
A module truck driver for a cotton gin in Texas died from internal injuries when crushed between the tailgate of a trailer and the metal beam supporting a cotton seed dispenser box
Investigation # 99TX38101
Release Date: January 18, 2001
SUMMARY
On October 12, 1999 a 35 year-old module truck driver for a cotton gin in Texas suffered fatal injuries when he was caught between a semi-truck/trailer tailgate and the lower supportive metal beam of a seed dispenser box unit. The victim had climbed up on the ladder attached to the rear gate of the trailer to motion with his left hand in guiding the truck driver. While the truck was backing up, the victim’s back struck the metal lower beam of the frame supporting the seed box dispenser unit. He was forced frontwards over the tailgate and fell into the bed of the trailer. EMS was called and he was transported to a regional hospital for treatment. He died of a severe internal infection from a torn/ruptured colon 15 days later.
The Texas FACE program officer concluded that to reduce the likelihood of similar occurrences, employers should:
- Ensure employees who are guiding trucks are on the ground and always visible to the driver
- Ensure employees do not climb onto moving trailers
- Redesign the driveway to eliminate the need for trucks to back up
- Install grooved and lowered tire paths for ease of tire alignment
- Install an electric eye mechanism onto the seed dispenser frame which provides oral and visual position warnings for truck drivers
- Provide regular training for seasonal workers on safety standards and procedures
INTRODUCTION
On October 12, 1999 a 35 year-old module truck driver (the victim) who worked for a cotton ginning crew died from injuries when he struck the framework of a cotton seed dispenser box unit, was forced over the tailgate of a semi-truck/trailer and fell into the bed of the trailer. The OSHA regional office notified the Texas FACE program officer of this incident on November 12, 1999. The Texas FACE program officer visited the site on November 22, 1999, where she interviewed the manager and an assistant at the cotton gin and took pictures of the dispenser and similar truck/trailer units.
The cotton gin had been in business for 25 years. It was a seasonal business running from about mid-October to mid-December or 10 to12 weeks. Work was conducted on a 24 hour basis with two 12 hour shifts having usually nine employees on each shift. The number of employees depended on how much cotton needed to be processed.
The cotton gin employed one other module truck driver. (A module truck is specifically built to pick up and haul the 20,000 lb. cotton modules or boxes from a farmer’s field to the cotton gin.) The victim was raised in the geographical area and had worked at this gin in past years (1990 and 1991). He was familiar with the ginning process and was an experienced mechanic, who worked on the trucks and repaired gin equipment before the season started. When he was fatally injured, he had worked at the gin for 2&frac;12 weeks.
The employer’s safety policy consisted of written general rules which employees were required to read and sign acknowledging their understanding and adherence. Only persons experienced in the ginning process were hired. New employee safety training would begin a day or two after employees began working and would consist of a meeting and walk-around with the manager of the gin who reviewed the procedures and the operation of the equipment. As safety issues arose during the season, employees and management would informally discuss them. The employer provided hard hats, dust masks, and earplugs to the employees. The employer did not conduct pre-employment physical exams or drug screening. Employees determined to be working under the influence of drugs or alcohol were terminated.
The manager stated that in the last 4 years they have had more injuries and incidents than in the previous 21 years. They had four minor injuries in the last four years. It was conjectured that the reason for the increased injury rate was due to having to hire employees not necessarily familiar with gin operations. This unfamiliarity increases injury exposure and should demand more training for new employees.
INVESTIGATION
The employer, an operator of a cotton gin in Texas, had just started its seasonal operations which usually ran for 10 to 12 weeks from mid-October to mid-December. Employees were processing their third load of cotton for the season on the day of the incident. There were six employees (out of the regular crew of nine) on duty during this shift because the amount of cotton did not justify having a full crew. Ginning was a daily 24-hour operation and there were two 12-hour shifts of workers. The incident occurred during the day shift.
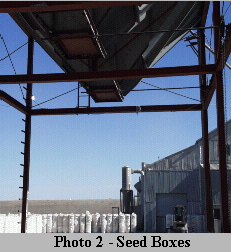

Employees were preparing to dispense a small quantity of seed after the cotton fiber had been processed and baled. The seed was mechanically conveyed to the cotton seed dispenser box unit situated outside the gin. The unit consisted of three metal boxes positioned on a metal frame 37 feet in length, 18 feet wide and13 feet 9 inches high to the lower metal beam (see Photo 1). The cotton seed boxes had a funnel bottom with a door controlled by a chain to open and let the seed flow out into the trucks’ trailers (see Photo 2). Semi-trucks with trailers (see Photo 3) would back up and position their trailers under the boxes and normally have the seed deposited in the front end of the trailer first (next to the cab). As the semi-truck traveled slowly forward, the seed would be deposited evenly in the rest of the trailer.

The height of the lower beam of the seed dispenser metal frame was 13 feet 9 inches from the ground. The gin management preferred no trucks over 13 feet high to back under the dispenser. It was possible that a 13 foot 6 inch truck could get under the beams if tire pressure was decreased to lower the unit. Also, if a raised tarp was on the trailer, it could be lowered or removed. The trailers had a ladder on the tailgate so individuals could climb up to adjust the tarp (see Photo #3).
Trucks would pull out in front of the seed dispenser and then back up under the boxes. It was sometimes necessary to have someone help the drivers maneuver under the box frame by motioning them back. The standard procedure was to have a person stand on the ground next to the seed box dispenser and use their hands to signal to the driver.
