
Guatemalan Tree-Service Worker Killed When Pulled into Brush Chipper
New York Case Report 05NY034
Summary
On May 4, 2005, a 42-year-old Guatemalan tree-service worker died after he was caught and pulled into a brush chipper. The victim was a day laborer who had worked for the tree service for approximately two weeks. On the day of the incident, the victim and his employer, the tree service owner, were trimming trees behind a residence. The owner had climbed a tree and was cutting branches and passing them down to the victim; the victim then fed the limbs through the brush chipper. After passing a few limbs to the victim, the owner heard the victim yelling and saw that he was being pulled into the chipper. The owner climbed down, discovered that the brush chipper had shut off, and that only the victim’s hand was visible in the feed chute. The owner immediately contacted the homeowner; 911 was called and emergency medical services arrived within minutes. The victim was pronounced dead at the scene.
New York State Fatality Assessment and Control Evaluation (NY FACE) investigators concluded that to help prevent similar incidents from occurring in the future, employers should:
- Ensure that workers fully understand and strictly follow the safe operating, trouble shooting, and machine maintenance procedures recommended by the manufacturers when operating brush chippers;
- Train workers in safe and proper feeding technique to avoid the hazard of being pulled into an operating brush chipper;
- Ensure that the safety instructions and training are provided in a language that workers are able to comprehend;
- Designate another employee as a safety watch to assist the brush chipper operator and;
- Ensure that the area in front of the infeed hopper is free of tripping hazards.
Additionally:
- Brush chipper manufacturers should install additional safety features including emergency shut-off devices on brush chippers.
Introduction
On May 4, 2005, a 42-year-old Guatemalan tree-service worker died after he was caught and pulled into a brush chipper. NY FACE staff learned of the incident on May 5 through a newspaper article. NY FACE investigators met with the Occupational Safety and Health Administration (OSHA) compliance officer who had investigated the incident to collect information related to the fatal event. In preparation for the report, NY FACE staff also contacted the manufacturer of the brush chipper that was involved in the fatal incident, and reviewed news reports, police investigation records and the death certificate. No site visit or employer interview was conducted.
The victim’s employer was a self-employed tree-service owner. The tree service had been in business for ten to twelve years. The owner hired the victim, his only employee, through a contact referral approximately two weeks before the incident.
The victim was a day laborer, having arrived in the United States approximately ten years ago from Guatemala. The victim spoke Spanish and reportedly neither spoke nor understood English well. Prior to working for the tree-service, the victim had assorted jobs such as lawn mowing and fence repair. This was the tree-service’s first fatality.
Back to Top
Investigation
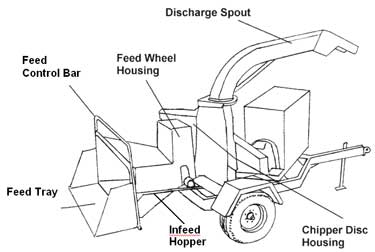
On May 4, 2005, the victim and his employer were trimming trees behind a residence. A brush chipper was used to grind up the cuttings. The brush chipper, purchased by the tree-service owner ten year ago, was a hand-fed portable model (Figure 1) and could process materials up to 12 inches in diameter. The machine consists of a feed mechanism, a rotating chipper drum, and a power plant. Tree cuttings are fed into the machine through a feed chute, or infeed hopper. At the end of the chute, two feed wheels are arranged one above the other to pull material into the chute. The feed wheels grab the tree cuttings and forces them into the knives mounted inside on a rotating drum. The drum operates at a high rate of speed and pushes the chipped wood through a discharge spout for removal and transport.
|
|
Figure 1. Diagram of wood chipper model involved in incident. (Courtesy of National Institute for Occupational Safety and Health, FACE Report 98-13).
|
The brush chipper is equipped with a feed control bar (a.k.a., safety bar) located around the opening of the feed chute. The control bar operates the feed wheels and has three positions: feed, off (neutral), and reverse. An operator pulls the bar toward the feed chute to activate the feed wheel rotation and pull the material into the chipper, places the bar in the middle (neutral) to stop the feed wheels, or pushes the bar toward the chipper to reverse the feed wheels and back the material out of the chipper. Since the feed control bar was around the infeed hopper, a worker caught in the feed mechanism may not be able to activate it.
