
A County Road Worker Died When a Tow Rope Connection Broke Loose and Struck Him in the Head

OKFACE Report #03-OK-007-01
SUMMARY
A 61-year-old equipment operator for a county maintenance crew died on January 8, 2003, from head injuries received in a towing incident when a tow rope connection broke loose and struck him in the head. At the time of the incident, the victim was seated in a motor grader that was stuck in a ditch. Another grader had been dispatched and was attempting to pull the grader that was stuck. The tow rope was attached to a ripper tooth on the dispatched grader. During the towing process, the ripper tooth broke loose and was slung forward and struck the victim in the back of the head. Co-workers called for help via a two-way radio. An ambulance arrived at the scene within 25-30 minutes, but the injuries sustained by the worker were sufficiently severe to cause death within two hours of the incident.
Oklahoma Fatality Assessment and Control Evaluation (OKFACE) investigators concluded that to help prevent similar occurrences, employers should:
- Develop written procedures to safely tow equipment using work practices that provide protection from flying parts that could break loose during the operation.
- Train workers on safe procedures for towing equipment.
INTRODUCTION
A 61-year-old equipment operator for a county maintenance crew died on January 8, 2003, from head injuries he received that day in a towing incident. OKFACE investigators were notified of the incident, and a site visit was conducted. OKFACE investigators reviewed the death certificate, the medical examiner’s report, the Oklahoma Department of Labor report, and media reports regarding the incident. Investigators also interviewed the supervisor of the county maintenance department. The county employs about 30 people and had not had a workplace fatality for 30 years. The deceased had been employed by the county for over 19 years before the incident occurred. He had worked on this type of road project for the county continuously during his years of employment. The county has a formal safety program, including safety meetings, and written policies and practices. However, there was no written procedure for this type of operation. The safety director conducts quarterly scheduled safety meetings; additional monthly safety meetings were held on a sporadic basis. The practice being used at the time of the incident was a commonly utilized procedure for attaching tow ropes in order to pull out equipment that was stuck.
 |
| Figure 1. Grader stuck in Ditch |
INVESTIGATION
Prior to the incident, the victim was waiting on gravel and preparing to repair a tinhorn on a rural road when his grader got stuck in a roadside ditch (Figure 1). The victim radioed the office to notify them that he was stuck, and another grader was dispatched to remove the grader from the ditch. At the time of the incident, the victim was sitting in his grader with the vehicle running. Weather conditions were excellent, including a clear sky and a temperature of about 60 degrees. The two man crew that was dispatched was attempting to pull the victim’s grader out using their grader as a tow vehicle. The towing grader was equipped with ripper teeth; the purpose of the ripper teeth was to loosen road surface materials. A seven-year old military nylon tow rope, with a circumference of 10 inches was hooked on a ripper tooth on the back of the tow vehicle (Figure 2). The other end of the approximately 50-foot rope was hooked on the hitch pin on the victim’s grader. One member of the two-man crew was positioned to the side, on the ground, to watch the operation. The victim’s grader was in reverse with the victim facing away from the operation. The tow grader’s operator was facing forward, away from the operation as well. As the tow grader began to pull, the ripper tooth on which the tow rope was attached to the tow vehicle broke loose at the bottom where it was connected to the support beam. Because of the extremely tight tension on the rope, the tooth was projected toward the rear window of the victim’s grader, hit the victim in the back of the head, and continued out through the front window. The ripper tooth was approximately 18 inches long and weighed approximately 15-20 pounds (Figure 3). The two-man crew called the county maintenance office by two-way radio. A first responder arrived within 20 minutes and determined that they should wait for the ambulance to arrive before administering first aid. Another co-worker started to administer CPR while waiting for the ambulance to arrive. An ambulance arrived within 25 to 30 minutes. The victim was administered shock by an automated external defibrillator and was transported to a local hospital where he was pronounced dead one hour and forty-four minutes following the incident.
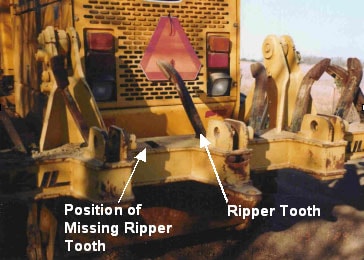 |
| Figure 2. Dispatched Grader with Ripper Tooth Missing |
 |
| Figure 3. Ripper Tooth |
CAUSE OF DEATH
The Medical Examiner listed the cause of death as blunt force injuries to the head.
RECOMMENDATIONS
Recommendation #1: Employers should develop written procedures to safely tow equipment using work practices that provide protection from flying parts that could break loose during the operation.
Discussion: There is not an OSHA standard that addresses towing procedures for motor graders. However, a safe towing procedure provides employees and bystanders with protection during towing operations. Towing procedures listed in the manufacturer’s operator manual should be followed. In this incident, the tow ropes should have been mounted to the factory equipped hitch on both graders. Instead, the ripper tooth was used, and it broke loose from its position. Employers should establish equipment towing procedures in writing to better ensure compliance.
Recommendation #2: Employers should train workers on safe procedures for towing equipment.
Discussion: Development of a written safe towing procedure, and training on that procedure is paramount in eliminating towing-related injuries. Employers should develop a scheduled training program that addresses the company’s safe towing procedures and have employees demonstrate proper procedures. In addition, actual towing operations should be monitored for compliance with the procedures.
REFERENCES
29 CFR 1910.178, Powered Industrial Trucks (General Industry)
29 CFR 1910.266, Logging operations (Special Industry)
29 CFR 1926.601, Motor vehicles (Construction)
The Oklahoma Fatality Assessment and Control Evaluation (OKFACE) is an occupational fatality surveillance project to determine the epidemiology of all fatal work-related injuries and identify and recommend prevention strategies. FACE is a research program of the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research.
These fatality investigations serve to prevent fatal work-related injuries in the future by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in injury, and the role of management in controlling how these factors interact.
To contact Oklahoma State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE website. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
Back to NIOSH FACE Web