On the day of the incident a 13 foot 6 inch truck came in for seed. The driver decreased the pressure in the tires and lowered the tarp on the trailer to effectively adjust the height to no more than 13 feet. The manager told the victim to go out to help the driver back in. That way they would make sure that the trailer fit under the dispenser. He would also be able to show the driver how to operate the doors on the seed boxes.
The victim was with the other module driver. They agreed that the other module driver would go ahead and unload a module while the victim assisted the semi-truck driver. At about 3:45 PM, for some unknown reason, the victim climbed up on the left rear ladder of the trailer and started motioning with his left hand to the driver to back up. The driver said that the victim stopped waving his hand so he went back to the rear of the trailer about five minutes after the waving stopped to see what had happened. When he reached the back of the trailer, the driver heard a noise inside. He climbed up the ladder and peered down into the trailer. He heard the victim groaning and saw him lying on the floor of the trailer on some cotton seed that had been dumped in earlier. The driver got down off the trailer and started running towards the gin office when he saw a gin employee and the victim’s father. He told them that the victim was hurt and lying in the bed of the trailer. The gin employee and the victim’s father ran to the semi-truck and climbed up the ladder and jumped into the trailer. A minute later, the gin manager drove his truck around the building to see how loading the truck was progressing. The driver stopped him to tell him what had happened.
There were no witnesses to the incident itself. The account of the fatality is based on the victim’s statements, injuries received, and the position of the semi-truck and trailer. Apparently, the victim was concentrating on guiding the trailer back under the seed boxes and was looking straight ahead when his back came into contact with the lower metal beam of the seed box dispenser unit. His body’s position was about belly high with the top of the trailer gate. The beam pinched him between the trailer and the beam at the top of his back with his stomach pushed over the trailer’s rear sideboards. The force flipped him into the trailer and he fell down about eight feet onto the small load of cotton seed inside the trailer.
The victim’s father and the gin manager held the victim steady so his weight did not shift on the cotton seed already in the trailer to keep from aggravating any possible injuries. The victim told them that he had a lot of pain in his chest, abdomen, and pelvic areas. The doors to the trailer were kept closed to contain the cotton seed and to keep conditions stable.
The co-worker ran to a telephone and called 911. EMS arrived within 10 minutes at 2:53 PM. The EMS crew determined how to remove the victim from the trailer so as not to cause further harm. They opened the doors to the trailer while the victim was held steady. Some of the cotton seed was scooped out so they could get a spine board under the victim. To keep him immobilized, it took six adults to move the victim on the spine board from the trailer to the EMS cot. He was transported to the area hospital with preliminary findings of several broken vertebrae in the lower back. He became very ill two days later. Doctors conducted exploratory surgery due to signs of internal distress. Surgery revealed a ruptured/torn colon with a 6 inch gap. The doctors could not determine if the colon was severed or if it exploded from the pressure of the beam and trailer sideboards. Death came 13 days later due to a severe infection from the contents of the torn colon.
CAUSE OF DEATH
The medical examiner determined the cause of death was a ruptured/torn colon as the result of an accident.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Ensure employees who are guiding trucks are on the ground and are always visible to the driver.
Discussion: Make it standard operating procedure that all truck drivers maintain visual contact with the gin employee guiding the truck and that the guiding employee is standing on the ground. There should be no truck movement unless the guiding employee is standing on the ground and can be seen by the driver.
Recommendation #2: Ensure employees do not climb onto moving trailers
Discussion: It is not known why the victim got up on the ladder of the trailer versus following standard procedure (standing on the ground in view of the driver through the side mirror). To prevent future incidents of this sort, it should be mandatory that employees do not climb on trailers.
Recommendation #3: Redesign driveway to eliminate need for trucks to back up
Discussion: Truck drivers should drive forward instead of backing under the seed dispenser unit and stop at designated markers to have the seed dumped into their trailers. This would eliminate the need for an employee to guide the drivers. A circular drive under the dispenser unit would be ideal. Visual markers could be installed to indicate if and when the driver should proceed.
Recommendation #4: Install grooved and lowered tire paths for ease of tire alignment
Discussion: If altering the driveway is not possible, grooves could be dug in the ground under the dispenser for drivers to back into to align their tires properly. Visual markers could be installed to indicate if and when the driver should proceed.
Recommendation #5: Install a photo cell device onto the dispenser frame which provides oral and visual position warnings for the truck drivers
Discussion: The need to have an employee guide the truck drivers could be eliminated through the installation of an electric eye mechanism on the frame of the seed dispenser. When the truck was in a specific location, the electric eye would detect the object and the circuit would be broken to sound a signal or produce a flashing light. Dealers of industrial controls supply such devices.
Recommendation #6: Provide regular training for seasonal workers on safety standards and procedures.
Discussion: Seasonal employees should receive training on safe work techniques and procedures before they begin work each year and refresher training provided regularly during the season. It is time and money well spent for employers to train and retrain employees in the proper performance of a task or job. Even experienced employees benefit from reviewing routine and nonroutine procedures. Providing safety information will convince employees that management is serious about safety and is sincerely interested in preventing accidents. Training is best provided in a group setting so all employees can benefit from the discussion. Although it is good practice to provide written safety instructions, it is difficult to ensure that they are read and understood. This necessitates constant communication between supervisors and staff on safety issues.
Please use information listed on the Contact Sheet on the NIOSH FACE web site to contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
Back to NIOSH FACE Web