
Career Fire Fighter Dies After Roof Collapse Following Roof Ventilation - Iowa
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2002-40 Date Released: May 14, 2003
SUMMARY
On September 14, 2002, a 53-year-old male career fire fighter died after falling through a roof following roof ventilation operations at a house fire. The victim, who was not wearing a self-contained breathing apparatus (SCBA), was observing another fire fighter who was wearing an SCBA while making ventilation cuts. After making the last cut, the victim, who had been covering his face with his hands, told his partner that they had to leave immediately. The fire fighters retreated toward the aerial platform, but the victim stopped a few feet from the platform, saying he could not continue. Seconds later, the area of the roof under the victim failed, and he fell through the roof into the structure and the fire. Within minutes the interior attack crew found the victim and, with the help of the Rapid Intervention Team (RIT), removed him. He was transported to a local hospital where he was pronounced dead.
NIOSH investigators concluded that, to minimize the risk of similar incidents, fire departments should
- enforce existing standard operating procedures (SOPs) for structural fire fighting, including the use of self-contained breathing apparatus (SCBA), Incident Command System, Truck Company Operations, and Transfer of Command
- ensure that the Incident Commander evaluates resource requirements during the initial size-up and continuously evaluates the risk versus benefit when determining whether the operation will be offensive or defensive
- develop, implement and enforce SOPs regarding vertical ventilation procedures
- review dispatch/alarm response procedures with appropriate personnel to ensure that the processing of alarms is completed in a timely manner and that all appropriate units respond according to existing SOPs
- ensure that Incident Command maintains the role of director of fireground operations and does not become involved in fire-fighting efforts
- ensure that adequate numbers of staff are available to immediately respond to emergency incidents
- consider using a thermal imaging camera (TIC) as part of the exterior size-up

Incident Site
INTRODUCTION
On September 14, 2002, a 53-year-old male career fire fighter died after falling through a roof following roof ventilation operations at a house fire. On September 17, 2002, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On October 16-17, 2002, three safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated the incident. NIOSH investigators met with the Chief of the department, the International Association of Fire Fighters (IAFF) representative, and the State Fire Marshal. The NIOSH team interviewed the Chief and the fire fighters directly involved in the incident. NIOSH investigators took photographs of the incident site and reviewed the department standard operating procedures (SOPs), pictures of the incident taken by the fire department, training records of the victim, reports of the State Fire Marshal concerning the incident, and the autopsy report.
This career department has 38 uniformed personnel in two fire stations and serves a population of approximately 23,000 in an area of about 15 square miles. They respond to 15-20 structure fires per year. The department requires that new recruits complete NFPA Fire Fighter Level I training before completing probation. The victim had 27 years of experience as a career fire fighter and during this time had taken numerous training courses including Ventilation, Fire Tactics, and Live-Fires. He was certified as an NFPA Fire Fighter Level I and II. The victim had performed vertical ventilation on many structure fires prior to this incident.
Structure. The structure was a 96-year-old, 2½-story wood-frame dwelling with balloon-frame construction. The roof was steeply pitched and had intersecting gables consisting of 2- by 4-inch timbers covered with 1-inch wood planks and 4-5 layers of asphalt shingles. The building was located on a corner lot on a grade. The second floor was accessed at street level from the rear. The top floor was used for storage and was accessed via an internal stairway. No one was home at the time of the incident.
According to the State Fire Marshal’s Office and the Fire Department, the origin and cause of the fire was faulty electrical wiring in a ceiling fan between the ceiling of a second-story room and the top floor.
Apparatus. Additional units were dispatched after the fatal event; however, only those that were directly involved in the fatal event are discussed in the investigation section of this report. They are listed in order of arrival on the scene:
- Rescue Squad—1 Fire Fighter/paramedic and 1 Fire Fighter (Rapid Intervention Team [RIT])
- Engine 1—Captain (Incident Commander [IC]) and 2 Fire Fighters
- Aerial Platform Truck—Fire Fighter #1 and the victim (driver)
- Engine 2—Lieutenant and 1 Fire Fighter/Emergency Medical Technician
INVESTIGATION
On September 14, 2002, at 2230 hours, a call was received by police dispatch reporting a structure fire. At 2232 hours, the first fire department apparatus (a Rescue Squad) arrived and parked on Side D (Diagram). At 2233 hours, Engine 1 (E1) arrived and parked on Side D (a grade). Per department SOPs, the officer on E1 assumed Incident Command (IC) and reported smoke showing under the rafters. The two fire fighters from the Rescue Squad were assigned to be a RIT. Approximately 1 minute later, an Aerial Platform Truck (the victim was driving) arrived and parked on Side D behind E1. The victim and Fire Fighter #1 (FF#1) pulled hose lines from Engine 1 for the interior attack crew.
