
Tree Feller Dies After Being Struck by Snag While Felling Tree in West Virginia
Investigation #99WV038
Release Date: November 12, 1999
SUMMARY
On July 6, 1999, a 46-year-old male tree feller (the victim) died of injuries sustained when he was struck in the head and back by a 63-foot snag which had been lodged in two trees. The crew had discussed removing the snag which rested in a tree above the skid road and was in contact with a tree below the road. Although company policy called for mechanical removal of all snags, the victim attempted to knock the snag out of the tree by felling another tree into it. Instead of breaking the snag loose, the tree fell in the wrong direction, lodging in one of the two trees which was in contact with the snag. The lodged tree was removed from the area with a bulldozer, yet the snag was left unmoved. The following day, the owner advised the victim to wait until the snag was mechanically removed before cutting in the area. The victim made the decision to fell the tree below the skid road whose top was in contact with the snag. Placing himself under the snag, the victim began cutting the tree. The company owner and the loader operator were at the landing site conversing with the landowner. The landing site was approximately 75 yards from the victim’s worksite. The company owner suddenly heard the chainsaw stop running and headed for the work site with a gasoline can. When he arrived at the scene, he saw that the snag had crushed the victim, killing him instantly. The chainsaw was still stuck in the tree as the tree remained standing. He yelled back to the landing for someone to contact 911. The landowner went to his home, located nearby, and called 911. The EMS arrived approximately one hour later and transported the victim to a local trauma center where he was pronounced dead on arrival.
The WV FACE Investigator concluded that, to reduce the likelihood of similar occurrences, employers should:
- ensure that any snag, in or near an active cutting zone, be identified, tagged/flagged, and removed mechanically before proceeding with the cutting operation.
- ensure that tree fellers properly evaluate the timber and the area around the timber to be felled immediately prior to felling so that potential hazards can be identified and appropriate control measures implemented.
- ensure that company safety programs are consistently implemented and enforced including those methods for dealing with worker non-compliance.
INTRODUCTION
On July 6, 1999, a 46-year-old male timber cutter (the victim) died of injuries sustained when he was struck in the head and back by a dead snag while felling a tree. On July 16, 1999, the WV FACE Investigator was notified via a newspaper clipping service. On October 13, 1999, the WV FACE Investigator conducted an on-site investigation. The Investigator reviewed the incident with a West Virginia Division of Forestry Representative, who then accompanied the Investigator to the site. The landowner was also interviewed. The incident site was examined and photographed. Other informational sources and contacts included death certificate, newspaper articles, West Virginia Division of Forestry, and OSHA investigation reports.
The employer in this incident was a commercial logging company that had been in business for 6-8 years. Three crew members, including the company owner, were present the day of the incident. The landowner was also on the premises throughout the morning. The marked timber on this 32-acre tract was being selectively harvested for saw timber. The operation began June 5 and was reported to be on schedule.
The company owner and the tree feller (the victim) had both undergone logger recertification in March 1999. [Note: The Logging Sediment Control Act of West Virginia (1992) requires that each timbering operation in West Virginia be supervised by a certified logger. To become a certified logger, an individual is required to successfully complete training and pass a test for best management practices (a soil erosion prevention plan) and chainsaw safety and possess a current first aid card.1]
The company has a written safety program, which includes a copy of logging regulations. Weekly safety meetings were held, and snag hazard identification and elimination were also discussed. The company policy required that snags be removed mechanically. The employer provided his employees with personal protective equipment. It was reported that the victim was wearing safety glasses, a hardhat, and hearing protection at the time of the incident. It was reported that the victim refused to wear certain types of PPE, such as chaps. It was also reported that the victim used non-directional felling techniques in spite of the owner’s request to cease such practices.
The victim was a certified logger and had attended the West Virginia Division of Forestry’s chainsaw safety workshop only three months before the incident. The victim had been felling trees for about 2-3 hours prior to the incident.
INVESTIGATION
On July 6, 1999, the company was selectively harvesting the tract and had begun work at approximately 7:00 a.m. It was reported to be a hot and dry day in the area. The victim and two other workers were present that day. They were working in an area that had some dead snags; they had unsuccessfully tried to remove one snag the previous day by felling another tree into it. The tree fell in the wrong direction and lodged in another tree (the same one in which the snag was lodged). The lodged tree was removed from the area with a bulldozer, yet the snag was left unmoved. The following day, the owner advised the victim to wait until the snag was mechanically removed before cutting in the area. That morning (July 6), at approximately 10 a.m., the victim was felling a scarlet oak on the lower side of the skid road. The victim made the decision to fell the tree below the skid road whose top was in contact with the snag. Placing himself under the snag, the victim began cutting the tree. It is uncertain whether the snag was resting in the tree that was being cut by the feller or if it was only in contact with it. The butt of a snag was resting on the slope above the road and extended approximately 62 feet. It rested in a tree above the skid road and was towering above the road and over the victim’s cutting position (see Figure 1). The company owner and the loader operator were at the landing site conversing with the landowner. The landing site was approximately 75 yards from the victim’s worksite. The company owner suddenly heard the chainsaw stop running and headed for the work site with a gasoline can. When he arrived at the scene, he saw that the victim had been crushed by the snag, killing him instantly. The chainsaw was still stuck in the tree as the tree remained standing with only partial felling cuts completed. He yelled back to the landing for someone to contact 911. The landowner went to his home, located nearby, and called 911. The EMS arrived approximately one hour later and transported the victim to a local trauma center where he was pronounced dead on arrival.
