. 3rd ed. Quincy, MA: National Fire Protection Association.
- NIOSH [2005]. NIOSH alert: preventing injuries and deaths of fire fighters due to truss system failures. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. (NIOSH) Publication No. 2005-132.
- Klaene BJ and Sanders RE [2000]. Structural fire fighting. Quincy, MA: National Fire Protection Association.
- Corbin DE [2000]. Seeing is believing. Dallas, TX: Occupational Safety and Health, Aug 69(8): 60-67.
- International Fire Service Training Association (IFSTA) [2000]. Model Procedures Guide for Structural Firefighting. 2nd Edition. Stillwater, OK: Fire Protection Publications.
- Dunn, V. [1988]. Collapse of Burning Buildings: A Guide to Fireground Safety. Saddle Brook, NJ: Fire Engineering Books and Videos.
- NFPA [2007]. NFPA 1971 Standard on Protective Ensembles for Structural Fire Fighting and Proximity Fire Fighting, 2007 Edition. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1582: Standard on comprehensive occupational medical program for fire departments. Quincy, MA: National Fire Protection Association.
- IAFF, IAFC [2000]. The fire service joint labor management wellness/fitness initiative. Washington, DC: International Association of Fire Fighters, International Association of Fire Chiefs.
- NFPA [2007]. NFPA 1982 Standard on Personal Alert Safety Systems (PASS), 2007 Edition. Quincy, MA: National Fire Protection Association.
- BSRIA [2008]. New European standard for smoke extraction fans. Press Release. https://www.bsria.co.uk/services/design/mock-up-testing/test-and-certification/ Building Services Research and Information Association of Great Britain. Date accessed: Sep 2009. (Link updated 10/28/2013 – no longer available 5/13/2015)
- NFPA [2007]. NFPA 72: National fire alarm code. Quincy, MA: National Fire Protection Association.
- NFPA [1997]. Fire Protection Handbook, 18th ed. Quincy, MA: National Fire Protection Association. 1-42.
- NFPA [2008]. NFPA 96: Standard for ventilation control and fire protection of commercial cooking operations. Quincy, MA: National Fire Protection Association.
- SMACNA [2001]. Kitchen ventilation systems and food service equipment fabrication and installation guidelines. Chantilly, VA: Sheet Metal and Air Conditioning Contractors’ National Association, Inc.
- NIOSH [2005]. Career Fire Fighter Dies of Carbon Monoxide Poisoning after Becoming Lost While Searching for the Seat of a Fire in Warehouse – New York. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2004-04.
- NIOSH [2009]. Nine career Fire Fighters Die in Rapid Fire Progression at Commercial Furniture Showroom – South Carolina. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2007-18.
- Firetactics.com [2007]. Rapid fire phenomenon.pdf iconexternal icon http://www.firetactics.com/RAPID%20FIRE%20PHENOMENA%202007.pdf Date accessed: Sep 2009
- Hartin E [2005]. Why compartment fire behavior training (CFBT) is importantexternal icon. http://www.firehouse.com/article/10510694/why-is-compartment-fire-behavior-training-cfbt-important Date accessed: Sep 2009 (Link Updated 1/8/2013)
- Firetactics.com [1999]. Realistic live fire training to deal safely with flashover and backdraughtexternal icon. http://www.firetactics.com/SHAN%20RAFFEL%20IFE.htm Date accessed: Sep 2009
- USFA [2009]. Fire Behavior in a Single-Family Occupancy. http://www.usfa.dhs.gov/applications/nfacourses/catalog/details/767 Date accessed: Sep 2009 (Link Updated 1/14/2010 – no longer available 12/6/2012)
- NIST [2009]. Building and Fire Research Annual Fire Conference. http://www.bfrl.nist.gov/info/fireconf/ Date accessed: Sep 2009 (Link no longer available 12/6/2012)
INVESTIGATOR INFORMATION
This incident was investigated by Jay Tarley, Safety and Occupational Health Specialist; Matt Bowyer, General Engineer; and Tim Merinar, Safety Engineer, Division of Safety Research, NIOSH. An expert technical review was conducted by I. David Daniels, Fire Chief / Emergency Services Administrator, Renton Washington, and member of the International Association of Fire Chiefs, Executive Board of Directors.
ADDITIONAL INFORMATION
The fire department conducted a separate investigation of this incidentpdf iconexternal icon. Their investigation report is available at: http://www.cityofboston.gov/fire/pdfs/BOI_Report.pdf
FigureS









|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit the program website at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 11/03/09.