The IC and a fire fighter from E1 did an interior size-up to determine the location of the fire and if there were any occupants (there were none). Note: There was no record of a formal transfer of command during this time. Because of the heat and smoke encountered as they tried to climb to the top floor, the crew had to back down the stairs. The IC then exited the structure and called for roof ventilation. The aerial crew acknowledged the command and repositioned their truck to Side A to set up.
Engine 2 (E2) arrived at 2242 hours and parked on Side D. Note: According to witnesses and to the fire department incident report, E2 was self-dispatched and was not immediately dispatched “in accordance with existing run assignments.” A fire fighter from the Rescue Squad (one of the original RIT) replaced the IC on the second interior attack crew and a fire fighter from E2 became part of the RIT. A second interior fire attack was begun through the rear (second floor) of the building, which initially was relatively free of smoke. As this attack crew tried to climb the stairs to the top floor, they too encountered heavy smoke and extreme heat, causing them to back down the stairs to wait for ventilation.
After positioning the aerial platform over the roof reportedly “as far as it would go,” the victim and FF#1, carrying only a chain saw, exited the aerial platform and walked approximately 15 feet to the area to be ventilated. Note: FF#1 had donned his self-contained breathing apparatus (SCBA) before leaving the ground and, upon exiting the platform, went on air due to heavy smoke. Although the equipment was available on his truck, for unknown reasons the victim did not don his SCBA. At approximately 2253 hours (about 23 minutes after initial dispatch), FF#1 under direction of the victim, started cutting a hole in the roof using the chain saw. After the last cut, the victim indicated to FF#1, with some urgency, that they had to leave immediately. Note: Presumably this was due to the heavy smoke because FF#1 reported that the smoke was thick, and the victim had been covering his face with his hands while ventilation was being performed.
FF#1 quickly set down the chain saw (which fell off the roof) to help his partner. The cut section was not removed from the roof. As the two fire fighters retreated toward the platform, initially with the victim in the lead, the victim lagged behind and went down on his knees. FF#1 tried to assist the victim and encouraged him to keep moving toward the aerial platform, which was approximately 3 feet away, but the victim said he could not continue. Seconds later, the roof under the victim failed, and he fell through into the structure and the fire. Note: Videotape evidence indicates that the time that elapsed from completion of the chain saw cuts to the time at which fire self-vented out the hole through which the victim fell, was just over 1 minute. As the victim fell through the roof, flames shot up and scorched the edge of the aerial platform. At approximately 2255 hours, FF#1 started yelling something unintelligible on the radio. Approximately 1 minute later the IC and the interior attack crew realized that FF#1 was saying that the victim had fallen through (or off) the roof. FF#1 entered the aerial platform and moved it to safety.
Because the roof had self-ventilated, within 5 minutes the interior attack crew, which had remained inside the structure, was able to find the victim on the top floor and, with the help of the RIT, to remove him. The victim was carried to a waiting ambulance and transported to a local hospital where he later was pronounced dead.
The victim was on the roof for less than 7 minutes. He did not fall through the hole cut by the saw but rather through an area of the roof between the cut hole and the aerial platform. According to the Fire Department report, this area presumably failed due to direct exposure to the fire below and the weight of the victim above. The victim fell approximately 10 feet.
CAUSE OF DEATH
The cause of death per the autopsy report was smoke inhalation, intra-alveolar hemorrhage, and carbon monoxide intoxication (carboxyhemoglobin level, 30.3%).
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Fire departments should enforce existing standard operating procedures (SOPs) for structural fire fighting, including the use of self-contained breathing apparatus (SCBA), Incident Command System, Truck Company Operations, and Transfer of Command. 1–6
SCBA: According to the International Fire Service Training Association (IFSTA), “firefighters should never get on a roof wearing anything less than full protective clothing, SCBA, and a PASS device. . .” because of the possible presence of toxic products of combustion. The department in this incident has an SOP stating that SCBAs “will be worn by all personnel operating at emergency incidents above ground, below ground, or in any other area which is not, but which may become contaminated by products of combustion or other hazardous substances.” For unknown reasons, the victim was not wearing an SCBA. His partner, who survived, was wearing an SCBA and went on air before leaving the aerial platform due to heavy smoke conditions.