CAUSE OF DEATH
The medical examiner’s report listed the immediate cause of death as a severe crushing head injury.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that any snag, in or near an active cutting zone, be identified, tagged/flagged, and removed mechanically before proceeding with the cutting operation.
Discussion: The worksite in this incident had several dead snags. The tree being felled was located close to the deadly snag and possibly connected to it. The snag involved in the incident was identified and discussed the previous day but was not marked tagged/flagged or immediately removed. Snags should be mechanically removed as soon as possible after being identified. Where immediate removal is not feasible, tagging/flagging will alert workers to maintain a two-tree length safety buffer until mechanical removal is possible. OSHA Regulation 29 CFR 1910.266 (h)(1)(vi) requires that each danger tree, including snags and lodged trees, shall be felled, removed, or marked and avoided. Removal using mechanical or other techniques that minimize the logger’s exposure to the potential risk should have been utilized in this incident; the victim was working well within the danger zone. In fact, he had positioned himself directly beneath the snag while felling. Had the snag been removed the previous day or had the snag been flagged and the required buffer zone maintained, this incident might have been prevented.
Recommendation #2: Employers should ensure that tree fellers properly evaluate the timber and the area around the timber to be felled immediately prior to felling so that potential hazards can be identified and appropriate control measures implemented.
Discussion: A large snag was resting in or near the tree that the feller had selected to cut. OSHA Regulation 29 CFR 1910.266 (h)(2)(ii) requires that, before each tree is felled, conditions, such as, but not limited to, snow and ice accumulation, the wind, the lean of the tree, dead limbs, and location of other trees, shall be evaluated by the feller and precautions taken so a hazard is not created. In this case, evaluations were made the previous day but abatement of the identified problem was not. It is possible that the victim failed to reevaluate the situation just prior to cutting since it had been looked at the day before. Having taken a second look at the situation may have given the victim a better understanding of the relationship between the deadly snag and its supporting members.
Recommendation #3: Employers should ensure that company safety programs are consistently implemented and enforced including methods for dealing with worker non-compliance.
Discussion: The evaluation of tasks to be performed at the work site form the basis for the development, implementation, and enforcement of a safety program. The key elements for this program should include, at a minimum, training in hazard identification and the avoidance and abatement of these hazards. Additionally, the program should address the steps to be taken in the event of identifying a worker who fails to follow company-established safe work practices. In this incident, the victim was fatally injured when he was working in a company-identified unsafe area. The owner advised the victim to wait until the snag was mechanically removed before cutting in the area. The victim made the decision to fell the tree below the skid road whose top was in contact with the snag. Additionally, it was reported that the victim refused to wear certain types of PPE, such as chaps, and that the victim used non-directional felling techniques in spite of the owner’s request to cease such practices. The above worker behavior indicates that the enforcement component of the company’s safety program was inadequate. Having enforced the safety program concerning all matters may have given the victim the incentive to follow the company’s directives concerning the deadly snag.
REFERENCES
- West Virginia Logging Sediment Control Act, 1992.
- Office of the Federal Register, Vol. 59, No. 196, 29 CFR 1910.266.
ILLUSTRATIONS:
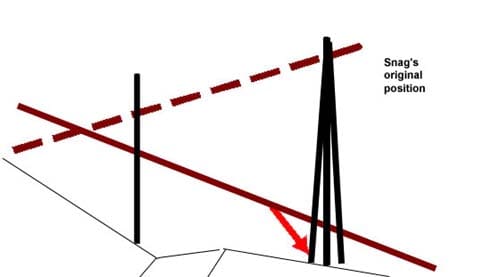
Figure 1. The red arrow indicates the position of the victim when felling.

Figure 2. The flag represents the approximate location of the victim’s head after being struck by the snag.

Figure 3. This is a view of the snag from the victim’s perspective.
The section which struck the victim was 12 inches in diameter.
Note: Snag has been moved and bucked prior to photograph.
FATALITY ASSESSMENT AND CONTROL EVALUATION PROGRAM
The WVU Center for Rural Emergency Medicine, through a contract with the West Virginia Department of Health and Human Resources, conducts investigations on the causes of work-related fatalities within the state. The goal of this program is to prevent future fatal work-place injuries. West Virginia FACE intends to achieve this goal by identifying and studying the risk factors that contribute to work-place fatalities, by recommending intervention strategies, and by disseminating prevention information to employers, employees, trade associations, unions, equipment manufacturers, students, teachers, and others with an interest in work-place safety.
Please use information listed on the Contact Sheet on the NIOSH FACE website to contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.