
A Press Brake Operator Died When He Was Struck by a Steel Lug
Oklahoma Case Report: 05-OK-005-01
Summary
A 39-year-old press brake operator died on January 24, 2005 from head and chest trauma he received after being struck by a steel lug (sheet of steel) that ejected from the machinery he was operating. Prior to the incident, the victim was using the press brake to finish curving the 920-pound steel lug. While the victim was applying pressure two to three inches from the edge of the lug, the lug edge slipped off the back of the V-shaped bottom die and was ejected from the press brake. The lug struck the victim in the head with one end of the lug coming to rest on the floor and the other end on the forks of a nearby forklift. The victim’s right arm was pinned between the fork and the lug. A coworker who was assisting the victim called for help and several employees were able to lift the lug and free the victim. The victim was transported to the hospital where he was pronounced dead in the emergency room.
Oklahoma Fatality Assessment and Control Evaluation (OKFACE) investigators concluded that to help prevent similar occurrences, employers should:
- Ensure that all machines have guarding in the form of physical barriers or adequate distance to protect employees from hazards.
- Ensure that machine operators are trained in recognizing and controlling hazards associated with their machine’s operation.
- Develop, implement, and enforce a comprehensive safety and health program that includes training based on written task-specific and machine-specific safe operating procedures.

|
|
Figure 1. Press brake involved in the incident.
|
Introduction
A press brake operator for a metal fabrication facility died on January 24, 2005 from head and chest trauma received when he was struck by ejected steel material. OKFACE investigators were notified of the incident and an interview with company officials was conducted on June 9, 2005. OKFACE investigators also reviewed the death certificate and reports from the Medical Examiner and the Occupational Health and Safety Administration (OSHA).
Employer: The victim was employed at a metal fabrication company that primarily worked on small to medium quantity runs of custom order metal parts. The company had been in business for 28 years and employed approximately 100 full-time employees. The company had a written safety and health program, but no management safety committee. Although, the company had five medium to large press brakes in operation, no written machine-specific safe operating procedures existed. The company required certification for forklift operators, but did not require machine operators to be licensed or tested for proficiency.
Victim: The 39-year-old male victim had been working for the metal fabrication company for one year and five months. He was operating a press brake and was considered an experienced operator. At the time of the incident, the victim was performing a task that was part of his normal job duties and was wearing the required personal protective equipment, including safety glasses and steel-toed shoes.
Training: Safety meetings were conducted monthly and toolbox safety meetings were held as new hazards were recognized. The company and machinery manufacturer conducted machine-specific training, utilizing equipment manuals, videos, classroom training, and on-the-job mentoring. Written task-specific safe work procedures existed, but task-specific training was not conducted. The company documented all employee training and maintained records on file.
Incident Scene: The incident occurred in the work area of a press brake machine. There was ample space for maneuvering equipment and personnel in the area. Lighting was adequate and the concrete floor was smooth and dry. The victim started his shift at 6:00 a.m. and the incident occurred at approximately 4:00 p.m.
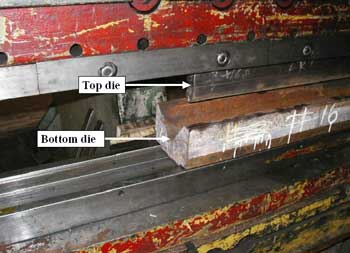
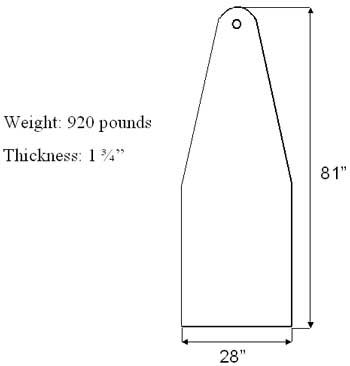
Equipment: The press brake used during the incident (Figure 1) was a piece of heavy machinery that could apply 1,250 tons of force along the 22-foot long top and bottom dies (Figure 2) that formed the machine’s point of operation. A die is a device used for cutting, forming, or stamping material during pressing operations. The control panel to the press brake was located at a safe distance from the point of operation of the machine; however, the foot actuator was on a flexible cord and could be positioned anywhere in front of the machine. The press brake was equipped with an emergency shut-off device and several signs were posted warning of the dangers of putting hands into the point of operation. However, it was not equipped with point of operation guards. Only one of the five press brakes in operation had any point of operation guarding (a safety curtain). The steel lug involved in the incident (Figure 3) was 81 inches long, 28 inches wide, 13/4 inches thick, and weighed 920 pounds.
Weather Condition: Weather was not a factor in the incident as the machine was located in a climate-controlled environment.
|
|
Figure 2. Top and bottom dies of press brake.
|
Investigation
On the day of the incident, the victim and a coworker were in the process of bending a radius into a steel lug. The victim’s coworker had positioned a forklift carrying the lug directly in front of the press brake. Due to the large size of the lug, it had to be supported on the forks of the forklift while the bending process was performed. In order to form the required radius, a series of several small bends had to be made.