The victim had a carboxyhemoglobin level of 30.3%. The toxicity of carbon monoxide (CO) varies with the length of exposure, the concentration, breathing and heart rate. CO causes tissue hypoxia (low oxygen content) by preventing the blood from carrying sufficient oxygen. CO combines much more readily with the oxygen-carrying sites on the hemoglobin molecule than oxygen itself. The carboxyhemoglobin thus formed is unavailable to carry oxygen. Toxicity of CO varies with the percent carboxyhemoglobin in the blood. Reactions to CO poisoning vary with the individual and include headache, vertigo, difficulty breathing, confusion, convulsions, and coma. Carboxyhemoglobin levels greater than 55% usually are fatal; 40% levels are associated with collapse and syncope (a faint); at 15% to 25% headache and nausea may be present.
Incident Command System, Truck Company Operations: Departmental SOPs on the Incident Command System state that the IC is responsible for giving orders for incoming apparatus regarding staging locations. There is no record of the truck crew being given staging orders; however, SOPs for this department state that the truck company will “prepare to ventilate” upon arrival at a fire scene, and will “coordinate the method and timing of the ventilation/rescue with the Incident Commander.” The driver of the aerial platform truck (the victim) initially parked on a grade and, thus, was not prepared to ventilate. He later had to reposition the truck to set up, causing a delay of several minutes.
Transfer of command: NFPA 1561, §5.1.11 states that “standard operating procedures shall define the circumstances and procedures for transferring command to another on-scene officer/member and shall specify to whom command shall be transferred.” The SOP for this department states that “when transfer of command occurs, a formal declaration shall be made over the radio identifying the unit number of the new IC.” At this incident, there was no record of a formal/radio transfer of command during the time the IC was inside the structure.
Recommendation #2: Fire departments should ensure that the Incident Commander evaluates resource requirements during the initial size-up and continuously evaluates the risk versus benefit when determining whether the operation will be offensive or defensive. 7–9
Discussion: One of the most important size-up duties of the first-in officers is locating the fire and determining its severity. This information lays the foundation for the entire operation. It determines the resource requirements (number of fire fighters, amount of apparatus and equipment) needed to control the blaze, assists in determining the most effective point of fire extinguishment attack, and the most effective method of venting heat and smoke. A proper size-up begins from the moment the alarm is received, and it continues until the fire is under control. Several factors must be evaluated in conducting the size-up, for example, type of structure and construction, time of day, contents of the structure, and potential hazards.
The size-up must include continued assessment of risk versus benefit during incident operations. According to NFPA 1500 §A-6-2.1.1, “The acceptable level of risk is directly related to the potential to save lives or property. Where there is no potential to save lives, the risk to fire department members must be evaluated in proportion to the ability to save property of value. When there is no ability to save lives or property, there is no justification to expose fire department members to any avoidable risk, and defensive fire suppression operations are the appropriate strategy.” As Dunn (1992, p.291) states “When no other person’s life is in danger, the life of the firefighter has a higher priority than fire containment.”
In this incident, the building was unoccupied at the time of the incident.
Recommendation #3: Fire departments should develop, implement and enforce SOPs regarding vertical ventilation procedures. 10, 11
Discussion: The purpose of vertical ventilation is to allow the fire and its toxic gases, and heat, to escape into the atmosphere via the most direct path out of the structure. Ideally, the opening is made directly over the seat of the fire. In this incident, the ventilation opening was made several feet from the seat of the fire, and the victim fell through a weakened area in the roof between the ventilation cut and the aerial platform. At the time of this incident, the department did not have an SOP regarding vertical ventilation; however, one has subsequently been developed.
Brannigan, in Building Construction for the Fire Service (p. 180), stresses the following caution about working on roofs: “It is not safe to assume that the roof is satisfactory as a working platform until definite signs of collapse are evident. The basic assumption should be that the roof is questionable, until valid information to the contrary is determined, either from the prefire plan or fire ground observation . . . While time-to-failure cannot be accurately predicted, the time the structure has been burning must figure in the fire ground commander’s thinking . . . Once the structure itself is involved in the fire, it is deteriorating in an unknown manner and rate.”