The owner, who spoke only English, reportedly explained basic chipper operations to the victim, including how to run and stop the machine, prior to letting the victim operate the chipper. The victim had operated the chipper for the tree-service approximately three times before the day of the incident.
The incident occurred at approximately 11:00 a.m. At the time of the incident, the owner had climbed up into a tree and was cutting branches and passing them down to the victim who then fed the limbs through the brush chipper. The branches being fed were reportedly smaller than 10 inches in diameter, so there were no oversized (larger than 12 inches in diameter) materials being fed into the machine. The victim was wearing gloves and a baseball hat at the time of the incident; it is unknown what other clothing he was wearing.
After passing a few limbs to the victim from the tree, the owner heard the victim yell and saw that he was being pulled into the chipper. As the employer was the only witness and was up in the tree at the time of the incident, the exact manner in which the victim was caught and pulled into the chipper is unknown.
The owner climbed down the tree, discovered that the wood chipper had shut off, and that only the victim’s hand was visible in the feed chute. The owner immediately contacted the homeowner; 911 was called and emergency medical services arrived within minutes. The victim was pronounced dead at the scene.
Back to Top
Cause of Death
The official cause of death was listed on the death certificate as exsanguination from trauma.
Recommendations/Discussion
Recommendation #1: Employers should ensure that workers fully understand and strictly follow the safe operating, trouble shooting, and machine maintenance procedures recommended by the manufacturers when operating brush chippers.
Discussion: Employers should require brush chipper operators to review the manufacturer’s operating instructions. Operators and other employees assisting with brush chipper tasks should be instructed on safe work practices and potential or existing hazards unique to the job assignment. Workers should receive training on chipper safety devices and controls, proper operation, feeding, starting, shutdown, and emergency procedures. Workers should also be familiar with what types of material should not be fed into the machine, the proper procedure for clearing jams, and personal protective equipment that should be used.
Employers should also instruct workers to follow safe procedures recommended by the manufacturer when clearing jams, trouble shooting, or performing routine maintenance on brush chippers. Before attempting any type of maintenance, the brush chipper should always be turned off. The cutting rotor operates at a powerful and high speed with a great amount of inertia and the chipper disc will coast for several minutes after the engine is shutdown. Workers should not attempt any type of maintenance until all internal machine parts have come to a complete stop.
Recommendation #2: Employers should train workers in safe and proper feeding techniques to avoid the hazard of being pulled into an operating brush chipper.
Discussion: Workers without proper training are at great risk of being pulled into and through the chipper knives. This can occur if the worker loses balance and falls forward into the feed chute, reaches too far into the feed mechanism, or becomes entangled or pushed by branches and limbs that are being pulled into the chipper. The risk can be minimized if workers are trained in safe feeding techniques that include the following:
- never place hands or feet inside the feed chute;
- always stand to the side of the infeed hopper when feeding the brush chipper. This minimizes the risk of entanglement in branches and allows quick access to the feed control bar to turn off or reverse the feeding mechanism. (Because of differences among machines, the manufacturer’s operating manual should be consulted for guidance. Safe feeding of some disc-type chippers requires the worker to be on the right side);
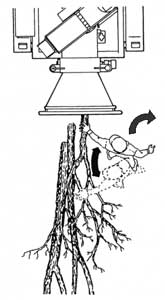
- immediately walk away once the machine has grabbed the material and been fed through the chipper knives (see Figure 2);
- feed brush and limbs into the infeed hopper butt end first; and
- lay short/small material on top of longer material to feed or use a push paddle to push short or thorny brush through the infeed hopper.
|
|
Figure 2. Safe feeding pathway: material fed from side, operator walks away immediately following feeding. (Courtesy of Michigan Occupational Safety and Health Administration, Pub OSC-6125).
|
Recommendation #3: Employers should ensure that the safety instructions and training are provided in a language that workers are able to comprehend.