With the forklift and lug ready, the victim approached the front of the press brake and aligned the lug with the bottom die. The plan was to apply pressure to the lug two to three inches from the edge. While standing next to the forklift, lug, and press brake point of operation, the victim used the foot actuator to engage the press brake. As the press brake began to apply pressure to the edge of the lug, the material slipped off the back edge of the V-shaped bottom die and was ejected from the press brake.
The coworker was positioned in the operator’s seat of the forklift at the time of the incident and did not see the victim being struck by the ejected lug. Immediately after the ejection of the lug, the coworker called the victim’s name three times, each with no response. The coworker dismounted the forklift and immediately yelled for someone to call 911. The victim was struck on the top of the head and as he fell, his chin hit the forklift. The wide end of the lug came to rest on the floor, while the narrow end came to rest on the forks, pinning the victim’s right arm. Three coworkers arrived at the scene almost immediately and manually lifted the steel lug off the victim’s arm. Within approximately two minutes of the incident, three additional coworkers equipped with a trauma kit began monitoring the victim’s pulse and respiration, while others secured the site by removing the lug with an overhead crane. Emergency medical services arrived on the scene and transported the victim to the hospital where he was pronounced dead in the emergency room.
|
|
Figure 3. Sketch and measurements of lug involved in the incident.
|
Cause of Death
The Medical Examiner’s report listed the cause of death as blunt force trauma of the head and chest.
Back to Top
Recommendations/Discussion
Recommendation # 1: Employers should ensure that all machines have guarding in the form of physical barriers or adequate distance to protect employees from hazards.
Discussion: Engineering controls in the form of machine guarding (e.g., fixed, adjustable, and self-adjusting guards) should be used to minimize operators’ exposure to physical hazards. During some manufacturing processes and when physical guarding is not practical, guarding by a safe distance (i.e., positioning all controls away from the point of operation) may be acceptable. Guarding by safe distance is acceptable when the employer can demonstrate that physical barriers are not feasible to guard the point of operation. When an employer adopts guarding by safe distance, the employer should have an effective program in place. An effective program should contain exposure prevention procedures, training, and measures of effectiveness of training, retraining, supervision, and periodic inspection.
According to OSHA standards, one or more methods of machine guarding should be provided to protect the operator and other employees in the machine area from hazards such as those created by point of operation, ingoing nip points, rotating parts, and flying chips and sparks. The National Safety Council recommends guarding where the machine contacts the material, part, or stock and performs operations such as cutting, punching, grinding, boring, forming, or assembling. Also, guarding should be considered near power transmission components, including flywheels, pulleys, belts, connecting rods, cams, spindles, chains, sprockets, clutches, feed rolls, cranks, gears, and robots.
Recommendation #2: Employers should ensure that machine operators are trained in recognizing and controlling hazards associated with their machine’s operation.
Discussion: Employees should be trained to recognize hazards that pose a risk to themselves or other workers. Manuals from the manufacturer are good sources of safety-related information on potential hazards. Written safety and health policies should encourage employees to report hazards and make suggestions related to safety. As in this incident, ejection of materials from a machine’s point of operation may be more likely when high pressure is applied to the edge of inadequately secured material. Heavy materials that are ejected from machinery may fall, causing injury or property damage and smaller lightweight materials may become projectiles.
Recommendation #3: Employers should develop, implement, and enforce a comprehensive safety and health program that includes training based on written task-specific and machine-specific safe operating procedures.
Discussion: Employers should develop a comprehensive, written safety program that incorporates guidelines for operating machinery and performing tasks. Employees should be given a copy of the program and provided training that emphasizes safe operating procedures, limitations of equipment, use of guards, and hazard recognition and control. Employers should monitor employee compliance with all policies and procedures and refresher training should be conducted as needed. Training should be completed before the employee/operator is allowed to work near equipment and the employer should maintain records of all training.
References
- Occupational Safety and Health Administration, 29 CFR 1910.211-219, Subpart O, Machinery and Machine Guarding.
- Occupational Safety and Health Administration, Directive Number: CPL 02-01-025, February 14, 1997, Guidelines for Point of Operation of Power Press Brakes.
- Occupational Safety and Health Administration, OSHA Publication 3170, 2001, Safeguarding Equipment and Protecting Workers from Amputations.
- Occupational Safety and Health Administration, OSHA Publication 3067, 1992, Concepts and Techniques of Machine Safeguarding.
- Occupational Safety and Health Administration, Publication OSHA 2236, 2002 (Revised), Materials Handling and Storage.
- National Safety Council, Publication 15250-000, 1993, Machine Guarding.
Oklahoma FACE Program
The Oklahoma Fatality Assessment and Control Evaluation (OKFACE) is an occupational fatality surveillance project to determine the epidemiology of all fatal work-related injuries and identify and recommend prevention strategies. FACE is a research program of the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research.
These fatality investigations serve to prevent fatal work-related injuries in the future by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in injury, and the role of management in controlling how these factors interact.
To contact Oklahoma State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.