SOPs should include health and safety considerations such as the need for personal protective equipment, as well as procedures for reading a roof and determining where to locate the ventilation opening. IFSTA lists a number of factors that the officer in charge should consider when choosing a site for ventilation, including the following:
- The seat of the fire
- Roof construction type and condition
- Continuous observation of the roof
- Charged attack and protection lines ready
- Wind direction and intensity
- Coordination with attack companies
- Keeping track of elapsed time into the incident
Recommendation #4: Fire departments should review dispatch/alarm response procedures with appropriate personnel to ensure that the processing of alarms is completed in a timely manner and that all appropriate units respond according to existing SOPs. 6, 12
Discussion: NFPA 1221 §6.3.1 states “the authority having jurisdiction shall ensure that the number of telecommunicators needed to effect the prompt receipt and processing of alarms shall meet the requirements of Section 6.4.” Section 6.4.2 states “ninety-five percent of alarms shall be answered within 15 seconds, and 99 percent of alarms shall be answered within 40 seconds.” Section 6.4.3 states “ninety-five percent of emergency dispatching shall be completed within 60 seconds.” Section 6.4.5 states “where alarms are transferred from the public safety answering point (PSAP), the transfer procedure shall not exceed 30 seconds for 95 percent of all alarms processed.” Section 6.4.6 states “in cases where the communications center is not the primary answering agency . . . for alarms, the answering agency shall transfer alarms as follows: (1) the alarm shall be transferred directly to the telecommunicator; (2) the answering agency shall remain on the line until it is certain that the transfer is effected; and (3) the transfer procedure shall be used instead of relaying the information to the communications center.” According to the departmental SOP regarding Alarm Responses, because this was a structure fire, it required a “full response” which included Engine 2 (Station 2). Engine 2 was not immediately dispatched in accordance with existing run assignments. The original emergency call, which came in through police dispatch, was not transmitted to Station #2. Station #2 personnel heard radio traffic about the fire and self-dispatched, causing a delay in arrival (Engine 2 arrived approximately 9 minutes after Engine 1). Since this incident, the fire department has had discussions with the authority having jurisdiction over telecommunicators. As a result of these discussions, run assignment charts for dispatchers have been reformatted. The new charts indicate the stations that need to be notified, as opposed to particular pieces of apparatus.
Recommendation #5: Fire departments should ensure that Incident Command maintains the role of director of fireground operations and does not become involved in fire-fighting efforts. 4, 13
Discussion: According to NFPA 1561, §4.1.1, “the Incident Commander shall be responsible for the overall coordination and direction of all activities at an incident.” In addition to conducting an initial size-up, Incident Command must maintain a command post outside of the structure to assign companies and delegate functions, and continually evaluate the risk versus gain of continued fire fighting efforts. To effectively coordinate and direct fire-fighting operations on the scene, it is essential that adequate staff are available for immediate response to ensure that the Incident Commander is not required to become involved in fire-fighting efforts.
Recommendation #6: Fire departments should ensure that adequate numbers of staff are available to immediately respond to emergency incidents. They should consider doing only defensive operations until sufficient resources are on the scene. 14, 15
Discussion: For “low-hazard occupancies” (e.g., 1-, 2-, or 3- family dwellings), the NFPA recommends the following initial attack response: “At least two pumpers, 1 ladder truck (or combination apparatus with equivalent capabilities), 1 chief officer, and other specialized apparatus as may be needed or available; not fewer than 12 fire fighters and 1 chief officer (p. 10-34).”
NFPA 1710 § 5.2.2 recommends that a minimum acceptable fire company staffing level should be four members responding on or arriving with each engine and each ladder company responding to this type of low-hazard fire. NFPA 1710 §5.2.1.1 states the following: “On-duty fire suppression personnel shall be comprised of the numbers necessary for fire-fighting performance relative to the expected fire-fighting conditions. These numbers shall be determined through task analyses that take the following factors into consideration:
- Life hazard to the populace protected
- Provisions of safe and effective fire-fighting performance conditions for the fire fighters
- Potential property loss
- Nature, configuration, hazards, and internal protection of the properties involved
- Types of fireground tactics and evolutions employed as standard procedure, type of apparatus used, and results expected to be obtained at the fire scene.”