If a language barrier exists, as in this incident, employers should ensure that the chipper safety training is provided in a language and at a literacy level that is fully understood by the workers before assigning the task. An interpreter should be used if workers require assistance in understanding safety training.
Recommendation #4: Employers should designate another employee as a safety watch to assist the brush chipper operator.
Discussion: A safety watch is mandated in many high-risk occupations to help prevent injuries. When the brush chipper is in operation, at least one worker in addition to the operator should be placed in the immediate vicinity of the work area and in close contact with the operator. In this incident, a designated safety watch stationed near the chipper may have been able to intervene verbally if the victim had been observed feeding material from a hazardous position or may have been able to inactivate the chipper before the victim made contact with the chipper blades.
Recommendation #5: Employers should ensure that the area in front of the infeed hopper is free of tripping hazards.
Discussion: Workers feeding material into brush chippers are at risk of being fed through the chipper knives if they fall into the infeed hopper or become entangled in branches feeding into the machine. Employers should ensure that the area in front of the infeed hopper is free of branches, logs, vines, rocks, and other tripping hazards to help prevent workers from tripping or falling into the chipper feed mechanism.
Recommendation #6: Brush chipper manufacturers should install additional safety features including emergency shut-off devices on brush chippers.
Discussion: Newer brush chippers are equipped with additional safety features besides the feed control bar. For example, a newer model of the chipper that was involved in the incident now has a new safety emergency shut-off device, termed “Last Chance Stop”. The Last Chance Stop, located inside the infeed hopper is a cable assembly connected to the feed control bar. By pulling the cable, the operator can reverse the feed wheels from inside the hopper. Technology is emerging which may allow the use of electronic sensors to eliminate machine-related injury. In one example of this technology, the worker would wear gloves made of metal-impregnated material. The presence of the workers’ hand near the feed hopper would be detected by a metal detector mounted at the opening. The detected signal could then be used to stop the feed wheels.
Back to Top
References
-
CDC/NIOSH. NIOSH Hazard ID. Injury Associated with Working Near or Operating Wood Chippers. DHHS (NIOSH) Publication No. 99-145, August 1999.
-
NIOSH FACE Program. Groundsman On Tree Trimming Crew Caught In Wood Chipper, In-house Report No. 1998-13.
-
NIOSH FACE Program. Fourteen-Year-Old Youth Pulled Into Operating Wood Chipper, In-house Report No. 2000-21.
-
American National Standards for Tree Care Operations—Pruning, Trimming, Repairing, Maintaining, and Removing Trees, and Cutting Brush—Safety Requirements”, ANSI z133.1-1994. American National Standards Institute, Inc, New York, New York.
-
University of California, Agriculture and Natural Resources, Environmental Health and Safety. Safety Note #91: Brush Chipper Safety. November 2005.
-
California FACE Report No. 00CA010. A tree trimmer dies when pulled into in a brush chipper, http://www.cdph.ca.gov/programs/ohb-face/Documents/00ca010.pdfpdf iconexternal icon (Link updated 4/1/2009)
-
Michigan Occupational Safety and Health Administration, Consultation Education and Training Division. Onsite Consultation Abatement Method Advice for: Brush Chipper In Feed and Cutter Pinch Points. OSC-6125, Revised June 2005.
New York FACE Program
The Fatality Assessment and Control (FACE) program is one of many workplace health and safety programs administered by the New York State Department of Health (NYS DOH). It is a research program designed to identify and study fatal occupational injuries. Under a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), the NYS DOH FACE program collects information on occupational fatalities in New York State (excluding New York City) and targets specific types of fatalities for evaluation. NYS FACE investigators evaluate information from multiple sources. Findings are summarized in narrative reports that include recommendations for preventing similar events in the future. These recommendations are distributed to employers, workers, and other organizations interested in promoting workplace safety. The FACE program does not determine fault or legal liability associated with a fatal incident. Names of employers, victims and/or witnesses are not included in written investigative reports or other databases to protect the confidentiality of those who voluntarily participate in the program.
To contact New York State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.