Recommendation #7: Fire departments should consider using a thermal imaging camera (TIC) as part of the exterior size-up. 16
Discussion: In recent years, thermal imaging cameras (TICs) are used more frequently by the fire service for exterior size-up to locate the source as well as the hottest part of the fire and for search and rescue to locate victims. This knowledge, in turn, may help fire fighters determine the safest approach and areas of the structure to avoid. Ceilings and floors, for example, that have become weakened by fire and are threatening to collapse may be spotted with a TIC. In this incident, the exact location of the fire on the top floor was unknown. A TIC could possibly have been used to identify the seat of the fire and, thus, the optimal area for vertical ventilation.
REFERENCES
- International Fire Service Training Association [2002]. Fireground support operations. 4th ed. Stillwater, OK: Fire Protection Publications.
- Proctor & Hughes [1996]. Chemical hazards of the workplace. 4th ed. New York: Van Nostrand Reinhold.
- Merck Research Laboratories [1999]. The Merck manual of diagnosis and therapy. 7th ed. Whitehouse Station, NJ: Merck Research Laboratories.
- NFPA [ 1995]. NFPA 1561: standard on fire department incident management system. Quincy, MA: National Fire Protection Association.
- Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
- Iowa Fire Department [2002]. Written standard operating procedures.
- Dunn V [1992]. Safety and survival on the fireground. Saddlebrook, NJ: Fire Engineering Books & Videos.
- Foley SN [1998]. NFPA 1500: fire department occupational health and safety standards handbook. 1st ed. Quincy, MA: National Fire Protection Association.
- Klaene BJ, & Sanders RE [2000]. Structural fire fighting. Quincy, MA: National Fire Protection Association.
- IFSTA [1994]. Fire service ventilation. 7th ed. Stillwater, OK: Oklahoma State University.
- Brannigan FL [199]. Building construction for the fire service. 3rd ed. Quincy, MA: National Fire Protection Association.
- NFPA [1999]. NFPA 1221, standard for the installation, maintenance, and use of emergency services communications systems. Quincy, MA: National Fire Protection Association.
- Page JO [1973]. Effective company command for company officers in the professional fire service. Alhambra, CA: Borden Publishing Co.
- NFPA [2001]. NFPA 1710: standard for the organization and deployment of fire suppression operations, emergency medical operations, and special operations to the public by career fire departments. Quincy, MA: National Fire Protection Association.
- NFPA [1997]. Fire protection handbook. 18th ed. Quincy, MA: National Fire Protection Association.
- Corbin DE [2000]. Seeing is believing. Occupational Health & Safety. August issue.
INVESTIGATOR INFORMATION
This incident was investigated by Jay Tarley, Linda Frederick and Steve Berardinelli, Safety and Occupational Health Specialists, NIOSH, Division of Safety Research, Surveillance and Field Investigation Branch.
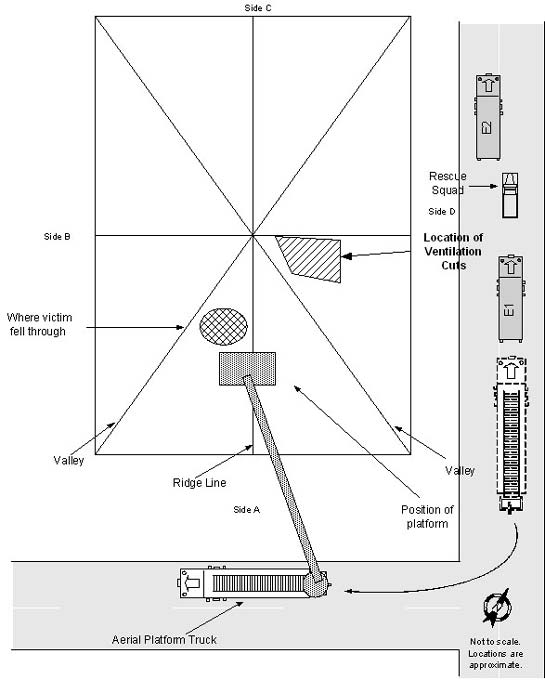
Diagram. View of roof and aerial platform from above
This page was last updated on 05/14/03